Lung carcinoma Squamous cell carcinoma Small cell carcinoma
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks to compose a detailed answer. Let me compile the full response.
Lung Carcinoma: Overview, Squamous Cell Carcinoma & Small Cell Carcinoma
Overview of Lung Carcinoma
Lung cancer is the leading cause of cancer-related death worldwide. About 90% of cases occur in current or recent smokers, with a nearly linear correlation to pack-years of smoking (60x increased risk with 2 packs/day for 20 years). Women are more susceptible to tobacco carcinogens than men.
WHO Classification (2021, Simplified)
| Category | Subtypes |
|---|---|
| Adenocarcinoma | Acinar, papillary, micropapillary, solid, lepidic, mucinous |
| Squamous cell carcinoma | Keratinizing, nonkeratinizing, basaloid |
| Large cell carcinoma | - |
| Neuroendocrine carcinoma | Small cell carcinoma, Large cell neuroendocrine, Carcinoid |
| Mixed | Adenosquamous, SCLC + other types |
Proportions:
- NSCLC (adenocarcinoma + SCC + large cell) ~ 84%
- Small cell carcinoma ~ 13-15%
- Neuroendocrine (carcinoid) ~ 1-2%
Pathogenesis
Lung cancers arise by stepwise accumulation of driver mutations. Key events include:
- Early event: Loss of chromosomal material on 3p (found even in benign bronchial epithelium of smokers - "field effect")
- Late events: TP53 mutations, KRAS oncogene mutations
- Adenocarcinoma-specific targetable mutations: EGFR, KRAS, ALK, ROS1, HER2, MET
Molecular targets differ sharply between SCC and SCLC/adenocarcinoma - this drives "personalized" therapy.
Part 1: Squamous Cell Carcinoma (SCC)
Epidemiology & Risk Factors
- ~25% of all lung cancers in the USA
- Strongly linked to smoking - the most important risk factor
- More common in men than women
- Historically central (2/3 were hilar/airway-associated), but there has been a trend toward more peripheral SCC over the past 2 decades - possibly linked to the shift from unfiltered to filtered cigarettes
Pathogenesis & Precursor Lesions
SCC has a well-documented stepwise morphologic progression:
Normal epithelium → Basal cell hyperplasia → Squamous metaplasia → Squamous dysplasia → Carcinoma in situ → Invasive SCC
Tumors likely originate from basal squamous cells with stem cell-like properties.
Key mutations: TP53 (65%), PIK3CA (30%), CDKN2A (25%), SOX2 (15%), CCND1 (15%). None are currently actionable for targeted therapy. FGFR1 amplification occurs in up to 20% but FGFR inhibitors alone have been largely ineffective.
Gross Pathology
- Central location - arises in major bronchi, spreads first to local hilar nodes
- Dissemination outside the thorax occurs later than other subtypes
- Large lesions may undergo central necrosis → cavitation
Panel D in the Robbins image (below) shows SCC as a large central (hilar) mass invading contiguous parenchyma.
Histology
Hallmarks of squamous differentiation:
- Intercellular bridges (Panel A in SCC image)
- Intracellular keratinization of individual cells (Panel B)
- Keratin pearls - concentric whorls of keratinized cells (Panel B, arrow; Panel C in Robbins image)
These features are readily apparent in well-differentiated tumors, subtle in moderately differentiated, and may be absent in poorly differentiated tumors.
