Development of the Mandible & Its Anomalies
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information. Let me compile the full answer.
Development of the Mandible & Its Anomalies
1. Embryological Origin
The mandible is a derivative of the first pharyngeal arch (mandibular arch). The first arch contains a cartilaginous rod called Meckel's cartilage, which acts as a scaffold (template) for mandibular development but does not contribute directly to its formation.
The first pharyngeal arch is innervated by the trigeminal nerve (CN V), which supplies all muscles and mucosa derived from it.
2. Method of Ossification
The mandible forms by intramembranous ossification of mesenchymal tissue surrounding Meckel's cartilage. This is the same mechanism used by flat bones of the skull, the clavicle, and other facial bones.
"The mandible is formed by intramembranous ossification of mesenchymal tissue surrounding the first arch cartilage. The cartilage acts as a template for development of the mandible but does not contribute directly to its formation."
- The Developing Human: Clinically Oriented Embryology, p. 466
Exception - the condyle: The condylar head of the mandible undergoes secondary endochondral ossification (secondary cartilage), distinct from the primary Meckel's cartilage mechanism. This makes the mandibular condyle a site of growth and remodeling throughout childhood.
Ossification Timeline
- First ossification centre appears at 6 weeks of intrauterine life (near the mental foramen region)
- The two halves of the mandible (right and left hemimandibles) are initially separate and unite at the symphysis menti during the 2nd year of postnatal life
3. Pharyngeal Arch Cartilage Diagram
