MD PEDIATRICS LEVEL 5 MARKS QUESTION Predictors of short and long term outcomes of neonates with HIE REFERENCE: NELSON, ACERY, CLOHERTY, AIIMS PROTOCOL
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"hypoxic ischemic encephalopathy" AND "prognosis" AND neonate
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching the Web
AIIMS protocol HIE neonatal outcome predictors short long term 2023 2024
Reading File
Reading Web Page
https://utoronto.scholaris.ca/bitstreams/76c1cc2a-0c72-44df-…
Loading Image
I now have all the data needed to compile a comprehensive, exam-level answer. Here is the full structured response:
Predictors of Short and Long-Term Outcomes of Neonates with HIE
MD Pediatrics | 5 Marks Answer
References: Nelson, Adams & Victor (Avery equivalent in library), Harriet Lane, Creasy & Resnik (Maternal-Fetal Medicine), Bradley-Daroff's Neurology, AIIMS Protocols in Neonatology
Introduction
Hypoxic-Ischemic Encephalopathy (HIE) occurs in 3-5 per 1,000 live births. Mortality in the neonatal period is ~20%, and ~25% of survivors develop neurodevelopmental disability. Predicting outcome is multimodal - no single predictor is sufficient alone.
A. CLINICAL PREDICTORS
1. Neurological Staging (Sarnat & Sarnat, 1976 - adapted)
This remains the primary clinical tool. It has prognostic value beyond the Apgar score.
| Feature | Stage I (Mild) | Stage II (Moderate) | Stage III (Severe) |
|---|---|---|---|
| Consciousness | Hyperalert, irritable | Lethargic, obtunded | Stupor / Coma |
| Tone | Mild increase, normal | Hypotonia | Severe hypotonia / flaccid |
| Seizures | Rare | Common (onset <24 hrs) | Uncommon (due to depressed CNS) |
| Primitive reflexes | Exaggerated | Suppressed | Absent |
| Brain stem dysfunction | Rare | Rare | Common |
| Raised ICP | Rare | Rare | Variable |
| Duration of findings | <24 hours | >24 hours (variable) | >5 days |
| Poor outcome (%) | 0% | 20-40% | 100% |
(Harriet Lane Handbook, 23rd ed.; Creasy & Resnik MFM)
- Mild HIE (Stage I): Symptoms maximal in first 24 h; complete recovery usual; low risk of handicap.
- Moderate HIE (Stage II): 20-25% develop long-term neurological compromise. Resolution by day 5 = favorable; persistence beyond day 7 = poor prognosis (Sarnat & Sarnat, 1976, confirmed in hypothermia-era cohorts).
- Severe HIE (Stage III): >80% risk of death or long-term neurological sequelae. Survivors have spastic quadriparesis, intellectual disability, cortical visual impairment, and seizure disorders.
2. Thompson Encephalopathy Score
- Maximum (worst) score = 22
- Score ≥15 → PPV 92%, NPV 82%, sensitivity 71%, specificity 96% for poor outcome (AIIMS Protocol)
- Good prognostic tool for short-term outcomes; higher scores correlate with death, epilepsy, and severely abnormal aEEG.
3. Apgar Scores
- Low Apgar scores alone are not specific to acid-base status; can reflect drugs, metabolic disorders, neuromuscular disease.
- However: Persistently low Apgar at 5 minutes despite CPR is associated with increased morbidity and mortality.
- Combined predictor (Perlman & Risser): 5-min Apgar ≤5 + delivery room intubation or CPR + umbilical arterial pH <7.00 = 340-fold increased risk of seizures and moderate-severe encephalopathy (Creasy & Resnik).
4. Time to Establish Spontaneous Respiration
- ≥30 minutes to spontaneous breathing → strong predictor of mortality and neurological morbidity (AIIMS Protocol).
5. Extended Very Low Apgar Scores
- Low Apgar persisting ≥20 minutes → predictor of mortality and neurological morbidity (AIIMS Protocol).
6. Neurological Examination Severity
- Severe HIE at examination = adverse outcome indicator.
- Improvement by day 5: favorable; clinical signs persisting beyond day 7: unfavorable.
B. BIOCHEMICAL PREDICTORS
1. Cord / Neonatal Blood Gas (pH and Base Deficit)
- pH <7.0 and/or base deficit ≥16 mEq/L in cord blood or first-hour blood gas are criteria for therapeutic hypothermia.
- Meta-analysis shows good association of cord ABG abnormalities (pH <7.0 and BD ≥16 mmol/L) with short-term outcomes (mortality, HIE, IVH, PVL) AND long-term outcomes (cerebral palsy) (AIIMS Protocol; Harriet Lane).
- pH ≤7.11 within 24 hours of birth is among the strongest predictors of death or severe NDI (Glass et al., JAMA Netw Open, 2024; specificity 99.6%, PPV 95.2% when combined with other markers).
- Lower pH and more negative base deficit = poorer short-term prognosis.
2. Lactate
- High and persistently elevated serum lactate = poor outcome.
- Prolonged time to normalization of serum lactate correlates with severity of encephalopathy and seizures.
