A 35 yr old female came ith complaints of polayarthralgia, low back ache for past 2 minths not releived by oain killers, no h/o of trauma, no radiculopathy, on evaluation she came as ANA +, ESR+, CRP+ RA - hoe to proceed
Reading File
Finding Sources
Finding Sources
Searching PubMed
ANA positive polyarthralgia undifferentiated connective tissue disease workup
Reading File
Finding Sources
Finding Sources
Searching PubMed
undifferentiated connective tissue disease SLE diagnosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have sufficient information from authoritative sources to provide a thorough, structured answer. Let me compile the comprehensive response.
Clinical Approach: 35-year-old Female with Polyarthralgia + Low Back Ache + ANA+, ESR+, CRP+, RA-
This presentation is a classic rheumatology workup scenario. An ANA-positive young woman with polyarthralgia and elevated inflammatory markers but seronegative for RA points toward a connective tissue disease (CTD) - most likely SLE, primary Sjogren's syndrome, undifferentiated CTD (UCTD), or mixed CTD. Here is how to proceed systematically.
Step 1: Understand What You Already Know
| Finding | Interpretation |
|---|---|
| ANA positive | Serologic hallmark of autoimmune CTDs - SLE, Sjogren's, MCTD, SSc, UCTD |
| ESR + CRP raised | Active systemic inflammation confirmed |
| RA negative (RF-) | Seronegative - but does NOT exclude RA; more importantly, points away from RA and toward CTD spectrum |
| Polyarthralgia, 2 months | Chronic, NSAID-resistant - suggests immune-mediated not mechanical origin |
| Low back ache, no radiculopathy | May be inflammatory spondyloarthropathy or CTD-related |
| No trauma | Excludes traumatic cause |
| Young female 35 yr | Demographics strongly favor SLE (9:1 female:male ratio), Sjogren's, or UCTD |
Step 2: The Differential Diagnosis
Top differentials in order of likelihood:
- SLE (Systemic Lupus Erythematosus) - most common ANA+ CTD in young women; joint involvement scores 6 points on 2019 EULAR/ACR criteria
- Primary Sjogren's Syndrome - 50% of pSS patients show RA-like polyarthralgia; ANA positive in most cases; anti-Ro/SSA positive in ~2/3
- Undifferentiated CTD (UCTD) - ANA+ plus at least one CTD feature but not fulfilling any specific CTD criteria; ~25% eventually evolve to SLE
- Mixed CTD (MCTD) - overlap of SLE + SSc + myositis features; defined by high-titer anti-U1-RNP
- Inflammatory spondyloarthropathy (given back pain) - though ANA is not typical
- Early Systemic Sclerosis - especially if puffy fingers or Raynaud's present
- Viral arthritis (Parvovirus B19, Chikungunya, Ross River) - but 2 months duration makes persistent viral less likely
Step 3: Detailed History to Elicit NOW
Do a targeted systemic review for CTD features:
For SLE:
- Photosensitivity, malar/butterfly rash, discoid lesions
- Oral ulcers (painless)
- Hair loss (non-scarring alopecia)
- Pleuritis, pericarditis (chest pain)
- Raynaud's phenomenon
- Prior thrombosis or recurrent pregnancy loss (antiphospholipid)
- Nephritic symptoms - frothy urine, edema
- Neuropsychiatric symptoms - seizures, psychosis, headaches
- Unexplained fever, weight loss
For Sjogren's:
- Dry eyes (xerophthalmia), dry mouth (xerostomia) > 3 months
- Parotid gland enlargement
- Dental caries, difficulty swallowing dry food
For Spondyloarthropathy (given back pain):
- Morning stiffness > 30 min improving with activity
- Alternating buttock pain
- Psoriasis, inflammatory bowel disease, uveitis, urethritis
- Family history of AS/psoriasis/IBD
Step 4: Focused Clinical Examination
- Vital signs, weight loss
- Skin: malar rash, discoid lesions, photosensitive rash, livedo reticularis, vasculitic lesions
- Eyes: keratoconjunctivitis sicca (Schirmer test)
- Mouth: dry mucosa, oral ulcers, parotid enlargement