The diagram below (from The Developing Human) shows Meckel's cartilage in the 4-week embryo (A) and its adult derivatives (B). Note that the mandible does not ossify from the cartilage itself - the cartilage is resorbed/disappears, while some portions persist as ligaments and ossicles:
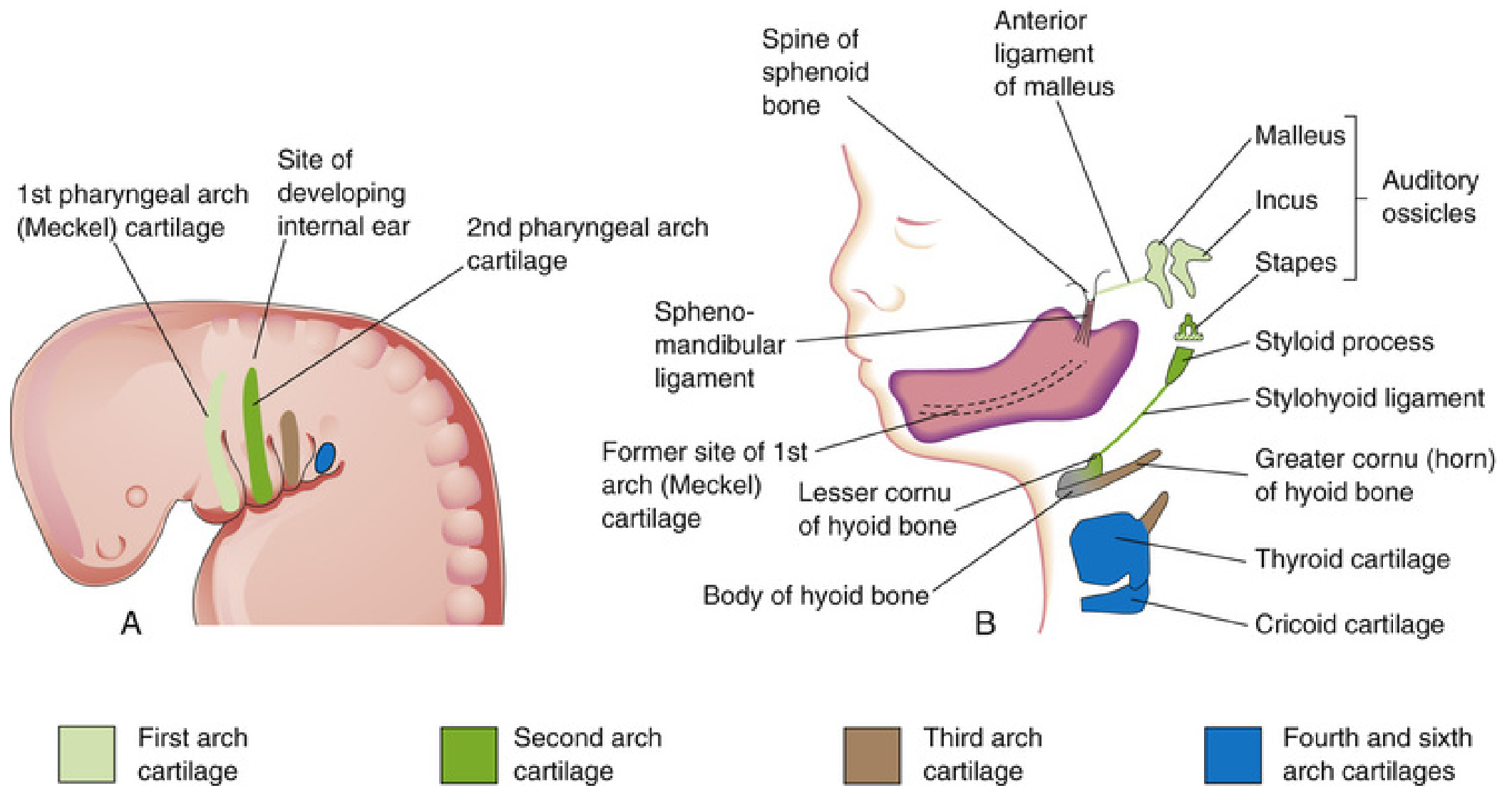
Fate of Meckel's cartilage (1st arch cartilage):
| Portion | Adult Derivative |
|---|---|
| Dorsal end | Malleus and Incus (auditory ossicles) |
| Middle | Sphenomandibular ligament (fibrous remnant) |
| Ventral portion | Disappears - serves as template for mandible ossification |
4. First Pharyngeal Arch Derivatives (Table)
| Component | Skeletal | Muscles | Nerve | Ligament |
|---|---|---|---|---|
| 1st arch (mandibular) | Malleus, Incus | Muscles of mastication, Mylohyoid, Anterior digastric, Tensor tympani, Tensor veli palatini | CN V (Trigeminal) | Anterior ligament of malleus, Sphenomandibular ligament |
5. Postnatal Growth of the Mandible
- At birth, the mandible consists of two halves joined at the symphysis menti by fibrous tissue (symphyseal cartilage)
- The two halves fuse by early childhood (1-2 years)
- Growth of the mandible occurs primarily at the condylar cartilage (secondary cartilage), which is a major site of endochondral growth
- The body of the mandible also grows by periosteal apposition on the outer surface and resorption on the inner surface
- The angle of the mandible changes with age: wide/obtuse in infants (about 150°), becoming more acute (~120°) in adults
6. Anomalies of the Mandible
6.1 First Pharyngeal Arch Syndrome
The major group of mandibular anomalies results from insufficient migration of neural crest cells into the first pharyngeal arch during the 4th week of development. This is collectively called First Arch Syndrome, producing birth defects of the eyes, ears, mandible, and palate.