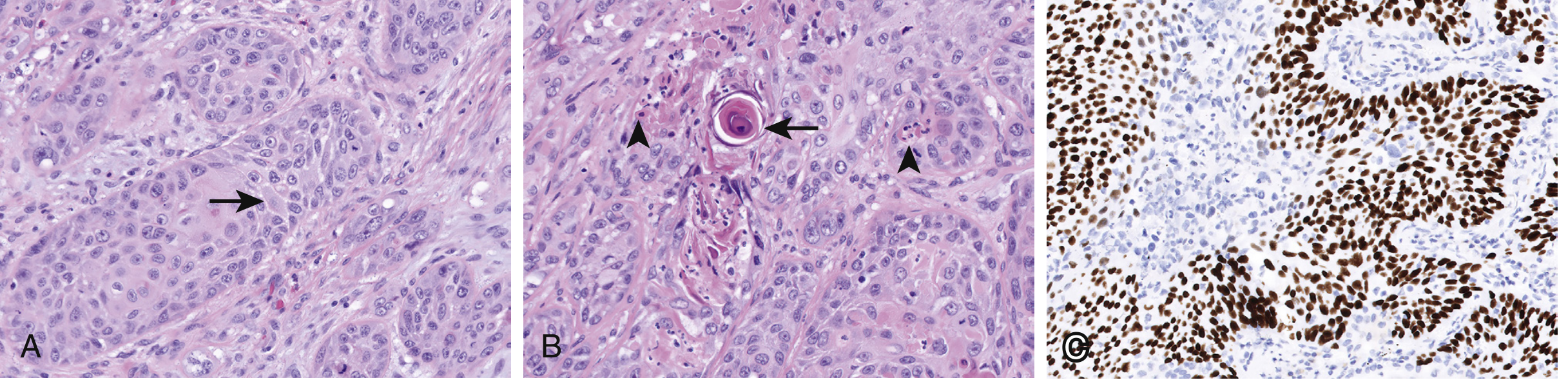
Squamous cell carcinoma: (A) intercellular bridges, (B) keratin pearls (arrow) and intracellular keratinization (arrowheads), (C) p40 IHC (brown staining) confirming squamous differentiation. - Murray & Nadel's Textbook of Respiratory Medicine
Immunohistochemistry
- Positive: p63, p40 (splice variant of p63) - nuclear expression
- Negative: TTF-1 and napsin A (adenocarcinoma markers)
Paraneoplastic Syndromes
- Hypercalcemia - via PTHrP (parathyroid hormone-related peptide) - most characteristic paraneoplastic syndrome of SCC
- SIADH can also occur (though more typical of SCLC)
Part 2: Small Cell Carcinoma (SCLC)
Epidemiology
- ~10-15% of all lung cancers
- Most aggressive pulmonary tumor - often widely disseminated at diagnosis
-
80% present at advanced stage (III or IV)
- Most cases present as a perihilar mass
- Unlike NSCLC, low-dose CT screening does NOT significantly improve detection of early-stage SCLC
Pathogenesis
- Precursor lesions for SCLC have NOT been clearly described (unlike SCC)
- Virtually all SCLC have bi-allelic loss of function mutations in both TP53 and RB1 (~90% each)
- 3p deletions: ~90%
- p16/CDKN2A mutations: only ~10% (contrast with NSCLC ~50%)
- KRAS and EGFR mutations: absent/rare (major distinction from adenocarcinoma)
Origin
SCLC belongs to the neuroendocrine spectrum of lung tumors. The spectrum from least to most aggressive is:
Typical carcinoid → Atypical carcinoid → Large cell neuroendocrine carcinoma → Small cell carcinoma