- Joints: synovitis vs arthralgia only, pattern (small/large/axial), tenderness, swelling
- Spine: sacroiliac joint tenderness, modified Schober test for lumbar flexion
- Lymphadenopathy, organomegaly
- Hair: diffuse alopecia
- Nails: periungual erythema, nail-fold capillaroscopy (if SSc suspected)
- Chest: pleural rub, signs of pericarditis
Step 5: Investigations - The Full Workup
Mandatory First-Line Serology (to narrow the CTD)
| Investigation | Purpose |
|---|---|
| ANA titer + pattern | If not done: titer ≥1:80 is entry criterion for SLE EULAR/ACR 2019 scoring; pattern gives clues (homogeneous → dsDNA; speckled → ENA; centromere → SSc) |
| Anti-dsDNA antibody | High specificity for SLE (scores 6 points in classification); also tracks disease activity |
| ENA panel (anti-Sm, anti-Ro/SSA, anti-La/SSB, anti-U1-RNP, anti-Scl-70, anti-Jo-1) | Anti-Sm: SLE-specific; anti-Ro+La: Sjogren's / neonatal lupus; anti-U1-RNP: MCTD; anti-Scl-70: SSc; anti-Jo-1: antisynthetase/myositis |
| Complement C3, C4 | Low C3/C4 in active SLE; C4 low also in inherited C4 deficiency |
| Anti-CCP (ACPA) | To firmly exclude seronegative RA (RF was done; anti-CCP adds specificity) |
| Antiphospholipid antibodies (anticardiolipin IgG/IgM, anti-β2GPI, lupus anticoagulant) | Antiphospholipid syndrome co-exists with SLE; scores 2 points |
| HLA-B27 | If spondyloarthropathy suspected given back pain without radiculopathy |
Mandatory Hematologic + Biochemical Panel
| Test | Why |
|---|---|
| CBC with differential | Leukopenia (scores 3 pts SLE), thrombocytopenia (4 pts), autoimmune hemolytic anemia (4 pts) |
| Direct Coombs test | Autoimmune hemolysis |
| Urine routine + microscopy | Proteinuria >0.5 g/24h (4 pts SLE); red cell casts = active nephritis |
| 24-hour urine protein OR spot urine protein:creatinine ratio | Quantify proteinuria |
| Serum creatinine, eGFR, LFTs | Baseline organ function |
| Blood glucose, lipid profile | Metabolic baseline (needed before starting steroids/HCQ) |
| Serum uric acid | Exclude gout co-morbidity |
| Thyroid function (TSH, fT4) | Autoimmune thyroiditis (Hashimoto's) common in ANA-positive young women; can cause myalgia, fatigue, joint pain |
Imaging
| Modality | Purpose |
|---|---|
| X-ray hands & feet (AP) | Erosions, joint space narrowing - to evaluate for early RA or psoriatic arthritis |
| MRI sacroiliac joints | Gold standard for early sacroiliitis/spondyloarthropathy (X-ray has low sensitivity early) |
| X-ray lumbosacral spine | Syndesmophytes, DISH, degenerative changes |
| Chest X-ray | Pleuritis, cardiomegaly, ILD |
| ECHO (2D) | If pericarditis suspected; also for pulmonary hypertension screening |
| HRCT chest | If ILD suspected (dry cough, crackles) |
Additional Tests (Symptom-directed)
- Schirmer's test / Rose Bengal staining if dry eye symptoms
- Minor salivary gland biopsy (focal lymphocytic sialadenitis) if Sjogren's strongly suspected
- Nail-fold capillaroscopy if Raynaud's or SSc suspected
- Muscle enzymes (CK, LDH, aldolase) if myalgia prominent
- Anti-ribosomal P antibody if neuropsychiatric symptoms
Step 6: Scoring - Apply 2019 EULAR/ACR SLE Classification Criteria
The diagnosis of SLE is clinical, supported by laboratory abnormalities. Per the 2019 criteria (Goldman-Cecil Medicine, Table 245):
- Entry criterion: ANA ≥1:80 - your patient already qualifies ✓
- Then score additional domains:
- Joint involvement: +6 points
- Each immunologic finding (anti-dsDNA, low complement, antiphospholipid) adds points
- Score ≥10 = classify as SLE
Even without a full SLE score, the patient may have UCTD - defined as ANA positive + ≥1 clinical CTD feature without fulfilling any specific CTD criteria. About 25% of UCTD patients progress to a defined CTD (most commonly SLE) over time, per [Firestein & Kelley's Textbook of Rheumatology (2022)].