The photograph below shows an infant with first arch syndrome, with mandibular hypoplasia, deformed auricle, and macrostomia:
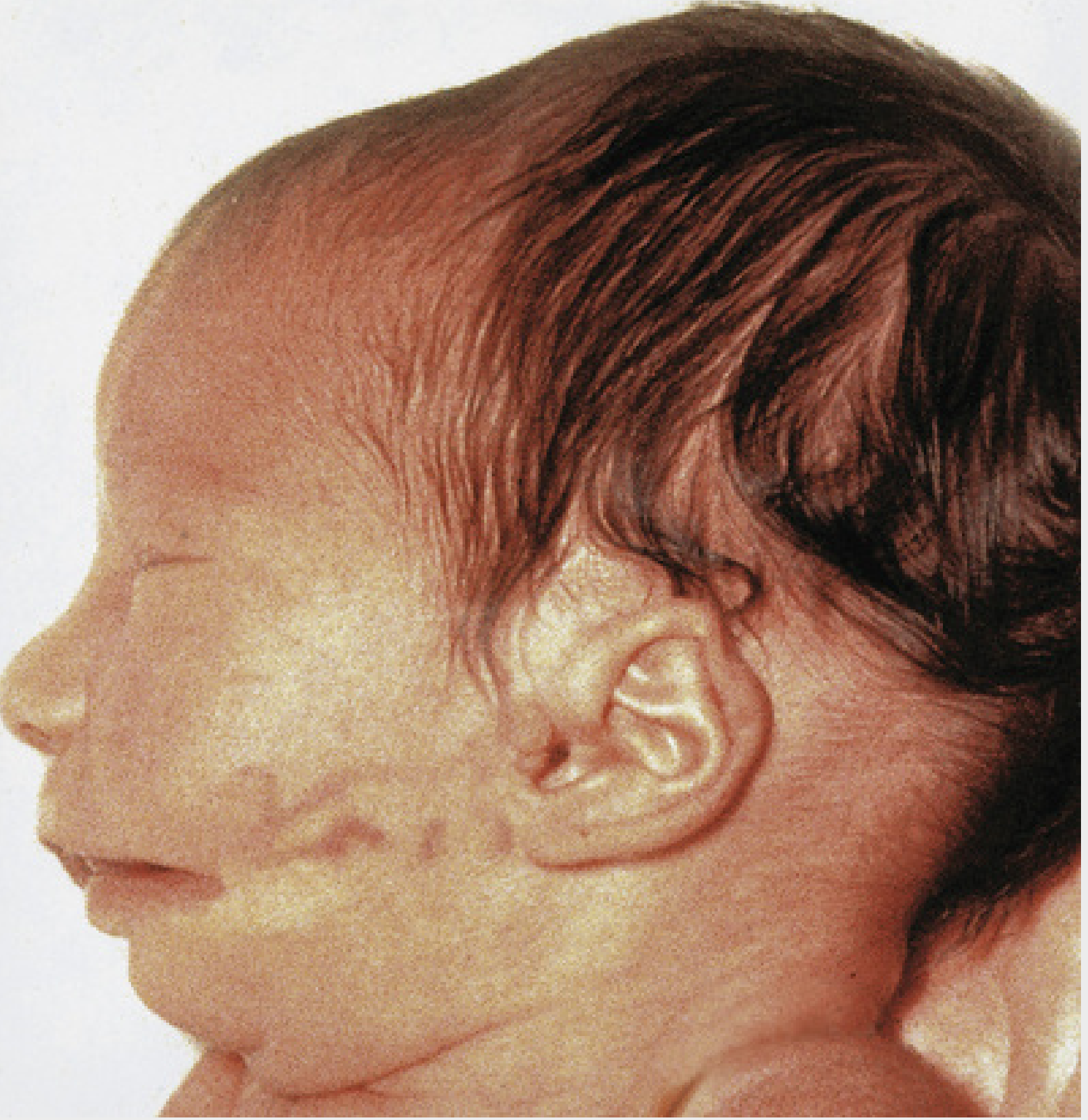
There are two main manifestations:
6.2 Treacher Collins Syndrome (Mandibulofacial Dysostosis)
- Inheritance: Autosomal dominant
- Gene: Mutation in TCOF1 gene (chromosome 5q32) → defective production of treacle protein, which is involved in ribosomal RNA biogenesis for facial bone and cartilage development
- Pathogenesis: Insufficient neural crest cell migration to the 1st and 2nd arches
- Features:
- Malar (zygomatic) hypoplasia
- Down-slanting palpebral fissures
- Defects/colobomas of the lower eyelids
- Mandibular hypoplasia
- Deformed external ears (microtia), sometimes with middle/inner ear defects
- Hearing loss (conductive)
- Macrostomia
- Bilateral and symmetric involvement
6.3 Pierre Robin Sequence
- Mechanism: The initiating defect is micrognathia (small mandible). This causes the tongue to fall posteriorly (glossoptosis), which physically obstructs the palatal shelves from elevating and fusing, resulting in a U-shaped cleft palate
- Triad:
- Micrognathia
- Glossoptosis (posterior tongue displacement)
- Cleft palate
- Inheritance: Usually de novo; rarely autosomal dominant
- Important association: ~30-40% of cases have Stickler syndrome (autosomal dominant collagen disorder)
- Clinical risk: Upper airway obstruction in neonates
"In the Robin morphogenetic complex, the initiating defect is a small mandible (micrognathia), which results in posterior displacement of the tongue and obstruction to full closure of the palatal processes, resulting in a bilateral cleft palate."
- The Developing Human, p. 487
6.4 Hemifacial Microsomia (Craniofacial Microsomia / Goldenhar Syndrome)
- Incidence: ~1 per 5,600 births
- Pathogenesis: Hypothesized to result from a unilateral hemorrhagic event involving the stapedial artery during early craniofacial development
- Features (typically unilateral):
- Mandibular, maxillary, zygomatic, and temporal hypoplasia