- Combined biochemical panel (lactate + CK + LDH + uric acid) predicts HIE severity.
3. PCO2 (Hypocarbia)
- Hypocarbia is a potent cerebral vasoconstrictor and cerebral blood flow modulator.
- Decreasing PCO2 correlates with unfavorable outcome at 18 months (CoolCap Study secondary analysis).
- High variability in PCO2 over 72 hours of hypothermia = poorer 2-year outcomes.
4. Glycemia
- Early glycemic profile in HIE is associated with neurodevelopmental outcomes.
- Both hypoglycemia and hyperglycemia are detrimental.
C. NEUROPHYSIOLOGICAL PREDICTORS
1. EEG / Amplitude-Integrated EEG (aEEG)
- The most important short-term neurophysiological predictor.
- 2026 systematic review and meta-analysis (PMID: 41078063, Neonatology, 2026) confirms EEG and aEEG predict neurodevelopmental outcomes with high diagnostic test accuracy.
- Severely abnormal EEG (persistently discontinuous, burst-suppression, electrocerebral silence, refractory seizures) = significant underlying brain injury.
- Combined predictor (Glass et al., JAMA Netw Open 2024): Severely abnormal EEG + pH ≤7.11 + 5-min Apgar = 0 → specificity 99.6%, PPV 95.2% for death/severe NDI.
- Early EEG grade predicts outcome at 5 years even in mild HIE.
- Abnormal visual and auditory evoked potentials = additional poor prognostic signs (Adams & Victor).
2. Seizure Burden
- Odds of abnormal outcome increase with:
- Total seizure burden >40 minutes
- Maximum hourly seizure burden >13 min/hour
- Median age of onset: 13 hours; median number: 2/hour.
- Clinical seizures are independently associated with adverse outcome.
D. NEUROIMAGING PREDICTORS
1. MRI Brain (Gold Standard for Extent and Timing of Injury)
Two predominant DWI patterns (Bradley-Daroff's Neurology):
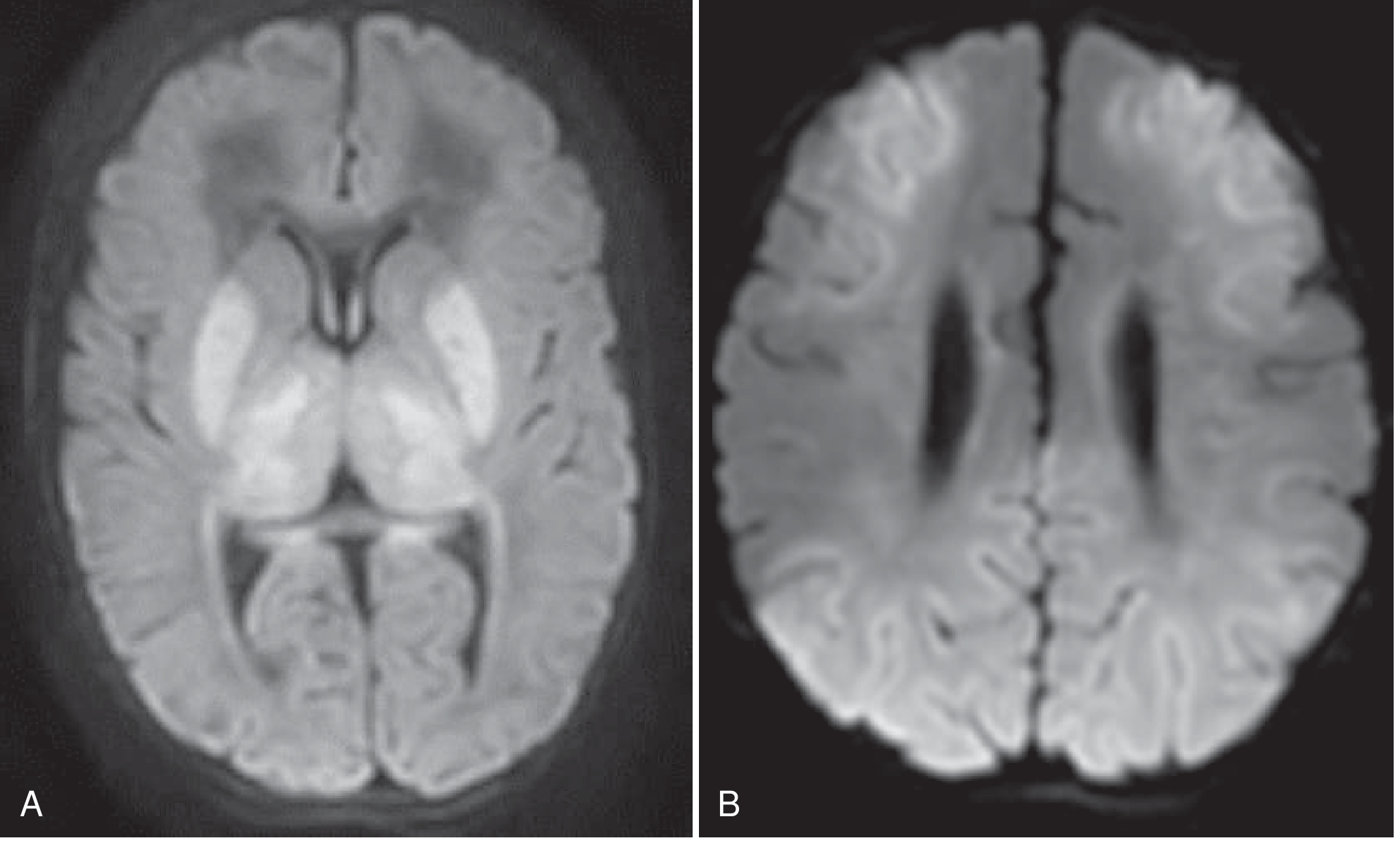
A. Basal Ganglia-Thalamus Pattern:
- Involves ventrolateral thalami, posterior putamina, perirolandic cortex.