Step 7: Initial Management While Workup is Ongoing
Even before a definitive label:
- NSAIDs - if not already tried adequately; use with gastroprotection
- Hydroxychloroquine (HCQ) 200-400 mg/day - indicated for joint symptoms and systemic inflammation in ANA+ CTD/undifferentiated lupus; reduces risk of progression to SLE, protects against thrombosis; requires baseline ophthalmology review
- Low-dose prednisolone (5-10 mg/day) - if severe inflammation not controlled, short course
- Sunscreen + sun protection - important for any suspected lupus
- Avoid triggers - estrogen-containing OCP (can flare SLE), sulfonamides
Step 8: Follow-up & Monitoring Plan
- Repeat ANA, anti-dsDNA, C3/C4, CBC, urinalysis every 3-6 months even if workup is initially negative - early UCTD can evolve
- Monitor for new clinical features: rash, serositis, renal symptoms, neuropsychiatric features
- If HLA-B27 positive with inflammatory back pain pattern, refer for spondyloarthropathy evaluation
- Rheumatology referral is mandatory - this patient needs specialist co-management
Summary Algorithm
ANA+ polyarthralgia + raised ESR/CRP + RA-
↓
Step 1: Anti-dsDNA + ENA panel + C3/C4 + APS antibodies
Step 2: CBC, urine R/M, urine protein
Step 3: HLA-B27, anti-CCP, TSH
Step 4: X-ray joints + MRI SI joints
Step 5: Score EULAR/ACR 2019 SLE criteria
↓
Score ≥10 → SLE
ANA+ + CTD features, no full criteria → UCTD
Anti-Ro/La + sicca symptoms → Sjogren's
High anti-U1-RNP → MCTD
HLA-B27+ + inflammatory back pain → SpA overlap
Key take-away: This young woman almost certainly has an autoimmune CTD. The ANA positivity with polyarthralgia and raised acute-phase reactants demands a full CTD serologic panel - specifically anti-dsDNA, ENA panel, complement levels, and APS antibodies. Simultaneously, complete a CBC, urine microscopy, and MRI sacroiliac joints given the back pain. Start hydroxychloroquine early while awaiting results. Refer to rheumatology.
- Firestein & Kelley's Textbook of Rheumatology, 2022 - Chapter on Undifferentiated CTD and Overlap Syndromes
- Goldman-Cecil Medicine - Table 245, SLE Classification Criteria (2019 EULAR/ACR)
- Harrison's Principles of Internal Medicine 22E - Sjogren's Syndrome, RA Differential Diagnosis
Treatment regimen for sle and uctd
Finding Sources
Finding Sources
Searching PubMed
"systemic lupus erythematosus" AND treatment
Reading File
Finding Sources
Reading Article
PMID: 41182321
Reading Article
PMID: 41107121
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive data from authoritative sources including the 2025 ACR Guideline, 2025 EULAR update, Harrison's 22E, and the Rheumatology textbook. Let me compile the full treatment guide.
