Cholecystectomy
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
cholecystectomy laparoscopic outcomes
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Cholecystectomy
Cholecystectomy is surgical removal of the gallbladder and is one of the most commonly performed abdominal operations worldwide - over 750,000 are performed per year in the United States alone. The first successful open cholecystectomy was performed by Carl Langenbuch in 1882; laparoscopic cholecystectomy was introduced by Philippe Mouret in France in 1987 and quickly became the standard of care.
1. Indications
Laparoscopic cholecystectomy is the treatment of choice for:
- Symptomatic cholelithiasis (biliary colic) - the most common indication
- Acute cholecystitis - acute inflammation of the gallbladder
- Cholecystitis complications - empyema, gangrene, perforation
- Gallstone pancreatitis - following resolution of the acute episode
- Choledocholithiasis - common bile duct (CBD) stones (often combined with ERCP)
- Gallbladder polyps >10 mm (or symptomatic/growing)
- Porcelain gallbladder (selected cases)
- Biliary dyskinesia (ejection fraction <35% on HIDA scan with symptoms)
2. Preoperative Assessment
Workup includes:
- Full blood count, renal and liver function tests, prothrombin time
- Abdominal ultrasound (primary imaging)
- ECG and chest X-ray if medically indicated
CBD stone risk stratification (Bailey & Love):
| Risk | History | LFTs | CBD diameter (USG) | Action |
|---|---|---|---|---|
| Low (2-3%) | No cholangitis/pancreatitis | Normal | ≤6 mm | None |
| Medium (20-40%) | Present | 2× normal | 8-10 mm | MRCP ± ERCP |
| High (50-80%) | Present + jaundice | 2× normal | ≥10 mm | MRCP ± ERCP |
Prophylaxis:
- Second-generation cephalosporin at induction (routine for complicated disease; selectively for uncomplicated biliary pain)
- DVT prophylaxis: subcutaneous heparin + antiembolic stockings
Predictors of difficult cholecystectomy (Bailey & Love, Table 71.3):
- Male sex, age >65, prior attacks, previous upper abdominal surgery
- Morbid obesity, high ASA score
- Thick-walled (>4-5 mm) or contracted gallbladder on imaging
- Gangrenous gallbladder, Mirizzi's syndrome, cirrhosis, cholecystoenteric fistula
3. Contraindications
Absolute contraindications to laparoscopic approach:
- Hemodynamic instability
- Uncontrolled coagulopathy
- Frank peritonitis
Relative (may require open conversion):
- Severe COPD or CHF (ejection fraction <20%) - may not tolerate CO₂ pneumoperitoneum
- Formerly listed contraindications - acute cholecystitis, obesity, pregnancy, cirrhosis, prior upper abdominal surgery - are now considered risk factors, not absolute contraindications
