Junctional bradycardia with syncope
Reading File
Finding Sources
Finding Sources
Searching PubMed
junctional bradycardia syncope management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
junctional bradycardia ECG rhythm strip
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information. Let me compile the complete answer.
Junctional Bradycardia with Syncope
Definition & Mechanism
The AV junction (AV node + His bundle) is the heart's secondary pacemaker, firing at an intrinsic rate of 40–55 bpm when the sinus node fails to suppress it. A junctional escape rhythm emerges as a protective mechanism whenever the sinus rate falls below this threshold — for example, when sinus bradycardia drops below ~40 bpm or during sinus arrest, sinoatrial exit block, or high-degree AV block.
Syncope results from cerebral hypoperfusion. Either extreme of ventricular rate can depress cardiac output to the point of critical hypotension. In junctional bradycardia, the rate may be too slow to maintain adequate blood pressure, or there may be a prolonged pause before the escape rhythm develops — both can precipitate loss of consciousness. — Fuster & Hurst's The Heart, 15th Ed.
ECG Recognition
Junctional escape beats / rhythm:
- Narrow QRS complexes (normal intraventricular conduction)
- No preceding P wave, or retrograde P waves (inverted in II, III, aVF) that may appear before, during, or after the QRS
- Rate 40–55 bpm (slower idioventricular escape = wide QRS, rate 15–40 bpm)
Classic scenario — sinus arrest with escape beats:
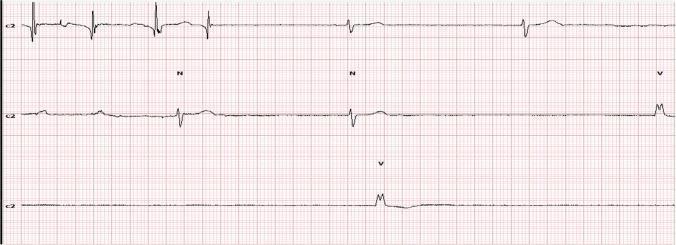
Rhythm strip: normal sinus rhythm interrupted by prolonged pause, then junctional escape (N) and idioventricular escape (V) beats — a classic syncope substrate.
Complete heart block with junctional escape (12-lead):
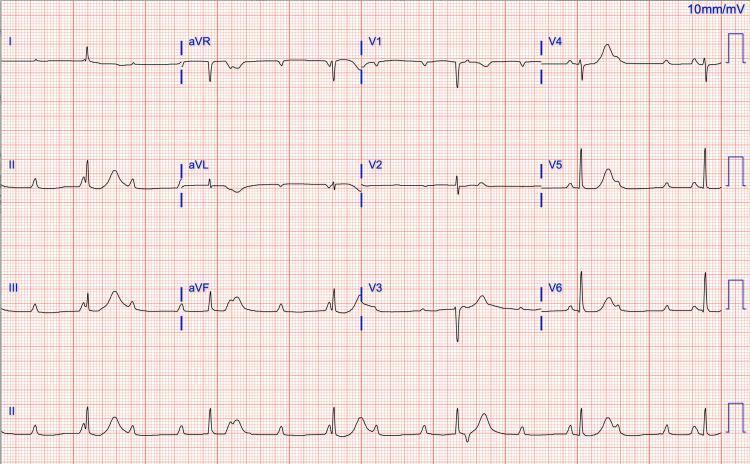
Third-degree AV block: P waves march through QRS complexes at a faster rate (AV dissociation). Junctional escape rhythm: narrow QRS at ~30–40 bpm.