Treatment Regimen for SLE and UCTD
PART 1: TREATMENT OF SLE
Treatment Goals (Treat-to-Target)
Per 2025 ACR Guideline (PMID: 41182321) and Harrison's 22E:
- Remission: SLEDAI-2K = 0, on HCQ ± stable immunosuppressive, prednisone ≤5 mg/day (DORIS criteria)
- Low Disease Activity State (LLDAS): SLEDAI ≤4, prednisone ≤7.5 mg/day - attainable in up to 80% of patients
- Minimize glucocorticoid exposure - even 5 mg/day prednisolone causes long-term damage accrual
- Prevent flares, organ damage, and cardiovascular events
A. General Measures (ALL Patients, Lifelong)
| Measure | Rationale |
|---|---|
| Daily broad-spectrum sunscreen (SPF ≥30) on all sun-exposed areas | UV light triggers SLE flares via keratinocyte apoptosis and autoantigen release |
| Avoid smoking | Tobacco reduces antimalarial efficacy |
| Balanced diet, maintain healthy weight | Reduces cardiovascular risk |
| Regular aerobic exercise | Reduces fatigue, cardiovascular risk, damage |
| Blood pressure control (target <130/80 mmHg) | Cardiovascular disease is the leading cause of late mortality in SLE |
| Lipid control (statin if indicated) | Accelerated atherosclerosis in SLE - statin reduces all-cause mortality in lupus nephritis patients post-transplant |
| Glucose monitoring | Steroid-induced DM risk |
| Vaccinations (influenza, pneumococcal, COVID-19, HBV) | Immunosuppression increases infection risk; avoid live vaccines when on IS |
| Avoid OCP (high-dose estrogen) | Can trigger flares; low-dose or progestogen-only pills are acceptable if no APS |
| Aspirin/VKA | If antiphospholipid antibody positive or APS confirmed |
| Ophthalmology review before starting HCQ | Baseline retinal screen |
B. Hydroxychloroquine (HCQ) - The Cornerstone Drug
Given to ALL SLE patients unless contraindicated (per 2025 ACR, EULAR, Harrison's).
| Parameter | Details |
|---|---|
| Dose | Up to 5 mg/kg/day actual body weight (typically 200-400 mg/day) |
| Route | Oral |
| Mechanism | Toll-like receptor inhibitor, lysosomal alkalinization, anti-inflammatory |
| Benefits | Prevents flares, reduces organ damage, lowers thrombosis risk, improves survival, reduces renal disease incidence, safe in pregnancy and breastfeeding |
| Monitoring | Baseline ophthalmology + annual retinal exams (risk of maculopathy with prolonged use); CBC, renal function |
| Cautions | G6PD deficiency, pre-existing retinopathy, QTc prolongation |
| Alternative antimalarials | Chloroquine (higher retinal toxicity), Quinacrine (add-on or if HCQ retinopathy develops) |
C. Glucocorticoids (GC) - Bridge Therapy, NOT Long-term
| Situation | Dose |
|---|---|
| Mild flare / arthritis | Prednisolone 5-15 mg/day PO, taper rapidly |
| Moderate active disease | Prednisolone 0.5 mg/kg/day (max 40 mg), taper to ≤5 mg/day within 3-6 months |