4. Laparoscopic Cholecystectomy - Technique
Patient positioning and access
- Patient supine; surgeon stands at patient's left (or between legs in split-leg positioning)
- Pneumoperitoneum established with CO₂ via Veress needle (closed) or Hasson technique (open)
- Port placement: Camera port at supraumbilical region; 10-12 mm epigastric port; 5 mm right midclavicular; 5 mm right flank
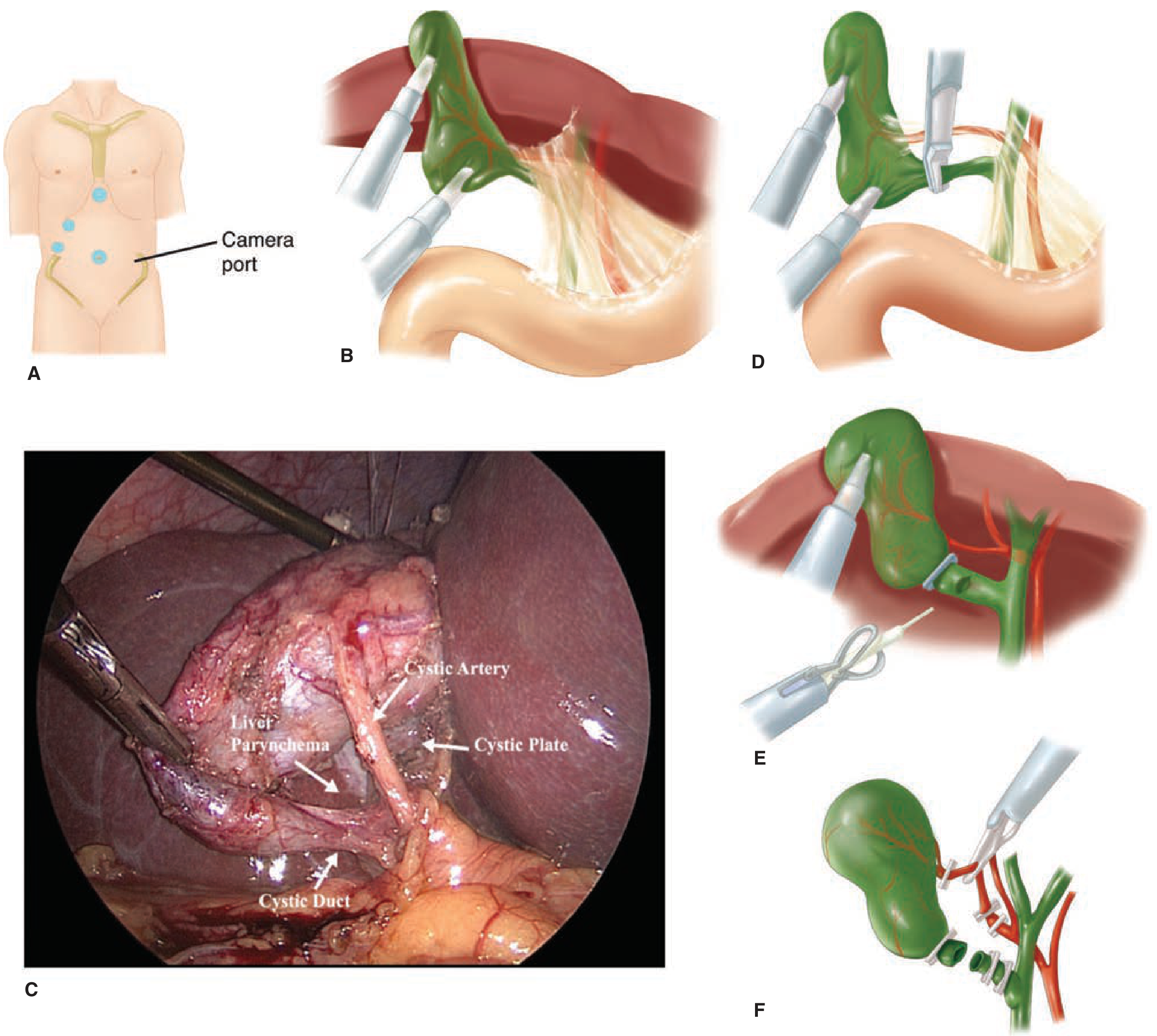
Key operative steps
1. Retraction
- Fundus retracted toward patient's right shoulder (over liver edge)
- Infundibulum retracted inferolaterally toward right iliac fossa
- This opens the hepatocystic (Calot's) triangle and increases the angle between the cystic duct and CBD
2. Dissection of Calot's triangle
- Peritoneum on both anterior and posterior aspects of the triangle divided
- Fat, areolar tissue, and fibrous tissue cleared
- Identify the cystic duct and cystic artery (cystic artery runs parallel to, often posterior to, cystic duct; passes behind Calot's/Lund's node)
3. Critical View of Safety (CVS) - the most important safety step
- Hepatocystic triangle cleared of ALL fat and fibrous tissue
- Lower one-third of gallbladder separated from the liver (cystic plate exposed)
- Two and only two structures seen entering the gallbladder (cystic duct + cystic artery)
- CVS may be documented photographically/video
4. Clipping and division
- Two clips placed at the base + one clip on gallbladder side for both cystic duct and cystic artery
- Structures divided between clips
- For a very dilated cystic duct: endoloop, laparoscopic stapler, or suture closure
5. Gallbladder dissection from the liver bed
- Electrocautery dissection; cystic plate left attached to liver (avoids liver sinus bleeding and bile leak)
- Gallbladder removed through epigastric or umbilical port (retrieval bag recommended)
6. Final inspection
- Check for bleeding, bile staining, and secure clip placement before final removal
- Drain placed only if severe inflammation, gangrene, or anticipated bile/blood collection
Intraoperative cholangiogram (IOC)
- Optional but valuable: detects CBD stones, identifies aberrant ductal anatomy
- Routine vs. selective IOC remains debated
- Indocyanine green (ICG) fluorescence cholangiography - newer modality that improves real-time biliary tree visualization and reduces BDI risk (Bailey & Love)
- When in doubt about anatomy, IOC is always warranted
5. Open Cholecystectomy
Performed when laparoscopic approach is contraindicated or conversion is required (elective conversion ~5%; emergent/complicated cases 10-30%).
