Nocardia vs actinomycetes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the information needed for a thorough comparison. Here is the full, structured answer:
Nocardia vs. Actinomyces - A Complete Comparison
Both are Gram-positive, filamentous, branching rods that were historically mistaken for fungi. The single most testable distinction: Nocardia is aerobic and weakly acid-fast; Actinomyces is anaerobic and NOT acid-fast.
Key Features at a Glance
| Feature | Nocardia | Actinomyces |
|---|---|---|
| Kingdom | Bacteria (true) | Bacteria (true) |
| Gram stain | Gram-positive (often stains poorly, beaded) | Gram-positive |
| Acid-fast | Weakly acid-fast (1% H₂SO₄ decolorizer) | NOT acid-fast |
| Oxygen requirement | Strict aerobe | Anaerobe / microaerophile |
| Morphology | Branching filamentous rods; aerial hyphae | Branching filamentous rods; no aerial hyphae |
| Cell wall | Mycolic acids (C50-62; shorter than mycobacteria) | No mycolic acids |
| Source / Habitat | Exogenous - soil (rich organic matter) | Endogenous - normal oral/GI/genital flora |
| Infection route | Inhalation or traumatic inoculation | Mucosal disruption (trauma, surgery, IUD) |
| Host | Primarily immunocompromised | Immunocompetent (low virulence) |
| Sulfur granules | Absent | Present (pathognomonic) |
| Key species | N. asteroides, N. brasiliensis | A. israelii (most common) |
| Culture speed | 3-7+ days; aerobic media | 4-10 days; anaerobic media |
| Growth on non-selective media | Yes (if incubated long enough) | Requires anaerobic conditions |
Microbiology Details
Nocardia
- Gram-positive, strictly aerobic branching rods with mycolic acids in the cell wall (C50-62 carbons - shorter chain than mycobacteria, explaining why it is only weakly acid-fast vs. strongly acid-fast in TB).
- Virulence depends on avoiding intracellular killing: catalase and superoxide dismutase neutralize the oxidative burst; a cord factor prevents phagosome-lysosome fusion.