| Severe organ-threatening disease | IV methylprednisolone 125-1000 mg/day × 1-3 days (pulse), then oral prednisolone |
| Maintenance target | ≤5 mg/day prednisolone equivalent, or discontinue |
Key principle from Harrison's 22E: "If corticosteroids are utilized, the goal should be to use the lowest possible dose to suppress disease activity... taper as quickly as possible and withdraw as soon as feasible."
D. Disease-Modifying Treatment by Severity
The chart below (from the EULAR/Fanouriakis recommendations, reproduced in Harrison's 22E) summarizes the approach:
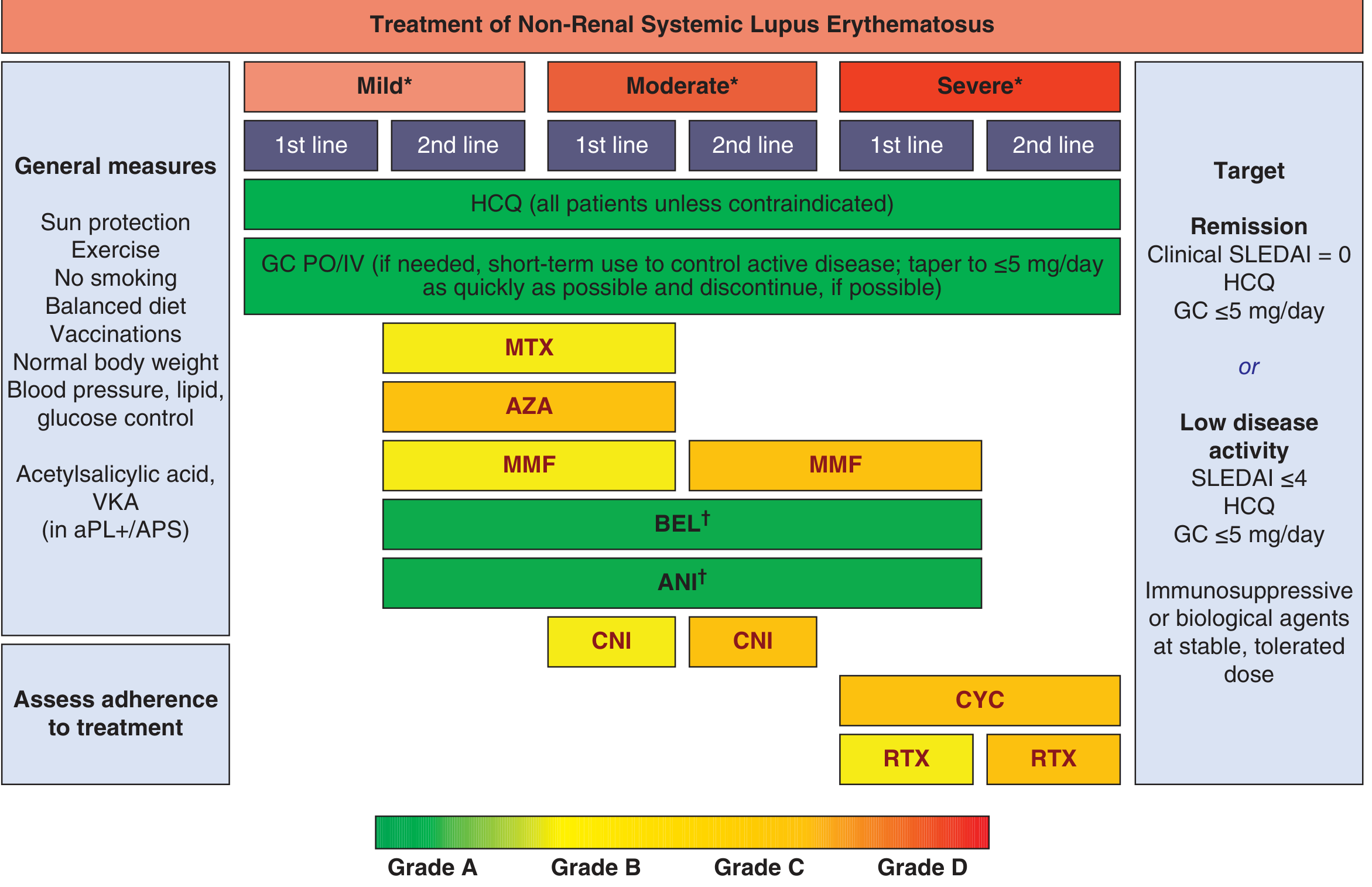
Mild SLE (SLEDAI ≤6; skin, arthritis, fatigue, mild serositis)
| Line | Drug | Dose |
|---|---|---|
| 1st | HCQ | 5 mg/kg/day |
| 1st | NSAIDs (short-term) | With gastroprotection; caution - aseptic meningitis, renal risk in SLE |
| 1st | Short-course low-dose GC | Prednisolone 5-10 mg to bridge |
| 2nd (if unresponsive) | Methotrexate (MTX) | 7.5-20 mg/week + folic acid 5 mg/week |
| 2nd | Azathioprine (AZA) | 1-2.5 mg/kg/day |
| 2nd | Mycophenolate mofetil (MMF) | 1-2 g/day |
Moderate SLE (SLEDAI 7-12; polyarthritis, significant skin, serositis, cytopenias)
| Line | Drug | Dose |
|---|---|---|
| 1st | HCQ + low-dose GC | As above |
| 1st | MMF (equivalent to AZA, MTX) | 1.5-2 g/day |
| 1st | Belimumab (BEL) | 10 mg/kg IV every 2 weeks × 3, then monthly OR 200 mg SC weekly |
| 1st | Anifrolumab (ANI) | 300 mg IV every 4 weeks |
| 2nd | Calcineurin inhibitors (CNI) - tacrolimus, voclosporin | Tacrolimus 3-4 mg/day |
Severe SLE (SLEDAI >12; renal, CNS, vasculitis, severe hematologic)
| Line | Drug | Dose |
|---|---|---|
| 1st | HCQ + GC pulse + aggressive IS | IV methylprednisolone 500-1000 mg × 3 days |
| 1st | Cyclophosphamide (CYC) | Low-dose Euro-Lupus: 500 mg IV q2 weeks × 6 doses OR High-dose NIH: 0.5-1 g/m² IV monthly × 6 |
| 1st | Rituximab (RTX) | 1 g IV × 2 doses, 2 weeks apart (off-label but widely used) |
| 2nd | Rituximab (if CYC failed) | Repeat cycles |
| Note | Belimumab and anifrolumab are NOT recommended for severe neuropsychiatric SLE | - |
E. Organ-Specific Treatment
Lupus Nephritis (Class III/IV - Proliferative)
Per 2025 EULAR update (PMID: 41107121):
Induction (first 6 months):
| Regimen | Details |
|---|---|
| MMF (preferred especially in Black/Hispanic) | 2-3 g/day + IV methylprednisolone 500-1000 mg × 3 days, then prednisolone 0.3-0.5 mg/kg/day tapering |
| Low-dose CYC (Euro-Lupus) | 500 mg IV q2 weeks × 6 pulses + GC as above |
| High-dose CYC (NIH) | For poor prognostic features (crescents, fibrinoid necrosis, low eGFR) |
| Add Belimumab to MMF/low-dose CYC | Superior outcomes; 10 mg/kg IV or 400 mg SC |
| Add Voclosporin (CNI) to MMF | 23.7 mg orally twice daily - improved complete renal response |