Histology
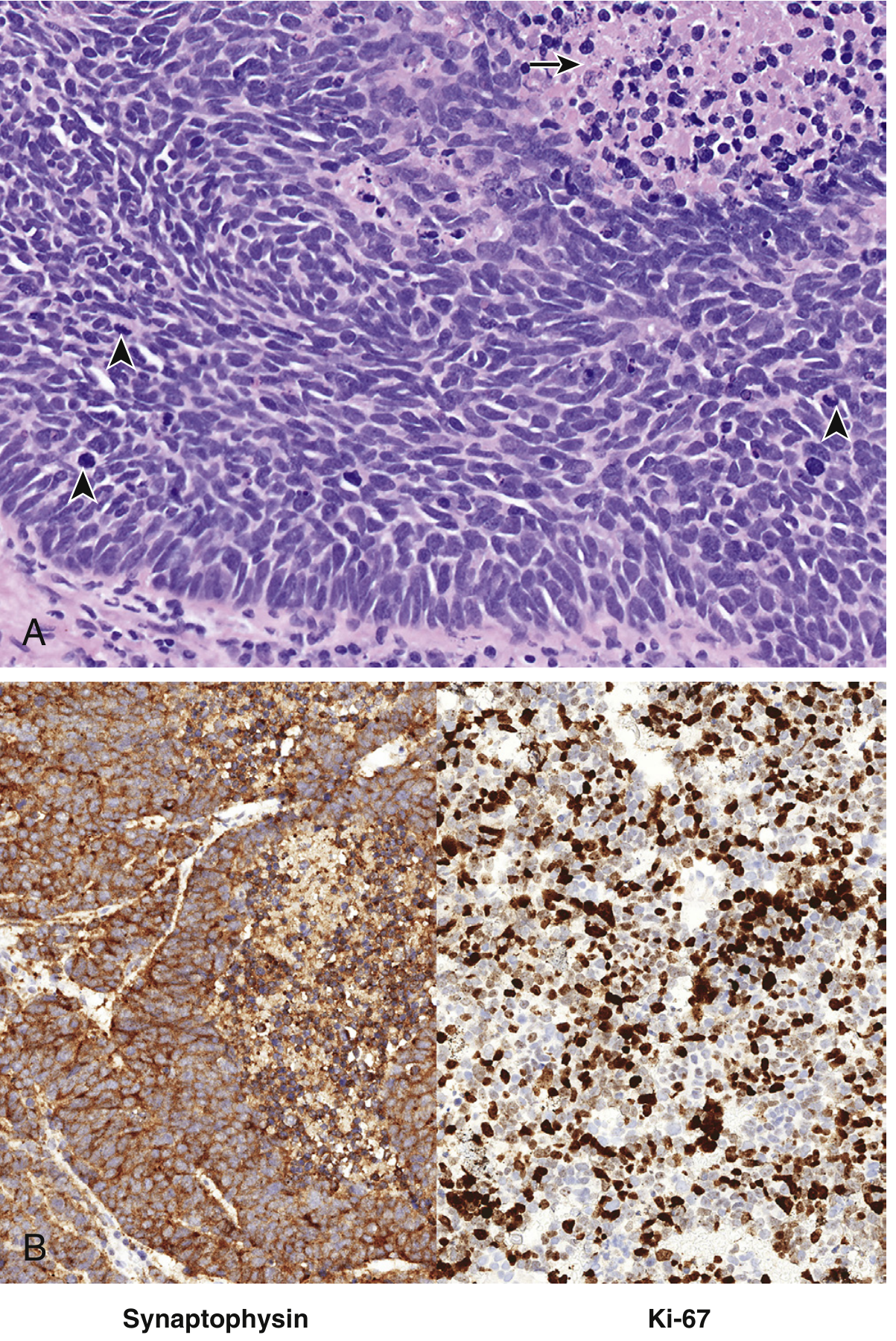
Small cell carcinoma: (A) H&E - "small" cells with high N:C ratio, finely granular chromatin, absent nucleoli, mitotic figures (arrowheads) and necrosis (arrow). (B) Synaptophysin IHC positive (neuroendocrine marker); Ki-67 >80% proliferation index. - Murray & Nadel's Textbook of Respiratory Medicine
Key histologic features:
- Solid sheetlike or nested growth architecture
- Scant pale cytoplasm - gives impression of "small" cell size (actually 2-3x the size of a lymphocyte)
- Fragile nuclear envelopes - nuclear "smudging" and nuclear "molding" (cells conforming to each other's shape)
- Finely granular chromatin ("salt and pepper")
- Absent or inconspicuous nucleoli
- High mitotic rate + extensive necrosis
- Azzopardi effect - basophilic encrustation of vascular walls by DNA from necrotic tumor cells (see Panel F in Robbins image)
IHC Profile
- Positive: Synaptophysin, chromogranin A, CD56 (neuroendocrine markers); dense-core granules on electron microscopy
- Ki-67: Usually >80% (very high proliferation)
- Positive: Epithelial membrane antigen (EMA), CEA, cytokeratins
- Negative: TTF-1 and napsin A (adenocarcinoma markers)
Staging
SCLC uses the Veterans Administration two-stage system (clarified by IASLC):
| Stage | Definition | Features |
|---|---|---|
| Limited Stage (LS) | Confined to one hemithorax + regional nodes (hilar, ipsilateral/contralateral mediastinal, supraclavicular), ± ipsilateral pleural effusion | ~30-40% of patients |