- External ear deformities (microtia, atresia of external auditory canal, preauricular skin tags)
- Hypoplastic facial musculature; facial paresis
- Ocular involvement (colobomas, epibulbar choristomas)
- Vertebral anomalies (fusion, spina bifida)
- Inheritance: Usually sporadic
- Also known as oculoauriculovertebral (OAV) spectrum
6.5 Other Mandibular Anomalies
| Anomaly | Description |
|---|---|
| Agnathia | Complete absence of the mandible; extremely rare, lethal |
| Micrognathia | Underdevelopment of the mandible; may be isolated or part of a syndrome |
| Macrognathia (Prognathism) | Overgrowth of the mandible; may occur in acromegaly or isolated |
| Bifid mandible | Failure of midline fusion; very rare |
| Cervical branchial vestiges | Residual cartilaginous/bony remnants of pharyngeal arch cartilage appearing in the neck (anterior to the lower 1/3 of sternocleidomastoid) |
7. Forensic & Age Estimation Notes
- First ossification centre appears in the mandible at ~6 weeks intrauterine life (one of the earliest ossification centres)
- The two halves of the mandible unite at the symphysis menti by 2 years
- Eruption of teeth and mandibular morphology are used in forensic age estimation
- Source: The Essentials of Forensic Medicine and Toxicology, 36th Ed.
Summary
| Feature | Detail |
|---|---|
| Pharyngeal arch | 1st (mandibular) arch |
| Cartilage involved | Meckel's cartilage (1st arch) |
| Ossification type | Intramembranous (body); Secondary endochondral (condyle) |
| Nerve supply | CN V (Trigeminal) |
| Ossification begins | 6th week IU life |
| Symphysis fusion | ~2 years postnatal |
| Main anomaly group | First arch syndrome (insufficient NCC migration) |
| Key syndromes | Treacher Collins, Pierre Robin, Hemifacial microsomia |
Sources:
- The Developing Human: Clinically Oriented Embryology - pp. 464-487
- Gray's Anatomy for Students - pp. 993-994
- Cummings Otolaryngology Head and Neck Surgery - Craniofacial Syndromes chapter
- The Essentials of Forensic Medicine and Toxicology, 36th Ed. - pp. 7532-7554
This is a shared conversation. Sign in to Orris to start your own chat.