Maintenance (after 6-12 months of remission):
| Drug | Dose |
|---|---|
| MMF (preferred) | 1-2 g/day |
| AZA (if pregnancy planned) | 1-2 mg/kg/day |
| Belimumab add-on | Continue if used during induction |
| Continue HCQ | All patients |
| Continue ACEi/ARB | Renoprotection, reduce proteinuria |
| Consider SGLT2 inhibitor | If eGFR reduced - reduces glomerular hyperfiltration and proteinuria |
Response milestones (EULAR 2025):
- 3 months: ≥25% reduction in urine protein:creatinine ratio (UPCR)
- 6 months: ≥50% reduction in UPCR to <3 g/day
- 12-24 months: UPCR <0.5-0.7 g/day + eGFR within 10% of baseline
Neuropsychiatric Lupus (CNS Vasculitis, Seizures, Psychosis)
- IV methylprednisolone pulse + IV cyclophosphamide
- Anticonvulsants for seizures
- Antipsychotics for psychosis (distinguish from steroid-induced psychosis)
- If APS-related: anticoagulation (VKA, target INR 2.5-3.5)
- Avoid belimumab and anifrolumab in severe NP-SLE
Hematologic (AIHA, Thrombocytopenia)
- IV methylprednisolone + IVIG (for emergencies)
- Rituximab for refractory cases
- Splenectomy as last resort
F. Biologic & Targeted Therapies (Summary)
| Drug | Class | Indication | Dose |
|---|---|---|---|
| Belimumab | Anti-BAFF | Moderate-severe non-renal SLE; lupus nephritis (add-on to MMF/CYC) | 10 mg/kg IV monthly OR 200 mg SC weekly |
| Anifrolumab | Anti-type I IFN receptor | Moderate-severe skin and musculoskeletal SLE (NOT CNS disease) | 300 mg IV q4 weeks |
| Rituximab | Anti-CD20 | Refractory/severe SLE, lupus nephritis, refractory cytopenias | 1 g IV × 2, 2 weeks apart |
| Voclosporin | Calcineurin inhibitor | Lupus nephritis (add-on to MMF) | 23.7 mg PO BD |
| Obinutuzumab | Anti-CD20 (type II) | Refractory lupus nephritis | Per protocol |
G. Drug Monitoring Table
| Drug | Key Monitoring |
|---|---|
| HCQ | Annual eye exam, CBC |
| Prednisolone | BP, glucose, bone density (DEXA if >3 months use), eye exam (cataracts) |
| MTX | LFTs, CBC q4-8 weeks; avoid in renal impairment |
| AZA | CBC, LFTs q4-8 weeks; TPMT genotyping before starting |
| MMF | CBC, LFTs, renal function monthly initially |
| CYC | CBC, urinalysis (hemorrhagic cystitis - mesna prophylaxis), ovarian protection |
| Belimumab | Infusion reactions, infections |
| Anifrolumab | Herpes zoster prophylaxis recommended |
PART 2: TREATMENT OF UCTD
Principles
UCTD is ANA-positive with ≥1 CTD clinical feature but not fulfilling criteria for any defined CTD. Per [Firestein & Kelley's Textbook of Rheumatology (2022)]:
- ~25% progress to a defined CTD (most commonly SLE) within 5 years
- Predictors of progression to SLE: anti-dsDNA+, anti-Sm+, homogeneous ANA pattern, discoid lesions, serositis, younger age, African American ethnicity