- Colonies initially white, can become dry/waxy or orange; aerial hyphae visible on dissecting microscopy. The combination of aerial hyphae + acid-fastness is unique to Nocardia.
-
100 species identified by gene sequencing; most infections caused by a few (N. asteroides complex, N. brasiliensis).
Actinomyces
- Gram-positive, anaerobic/microaerophilic branching rods. No mycolic acids, no acid-fastness.
- Colonize the alimentary tract (oral, GI, female genital tract) - never found on normal skin.
- Disease occurs only when mucosal barriers are disrupted (dental procedure, surgery, aspiration, IUD).
- Low virulence - disease is endogenous, with no person-to-person spread.
- The hallmark histological finding is sulfur granules - macroscopic colonies that look like grains of sand, with a dense Gram-positive center and filamentous rods at the periphery.
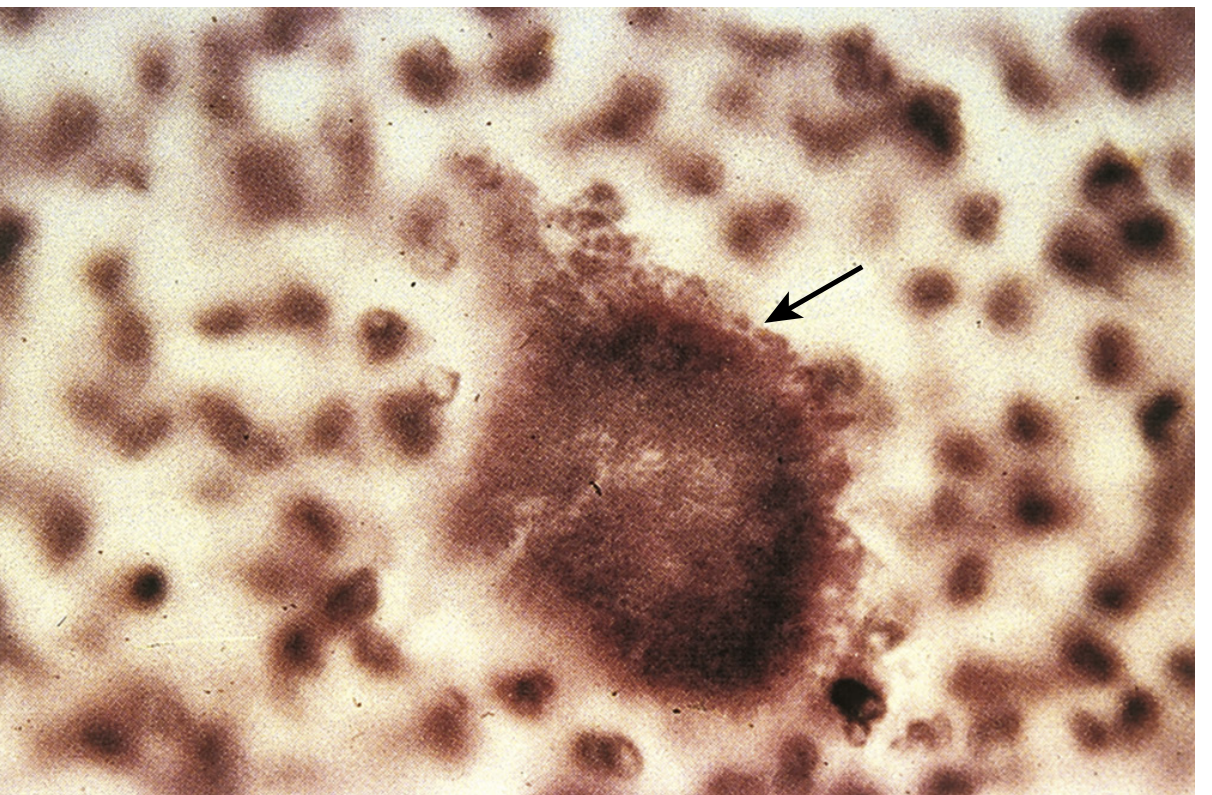
Sulfur granule from actinomycosis sinus tract - Medical Microbiology 9e, Fig. 31.3
Clinical Diseases
Nocardia - diseases
- Bronchopulmonary (most common): cavitary pneumonia, lung abscess, indolent course. Mimics TB or fungal infection on imaging.
- Cutaneous: mycetoma (chronic destructive disease of extremities), lymphocutaneous spread, cellulitis, subcutaneous abscess.
- CNS (disseminated): brain abscesses - occurs in 30% of pulmonary cases.
- Immunocompromised hosts: transplant recipients (tacrolimus/steroids), HIV, malignancy, corticosteroid use.
Actinomyces - diseases ("actinomycosis")
Follows a slow, burrowing course with induration, abscess, and draining sinus tracts opening through the skin.
- Cervicofacial ("lumpy jaw", most common, ~50%): follows dental trauma or extraction. Firm, indurated jaw mass with draining sinuses.
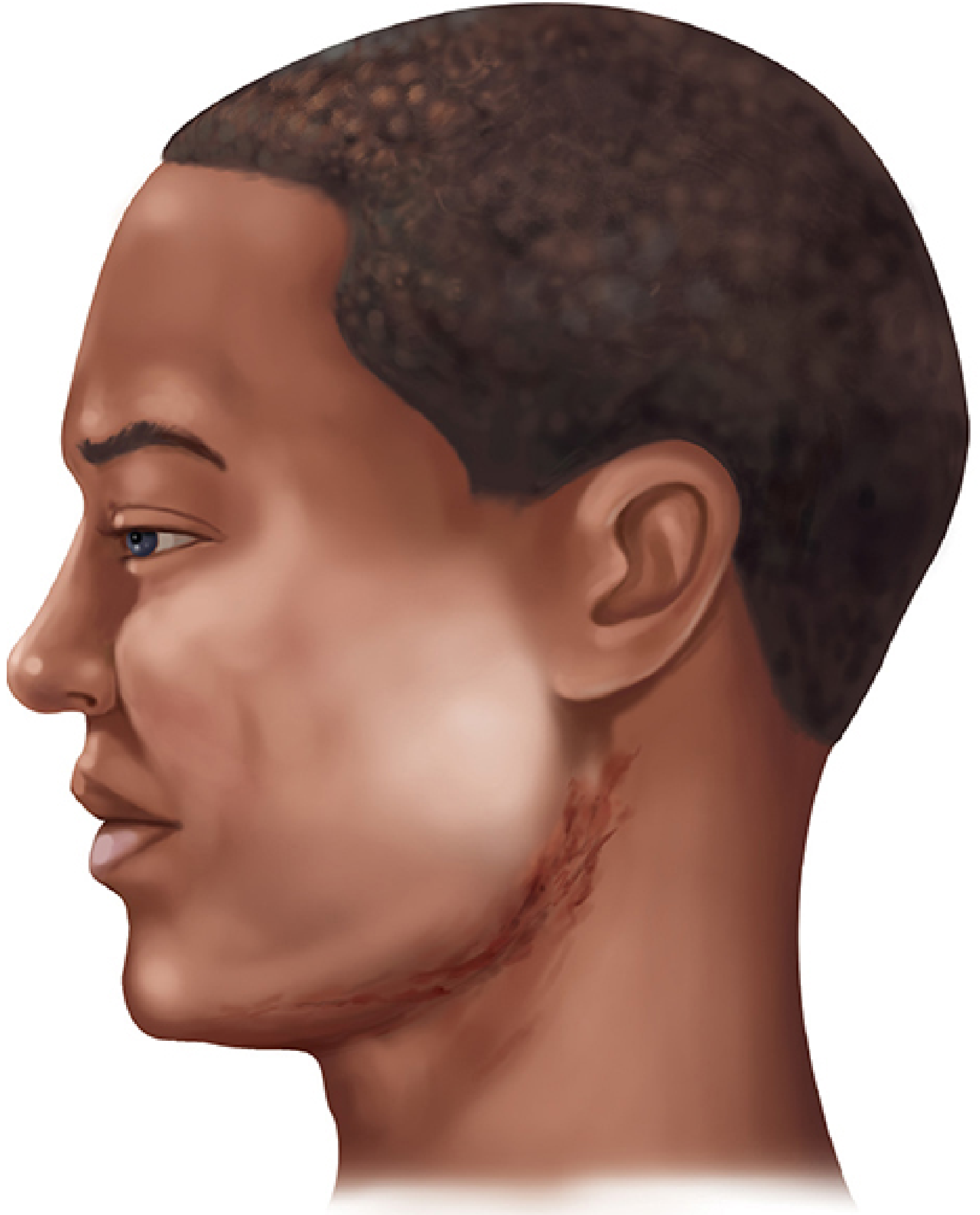
Cervicofacial actinomycosis - Sherris & Ryan's Medical Microbiology 8e, Fig. 28-4