- Incision: Right subcostal (Kocher's) or midline laparotomy; right upper transverse incision
- Same surgical principles: identify and achieve CVS; clip and divide cystic duct and artery
- Top-down (fundus-first) dissection is common in open approach
- Partial cholecystectomy reserved for cases where complete anatomy cannot be safely identified - remove as much mucosa as possible, close cystic duct stump, drain widely
6. Complications
Intraoperative
| Complication | Notes |
|---|---|
| Bile duct injury (BDI) | Most serious; 1 in 200-600 open cases; rate with laparoscopic historically higher but improving with modern technique |
| Vascular injury | Right hepatic artery is at risk (often injured alongside BDI) |
| Bowel injury | Rare |
Postoperative - Bile duct injury patterns (Sleisenger & Fordtran):
- Complete occlusion - rapid postop jaundice (clips misplaced on CBD)
- Bile leak/ascites - from cystic duct stump, duct of Luschka, or transection; presents with bile ascites, biloma, subhepatic collection
- Partial obstruction/stricture - intermittent pain, jaundice, or cholangitis, usually within 2 years
Management of BDI:
- Early: control subhepatic infection (percutaneous drainage), biliary drainage (ERCP or transhepatic)
- Definitive: complete cholangiography (ERCP + transhepatic) to define anatomy
- Surgical repair: resection of damaged duct + Roux-en-Y hepaticojejunostomy (best results)
General postoperative complications
- Wound infection, seroma (lower rates with laparoscopic vs open)
- Cardiopulmonary complications
- Urinary retention/infection, atelectasis
- DVT/PE
Mortality: ~0.1% for laparoscopic cholecystectomy (Schwartz's)
"Red flag" signs during surgery (stop and reassess):
- Failure of timely dissection progress
- Anatomical disorientation
- Difficulty visualizing the operative field
- → Seek a second opinion, consider conversion, or perform a partial/subtotal cholecystectomy
7. Post-op Care and Recovery
Laparoscopic cholecystectomy:
- Most patients discharged same day or within 24 hours
- Resume diet quickly (often within hours)
- Return to normal activities within 1-2 weeks
- Incision site care; no heavy lifting for ~2 weeks
Open cholecystectomy:
- Hospital stay 3-5 days typically
- Longer recovery (4-6 weeks to full activity)
- Higher wound complication rate
Surveillance: Post-op LFTs if jaundice or pain develops - evaluate for retained CBD stones or BDI.
8. Special Situations
Common Bile Duct Exploration (CBDE)
- Can be performed at the time of cholecystectomy for known/intraoperatively detected CBD stones
- Approaches: saline flush + IV glucagon (small stones), wire basket under fluoroscopy, flexible choledochoscope for direct retrieval
- Very dilated CBD may require choledochotomy (closed primarily or over T-tube)
Cholecystectomy in pregnancy
- Safest in second trimester
- Laparoscopic approach is appropriate (a 2024 network meta-analysis, PMID 39406972, supports surgical management)
Robotic cholecystectomy
- Growing evidence base; a 2025 meta-analysis (PMID 41354898) compared robotic vs. laparoscopic approaches - robotic shows comparable outcomes, potentially lower conversion rates
Sources:
- Schwartz's Principles of Surgery, 11e (Chapter 32)
- Bailey and Love's Short Practice of Surgery, 28e (Chapter 71)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Chapter 66)
This is a shared conversation. Sign in to Orris to start your own chat.