- The majority (>50%) remain undifferentiated or stabilize
Treatment Goals in UCTD
- Control symptoms (arthralgia, fatigue, myalgia)
- Prevent progression to defined CTD
- Minimize side effects - avoid over-treating an undifferentiated condition
- Regular monitoring for evolution
UCTD Treatment Algorithm
| Situation | Treatment |
|---|---|
| All patients | Sun protection, lifestyle measures, patient education |
| Arthralgia/arthritis | NSAIDs first (with gastroprotection) |
| Persistent symptoms despite NSAIDs | Hydroxychloroquine 200-400 mg/day - first choice; reduces risk of progression to SLE, controls joint symptoms, fatigue, and skin manifestations |
| Refractory arthralgia/myalgia | Low-dose prednisolone 5-7.5 mg/day (short course) |
| Persistent arthritis not responding to HCQ | Methotrexate 7.5-15 mg/week |
| Raynaud's phenomenon | Nifedipine (calcium channel blocker), amlodipine; avoid cold exposure |
| Sicca symptoms | Artificial tears, pilocarpine |
| Confirmed progression to defined CTD | Treat as per that specific disease (SLE, SSc, Sjogren's, etc.) |
Monitoring Schedule for UCTD
| Interval | What to Check |
|---|---|
| Every 3-6 months | Clinical review for new CTD features (rash, renal symptoms, serositis, neurological symptoms) |
| Every 6-12 months | ANA titer, anti-dsDNA, C3/C4, CBC, urine R/M, ESR/CRP |
| Annually | ENA panel reassessment if new features appear |
| As needed | Imaging if new symptoms develop |
Red Flags in UCTD Requiring Urgent Re-evaluation
- New proteinuria or hematuria - lupus nephritis developing
- Malar/discoid rash appearing
- New serositis (pleuritis, pericarditis)
- Rising anti-dsDNA or falling complement
- Thrombocytopenia or hemolytic anemia on CBC
- Raynaud's + puffy fingers (early SSc)
Quick Reference Summary
UCTD:
NSAIDs → HCQ 200-400 mg/day → Low-dose prednisolone → MTX
Monitor every 3-6 months for evolution to defined CTD
SLE - MILD:
HCQ + NSAIDs → Add MTX/AZA/MMF → BEL or ANI
SLE - MODERATE:
HCQ + GC (taper fast) + MMF/AZA/MTX → BEL + ANI
SLE - SEVERE (non-renal):
IV pulse GC + CYC or RTX
SLE - LUPUS NEPHRITIS:
HCQ + IV GC + MMF or Low-dose CYC ± Belimumab ± Voclosporin
Maintenance: MMF or AZA + ACEi/ARB + HCQ
TARGET:
Remission (SLEDAI = 0) or LLDAS (SLEDAI ≤4)
Prednisolone ≤5 mg/day
Sources:
- Harrison's Principles of Internal Medicine 22E (2025) - Chapter 368 (SLE Management)
- Firestein & Kelley's Textbook of Rheumatology (2022) - Chapter 87 (Overlap Syndromes, UCTD)
- 2025 ACR Guideline for Treatment of SLE (PMID: 41182321) - Sammaritano et al., Arthritis Care Res, 2026
- 2025 EULAR Recommendations for SLE with Kidney Involvement (PMID: 41107121) - Fanouriakis et al., Ann Rheum Dis, 2026
This is a shared conversation. Sign in to Orris to start your own chat.