trimethoprim-sulfamethoxazole uses
Reading File
Finding Sources
Searching PubMed
trimethoprim-sulfamethoxazole clinical uses indications
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a thorough answer. Let me compile the comprehensive response.
Trimethoprim-Sulfamethoxazole (TMP-SMX / Cotrimoxazole)
Mechanism of Action
TMP-SMX blocks two sequential steps in bacterial folate synthesis, creating a synergistic (often bactericidal) effect:
- Sulfamethoxazole inhibits dihydropterate synthetase, blocking incorporation of PABA into dihydrofolic acid
- Trimethoprim inhibits dihydrofolate reductase, blocking conversion of dihydrofolate to tetrahydrofolate
The combination is formulated in a 1:5 ratio (TMP:SMX), which gives a plasma concentration ratio of 1:20 - optimal for in vitro synergy. Neither drug alone is reliably bactericidal; together, they usually are.
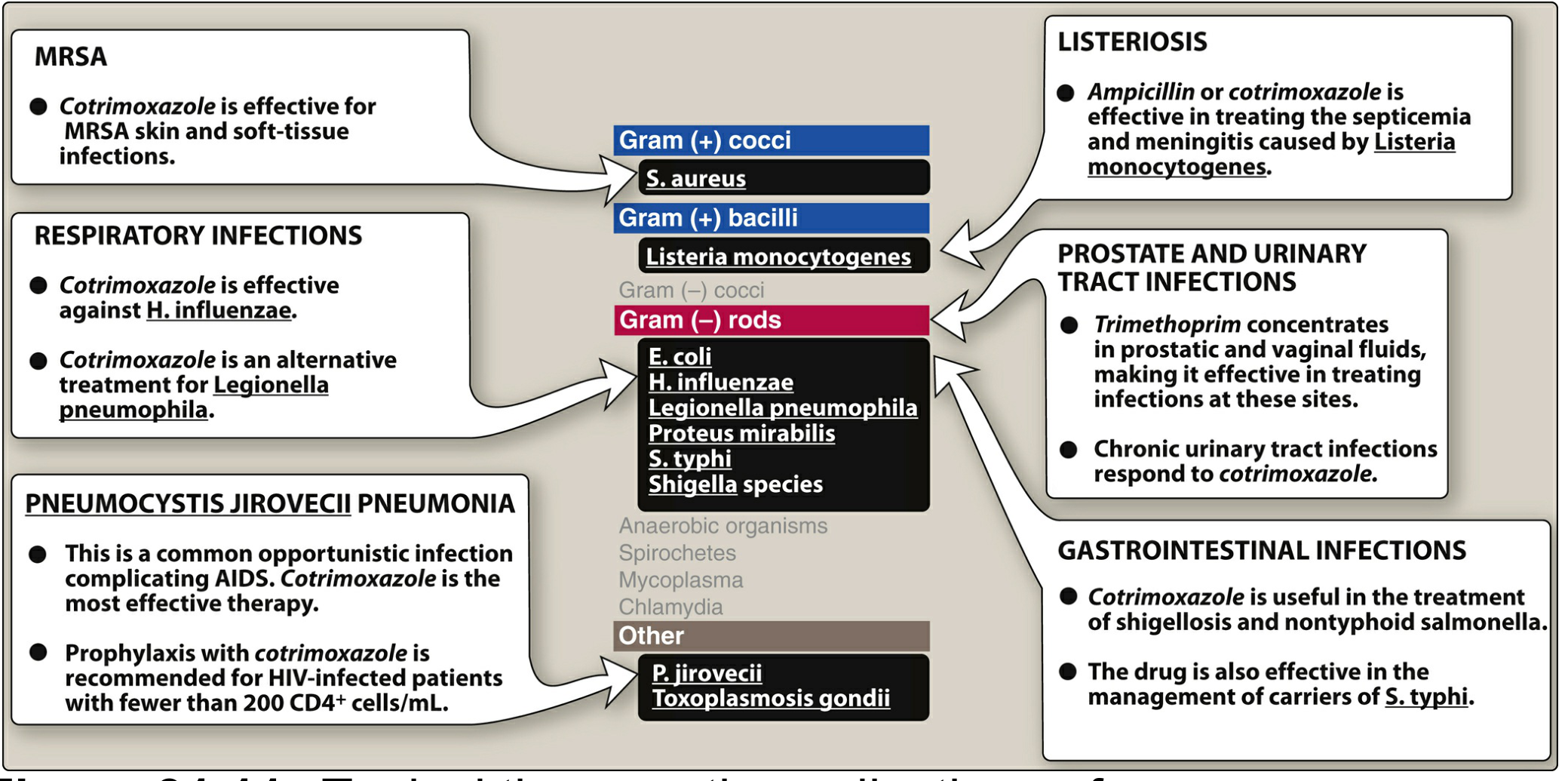
Antibacterial Spectrum
| Category | Organisms Covered |
|---|---|
| Gram-positive cocci | S. aureus (MSSA and CA-MRSA) |
| Gram-positive bacilli | Listeria monocytogenes |
| Gram-negative cocci | Neisseria gonorrhoeae (resistance now common) |
| Gram-negative rods | E. coli, H. influenzae, Proteus mirabilis, Shigella, Salmonella/S. typhi, Legionella pneumophila |
| Other gram-negatives | Stenotrophomonas maltophilia, Nocardia spp. |
| Fungi/opportunists | Pneumocystis jirovecii, Toxoplasma gondii |
Not active against: anaerobes, Pseudomonas aeruginosa, Mycoplasma, Chlamydia, spirochetes.