Causes
Junctional bradycardia with syncope arises from several overlapping etiologies: — Goldman-Cecil Medicine, Table 51-2 & 51-3
| Category | Examples |
|---|---|
| Degenerative | Idiopathic fibrocalcific degeneration (most common) |
| Ischemia/Infarction | Acute inferior MI (RCA supplies AV node) |
| Sick Sinus Syndrome | Bradycardia-tachycardia syndrome — syncope at SVT termination due to overdrive suppression of junctional pacemakers |
| Medications | β-blockers, non-DHP calcium channel blockers, digoxin, amiodarone, sotalol, SSRIs, opioids, cholinesterase inhibitors |
| Infiltrative | Amyloidosis, sarcoidosis, hemochromatosis |
| Infectious | Lyme disease (common reversible cause), endocarditis |
| Metabolic | Hypothyroidism, hyperkalemia, hypothermia, hypoxia |
| Autonomic | Vasovagal, carotid sinus hypersensitivity, high vagal tone |
| Iatrogenic | Post-valve surgery, post-AV nodal ablation, pulmonary artery catheter |
| Congenital | Congenital complete heart block (may remain asymptomatic with exercise-responsive junctional escape) |
Key clinical pearl: The tachy-brady syndrome (a subset of sick sinus syndrome) produces syncope specifically at the termination of SVT — overdrive suppression silences both the sinus node and junctional pacemakers, leading to a prolonged pause before any escape rhythm recovers. — Fuster & Hurst's The Heart
Clinical Presentation
- Syncope or near-syncope (abrupt, without prodrome in arrhythmic syncope)
- Fatigue, exertional dyspnea, dizziness
- Third-degree AV block may also present with elevated BP (peripheral vasoconstriction) and renal insufficiency (reduced CO)
- Congenital AV block with a good junctional escape that accelerates during exercise may remain asymptomatic for decades — Goldman-Cecil
Diagnosis
- 12-lead ECG — first step; identifies rhythm, AV relationship, QRS width
- 24-hour Holter or prolonged loop recorder — for paroxysmal/intermittent symptoms
- Implantable loop recorder — for infrequent syncope (the gold standard for symptom-rhythm correlation)
- Electrophysiology (EP) study — when non-invasive monitoring is inconclusive, especially if bifascicular block is present
- Echocardiogram — evaluate structural disease
- Exercise test — chronotropic incompetence, ischemia-induced block
- Lyme serology, TSH, electrolytes — reversible causes
- Medication review — always exclude drug-induced bradycardia first
Management
Acute / Emergent (symptomatic with hemodynamic compromise)
| Intervention | Details |
|---|---|
| Atropine | 1 mg IV q3–5 min, max 3 mg total (first-line for most bradycardias; ineffective post-cardiac transplant) |
| Isoproterenol infusion | 1–2 µg/min; also used post-transplant |
| Dopamine/Epinephrine infusion | Second-line if atropine fails |
| Transcutaneous pacing | Emergency bridge; rarely needed for isolated sinus bradycardia, more often required in high-degree AV block |
| Transvenous temporary pacing | If block is suspected infra-His or intra-His (wide QRS escape, suspected His-Purkinje disease) |
Note: Atropine is often unhelpful or paradoxically worsening in infra-nodal block (His-Purkinje disease) because it may speed the atrial rate without improving AV conduction, increasing the block ratio.
Reversible Causes — Treat First
- Withdraw offending drugs
- Treat hypothyroidism, correct electrolytes/hypothermia
- IV ceftriaxone for Lyme-mediated heart block
Definitive: Permanent Pacemaker Implantation
Permanent pacing is indicated in: — Goldman-Cecil; Braunwald's Heart Disease
- Sick sinus syndrome with syncope (symptomatic correlation confirmed)
- High-degree (Mobitz II second-degree) or third-degree AV block — especially if wide QRS (infra-His disease), symptoms present, or QT prolongation (torsades de pointes risk)
- Bifascicular block with prolonged PR — substantial risk of progressing to complete heart block
- Congenital complete AV block — when symptomatic or functional impairment is present
- Asymptomatic narrow-QRS junctional escape with third-degree AV block may be observed only if QT is normal and the patient is young with congenital block
Post-AV node ablation: pacemaker is set at 80 bpm for ≥6 weeks to prevent QT prolongation and torsades de pointes. — Goldman-Cecil
BRASH Syndrome (Notable Cause)
A systematic review (PMID 36842470) highlights BRASH syndrome — Bradycardia, Renal failure, AV nodal blockade, Shock, Hyperkalemia — as an underrecognized cause of severe junctional bradycardia and syncope, especially in patients on AV-nodal blocking drugs with superimposed renal dysfunction. Hyperkalemia synergistically potentiates the bradycardic effect. Management targets all five components simultaneously.
Summary Algorithm
Junctional Bradycardia + Syncope
↓
Is the patient hemodynamically unstable?
YES → Atropine IV → Temporary pacing → Identify & reverse cause
NO → 12-lead ECG + monitoring + Holter/ILR
↓
Reversible cause found?
YES → Treat cause (drugs, Lyme, hypothyroid, electrolytes)
NO → EP evaluation → Permanent pacemaker (if Sick Sinus or high-degree AV block)
Key references: Fuster & Hurst's The Heart (15th Ed.) · Goldman-Cecil Medicine · Braunwald's Heart Disease · Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.