| Extensive Stage (ES) | Beyond LS; includes contralateral/bilateral pulmonary involvement, pericardial involvement, distant mets | ~60-70% of patients |
Common metastatic sites: bone, liver, bone marrow, CNS (brain MRI mandatory for staging)
Treatment & Prognosis
- Very sensitive to chemotherapy and radiotherapy but invariably recurs
- Surgery is rarely indicated - usually only for T1-2 N0-1 (stage I/II) peripheral lesions
- LS-SCLC: Etoposide + cisplatin + concurrent thoracic radiation → response rate 85-90%, complete response 50-60%; median survival 18-24 months; 2-year survival 40-50%
- ES-SCLC: Chemotherapy alone → response rate 75-85%, complete response only 15-25%; median survival 7-11 months; 2-year survival <5%
- Prophylactic cranial irradiation (PCI) reduces brain metastasis risk
- Checkpoint inhibitors: SCLC is largely unresponsive (unlike NSCLC)
- Targeted therapies: currently unavailable
- Overall 10-year survival: only ~5%
Part 3: Robbins Pathology Composite - All Types
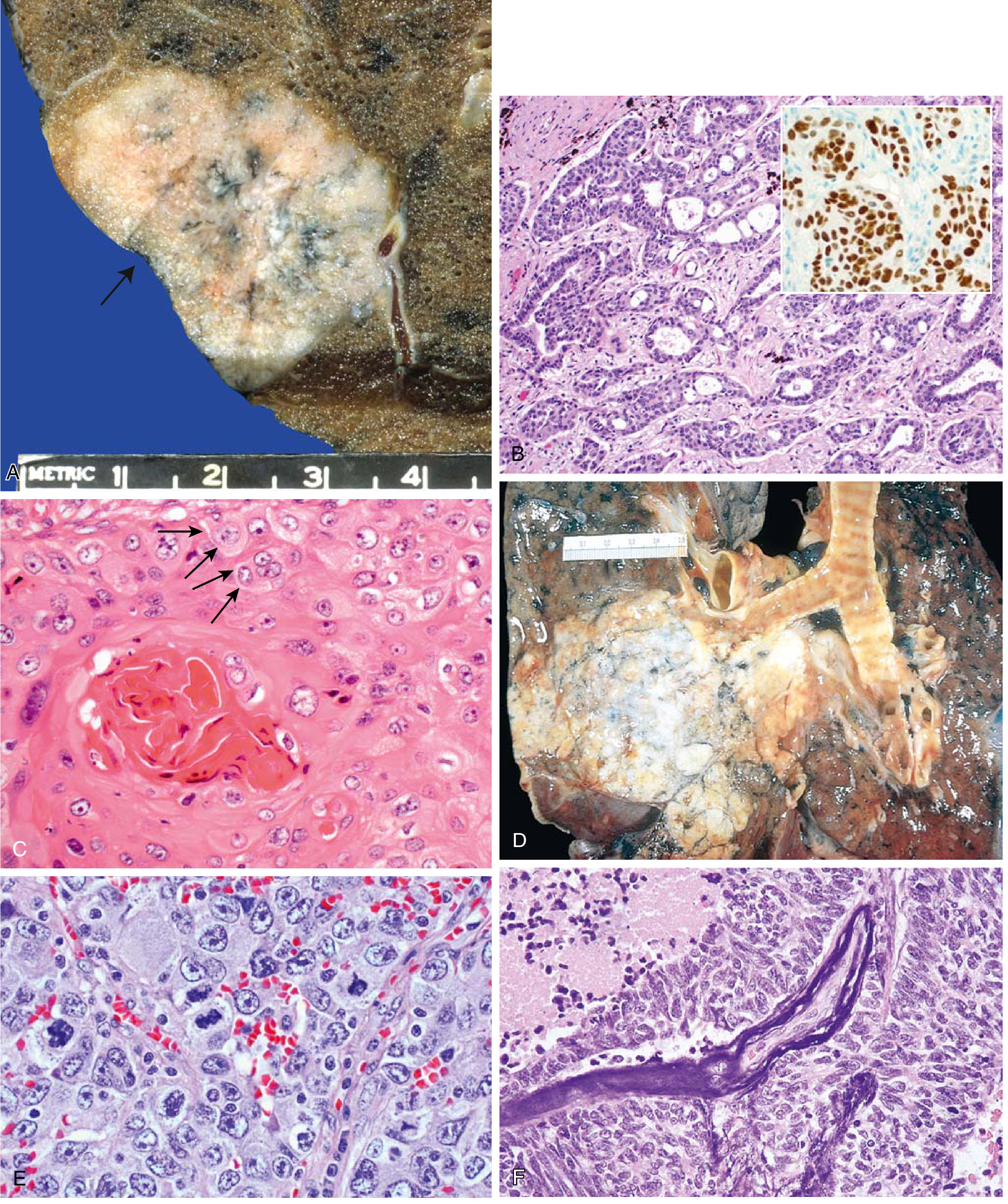
FIG. 11.44 (Robbins): (A) Peripheral adenocarcinoma with pleural puckering. (B) Gland-forming adenocarcinoma with TTF-1 IHC inset. (C) Well-differentiated SCC - keratin pearl + intercellular bridges (arrows). (D) SCC as central hilar mass invading parenchyma. (E) Large cell carcinoma. (F) Small cell carcinoma - small deeply basophilic cells with necrosis (top left) and Azzopardi effect (basophilic vascular staining).