Clinical Uses
1. Urinary Tract Infections (UTIs)
- Most common use - treats uncomplicated and complicated UTIs caused by susceptible E. coli, Klebsiella, Proteus
- Standard dose: 1 DS tablet (160/800 mg) every 12 hours
- Prophylaxis for recurrent UTIs in women: 1 SS tablet (80/400 mg) three times weekly
- Trimethoprim concentrates in prostatic and vaginal fluids (being more lipid-soluble) - effective for bacterial prostatitis
2. Pneumocystis jirovecii Pneumonia (PCP)
- Drug of choice for both treatment and prophylaxis
- Treatment: High-dose IV or oral TMP 15-20 mg/kg/d (dosed on trimethoprim component)
- IV formulation used for moderate-to-severe PCP
- Prophylaxis: 1 DS tablet daily or three times weekly; indicated in HIV patients with CD4 < 200 cells/mL
3. Skin and Soft Tissue Infections (SSTIs)
- Effective for community-acquired MRSA SSTIs (furunculosis, cellulitis, abscesses)
- Standard DS dosing every 12 hours
- Bone and joint MRSA infections: 8-10 mg/kg/d of the TMP component
4. Respiratory Tract Infections
- Haemophilus influenzae, Moraxella catarrhalis, susceptible K. pneumoniae
- Alternative treatment for Legionella pneumophila
- Not active against Mycoplasma pneumoniae or Streptococcus pyogenes (unreliable)
5. Gastrointestinal Infections
- Shigellosis (bacillary dysentery) - treatment of choice if susceptible
- Typhoid fever / Salmonella carriers - alternative agent
- Nontyphoid Salmonella infections
- Cyclospora cayetanensis and Cystoisospora belli (Isospora) infections - TMP-SMX is the drug of choice for both treatment and long-term suppression in immunocompromised patients
6. Nocardiosis
- Drug of choice for Nocardia spp. infections (pulmonary, disseminated, CNS)
- High-dose, prolonged treatment required
7. Stenotrophomonas maltophilia
- One of the few reliable agents against this intrinsically multidrug-resistant organism
8. Listeriosis
- Alternative to ampicillin for Listeria monocytogenes septicemia and meningitis, especially in penicillin-allergic patients
9. Other Uses
- Traveler's diarrhea (where susceptibility is maintained)
- Toxoplasmosis prophylaxis in HIV/immunocompromised patients (TMP-SMX covers this at PCP prophylaxis doses)
- Whipple's disease (alternative)
- Chronic granulomatous disease - long-term prophylaxis against bacterial infections
- Wegener's granulomatosis (GPA) - used for relapse prevention
Formulations and Doses
| Formulation | Composition | Common Use |
|---|---|---|
| Single-strength (SS) tablet | TMP 80 mg + SMX 400 mg | UTI prophylaxis |
| Double-strength (DS) tablet | TMP 160 mg + SMX 800 mg | Most adult infections |
| IV solution | TMP 80 mg + SMX 400 mg per 5 mL | Severe PCP, bacteremia |
| Pediatric tablet | TMP 20 mg + SMX 100 mg | Pediatric dosing |
Pediatric dose: TMP 8 mg/kg/day + SMX 40 mg/kg/day divided every 12 hours (for shigellosis, UTI, otitis media).
Dose adjustment: Reduce by half when creatinine clearance is 15-30 mL/min. Avoid if CrCl < 15 mL/min (if alternatives exist).
Adverse Effects
| Category | Effects |
|---|---|
| GI | Nausea, vomiting, diarrhea (most common) |
| Hypersensitivity | Rash, urticaria, Stevens-Johnson syndrome (sulfonamide component) |
| Hematologic | Leukopenia, thrombocytopenia, granulocytopenia, megaloblastic anemia (with prolonged use or folate deficiency) |
| Renal/Electrolytes | Nephrotoxicity, hyperkalemia, hyponatremia (more common at high doses; TMP blocks potassium secretion in collecting duct) |
| Hepatic | Elevated transaminases (uncommon) |
Key Drug Interactions
- Warfarin - TMP-SMX inhibits CYP2C9, potentiating anticoagulant effect
- Phenytoin - increased phenytoin levels (reduced metabolism)
- Methotrexate - additive folate antagonism, increased toxicity
- ACE inhibitors/potassium-sparing diuretics - additive hyperkalemia risk (TMP blocks renal K+ secretion)
- Cyclosporine - may increase nephrotoxicity
Resistance
- TMP resistance: due to reduced cell permeability, overproduction of dihydrofolate reductase, or plasmid-encoded resistant enzymes spread via transposons
- Combined resistance is less common than resistance to either drug alone (requires simultaneous resistance to both)
- E. coli resistance now ~25-30% in many regions - limits empiric use for upper UTIs and pneumonia
- Resistance in pneumococci is also significant
Sources: Harrison's Principles of Internal Medicine 22E, p. 1221 | Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 1301-1302 | Lippincott Illustrated Reviews: Pharmacology, pp. 1037-1039 | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.