- Seen after acute sentinel events (cord prolapse, abruption).
- Predicts: spastic quadriplegia, severe intellectual disability.
B. Watershed-Predominant Pattern:
- Involves ACA-MCA and MCA-PCA watershed zones; white matter + overlying cortex.
- Seen after prolonged partial asphyxia without a sentinel event.
- Predicts: cognitive impairment, speech-language disorders; motor function often relatively spared.
MRI Timing:
- DWI: Signal changes within 24-48 hours, peaks at a few days, "pseudo-normalizes" by end of first week (more rapid in severe injury).
- T1/T2 changes (including absent high-signal of posterior limb of internal capsule on T1): begin day 3-4.
- Absence of normal T1 signal in posterior limb of internal capsule = poor prognosis for motor outcome.
- Abnormalities in ≥2 deep grey matter regions (thalamus, caudate, putamen/globus pallidus) post-cooling + severely abnormal EEG → specificity 99.1%, PPV 91.7% for severe NDI (Glass et al., 2024).
MR Spectroscopy:
- Elevated lactate:N-acetyl aspartate (Lac:NAA) ratio in deep grey nuclei has strong prognostic value.
- Elevated lactate, reduced N-acetyl aspartate, altered choline/creatinine = metabolic injury.
2. Cranial Ultrasound
- Useful initial imaging, especially for preterm or unstable infants.
- Detects IVH, periventricular leukomalacia, echogenicity changes.
- Less sensitive than MRI for cortical and subtle white matter injury.
E. HEMODYNAMIC PREDICTORS
- Hemodynamic instability in 33-77% of neonates with HIE on therapeutic hypothermia.
- Hypotension in first 72 hours → increased risk of severe brain injury on MRI.
- Need for inotropes in first 72 hours → associated with increased risk of death or brain injury on MRI.
- Pulmonary hypertension on echocardiography → associated with abnormal brain MRI after rewarming.
- Cardiac dysfunction mediates ongoing brain injury.
F. LONG-TERM OUTCOMES
Short-term Outcomes (Neonatal Period):
- Death
- Seizures (neonatal)
- Multi-organ dysfunction (renal - ATN, hepatic injury, NEC, PPHN, DIC, SIADH, hypocalcemia)
Long-term Outcomes (Survivors of Moderate-Severe HIE):
| Outcome | Incidence |
|---|---|
| Combined death or IQ <70 at 6-7 years (with TH) | 47% (vs. 62% without TH) |
| Cerebral palsy (among survivors) | ~21% |
| Survival with IQ <70 at 6-7 years | ~27% |
| Blindness (at 18-22 months) | ~7% |
| Severe hearing impairment | ~4% |
| Epilepsy | Variable |
| Cognitive/developmental delay | Common |
(AIIMS Protocol; Creasy & Resnik; Bradley-Daroff)
Forms of CP: Hemiplegia, paraplegia, quadriplegia (spastic > dyskinetic > ataxic)
Mild HIE: Generally free from death or neurological sequelae.
G. MULTIMODAL APPROACH - SUMMARY
No single predictor is adequate in isolation. The current consensus is a multimodal approach combining:
- Clinical - Sarnat stage, Thompson score, neurological examination trajectory
- Biochemical - pH, base deficit, lactate, glycemia
- Neurophysiology - EEG/aEEG (early and serial), evoked potentials
- Neuroimaging - MRI at day 3-5 (DWI), MRS, internal capsule T1 signal, post-cooling MRI
- Hemodynamic - presence of inotrope requirement, PPHN, hypotension
(Creasy & Resnik; AIIMS Protocol; Bradley-Daroff; Harriet Lane; Adams & Victor; Glass et al., JAMA Netw Open 2024)
Recent Evidence Update: A 2026 systematic review with meta-analysis (PMID: 41078063) confirms that early EEG and aEEG are robust predictors of neurodevelopmental outcome in HIE with high diagnostic accuracy. A 2024 study (Glass et al., JAMA Netw Open) identified the most specific predictor combination: severely abnormal EEG + pH ≤7.11 + 5-min Apgar = 0 (pre-cooling), and ≥2 deep grey matter MRI abnormalities + severely abnormal EEG (post-cooling), each with PPV exceeding 90% for death or severe NDI.
This is a shared conversation. Sign in to Orris to start your own chat.