Comparison Table: SCLC vs NSCLC (Robbins Table 11.6)
| Feature | Small Cell Carcinoma | NSCLC (Adeno + SCC) |
|---|---|---|
| Microscopy | Scant cytoplasm; small hyperchromatic nuclei; fine chromatin; indistinct nucleoli; diffuse sheets | Abundant cytoplasm; pleomorphic nuclei; coarse chromatin; prominent nucleoli; glandular or squamous architecture |
| Neuroendocrine markers (chromogranin, synaptophysin, CD56) | Present | Absent |
| Epithelial markers (EMA, CEA, cytokeratins) | Present | Present |
| Mucin | Absent | Present (adenocarcinoma) |
| Peptide hormones | ACTH, ADH, GRP, calcitonin | PTHrP (SCC) |
| 3p deletions | ~90% | ~80% |
| RB mutations | ~90% | ~20% |
| p16/CDKN2A mutations | ~10% | ~50% |
| TP53 mutations | ~90% | ~50% |
| KRAS mutations | Rare | ~30% (adenocarcinoma) |
| EGFR mutations | Absent | ~20% (adenocarcinoma, nonsmokers, women) |
| ALK fusions | Absent | 4-6% (adenocarcinoma) |
| Response to chemo/RT | Often complete, but invariably recur | Incomplete response |
| Response to checkpoint inhibitors | Unresponsive | Responsive |
| Surgical resection | Rarely curative | Curative if detected early |
Paraneoplastic Syndromes Summary
| Syndrome | Mediator | Type |
|---|---|---|
| Hypercalcemia | PTHrP | Squamous cell carcinoma |
| Cushing syndrome (ectopic ACTH) | ACTH | Small cell > squamous |
| SIADH | ADH (vasopressin) | Small cell carcinoma (also squamous) |
| Lambert-Eaton myasthenic syndrome | Anti-VGCC antibodies | Small cell carcinoma |
| Neurologic syndromes | Various | Small cell carcinoma |
| Hematologic syndromes | Various | Adenocarcinoma |
Common Clinical Features of All Lung Carcinomas
- Chronic cough, hemoptysis, expectoration (early)
- Hoarseness (recurrent laryngeal nerve involvement)
- Chest pain, dyspnea
- Superior vena cava syndrome (compression/invasion)
- Pancoast tumor - apical tumor invading brachial/cervical sympathetic plexus → ulnar distribution pain + Horner syndrome (enophthalmos, ptosis, miosis, anhidrosis) + 1st/2nd rib destruction
- Pleural or pericardial effusions
- Virchow's node - left supraclavicular node involvement
- Metastatic symptoms - brain (neurologic changes), liver (hepatomegaly), bone (pain), adrenal (rarely adrenal insufficiency)
Sources: Robbins & Kumar Basic Pathology (Robbins Pathology), pp. 485-490; Murray & Nadel's Textbook of Respiratory Medicine, pp. 562-563; Mulholland and Greenfield's Surgery, pp. 4279-4280; Fishman's Pulmonary Diseases and Disorders, p. 560
This is a shared conversation. Sign in to Orris to start your own chat.