- Thoracic: follows aspiration; erodes through pleura and chest wall; often mistaken for malignancy.
- Abdominal: follows bowel surgery or trauma; erosion through abdominal wall.
- Pelvic: associated with IUD use (chronic endometritis).
- CNS: rare.
Diagnosis
| Step | Nocardia | Actinomyces |
|---|---|---|
| Stain | Weakly acid-fast (1% H₂SO₄); beaded Gram-positive rods | Gram-positive branching rods; NOT acid-fast |
| Specimen | Sputum, BAL, pus aspirate, biopsy | Pus (look for sulfur granules), tissue biopsy |
| Key finding | Branching + weakly acid-fast = genus-level ID | Sulfur granules on direct smear or H&E biopsy |
| Culture | Aerobic; BCYE agar useful; 3-7+ days | Anaerobic; 7+ days; anaerobic blood agar |
| Species ID | Gene sequencing or mass spectrometry | Biochemical tests; genus-level usually sufficient |
| Pitfall | Slow growth - lab must be notified to hold cultures | Sinus drainage heavily contaminated with other organisms; organisms few in pus |
Treatment
| Nocardia | Actinomyces | |
|---|---|---|
| Drug of choice | TMP-SMX (trimethoprim-sulfamethoxazole) | Penicillin G (high dose, prolonged) |
| Severe/CNS disease | TMP-SMX + imipenem or cephalosporin | Penicillin IV, then amoxicillin PO |
| Cutaneous (immunocompetent) | TMP-SMX alone | Penicillin |
| Pulmonary (severe/immunocompromised) | TMP-SMX + amikacin | Penicillin |
| Duration | Up to 12 months | Weeks to 12 months (depending on extent) |
| Surgery | Drainage of abscesses as needed | Drainage of abscesses + excision of sinus tracts |
The Single Most Important Mnemonic
"NAA vs. AAA"
- Nocardia = Aerobic, Acid-fast (weak), Acquired from soil (exogenous)
- Actinomyces = Anaerobic, Acid-fast negative, Alimentary tract flora (endogenous)
Sources: Sherris & Ryan's Medical Microbiology 8e, p. 1121-1128; Medical Microbiology 9e, pp. 363-366, 269-274; The Washington Manual of Medical Therapeutics.
This is a shared conversation. Sign in to Orris to start your own chat.