Give answer on coal worker pneumoconiosis from fishman and murray only for md exam answer 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed. Here is the comprehensive MD exam answer on Coal Worker's Pneumoconiosis from Fishman's and Murray & Nadel's:
Coal Worker's Pneumoconiosis (CWP)
[MD Examination Answer - 10 Marks]
1. Definition and Terminology
Coal mine dust lung disease (CMDLD) is a spectrum of chronic lung diseases caused by prolonged excessive exposure to coal mine dust. Classic coal workers' pneumoconiosis (CWP) is one manifestation, characterized by small nodules or masslike lesions and obstructive lung disease. CMDLD also encompasses COPD and dust-related diffuse fibrosis (DDF). Historically called "miners' asthma," "phthisis," "anthracosis," and "black lung," the modern understanding is that it is a preventable occupational disease.
(Murray & Nadel's, p. 2347; Fishman's, p. 1546)
2. Etiology and Dust Composition
Coal is a heterogeneous material - high in carbon but containing silica, silicates (mica, kaolinite), metals, and volatile hydrocarbons. Coal miners are exposed to mixed dusts including respirable crystalline silica (RCS), generated when miners cut through siliceous layers above, below, and within coal seams.
Coal is classified by rank (geologic age, carbon content):
- Peat - lowest rank (softest, newest)
- Bituminous - intermediate
- Anthracite - highest rank (hardest, oldest)
Higher coal rank and higher RCS component both increase disease risk. Modern continuous mining machinery generates larger quantities of RCS compared to older drilling/blasting methods, potentially worsening disease risk.
(Murray & Nadel's, p. 2347; Fishman's, p. 1546)
3. Pathology
Simple CWP begins as the coal macule - a collection of dust-laden macrophages containing reticulin and collagen, located within the wall of respiratory bronchioles, surrounded by centrilobular (focal) emphysema. Compared to macules, coal nodules contain a greater degree of collagen and are not confined to respiratory bronchioles. Macronodules measure 7 mm and larger; micronodules are up to 7 mm.
Progressive Massive Fibrosis (PMF) - the complicated form - is confirmed pathologically when one or more nodules attain a size of ≥2 cm in diameter (at autopsy). Radiographically, PMF is defined by opacities >1 cm. PMF lesions are:
- Solid, heavily pigmented, rubbery to hard
- Upper lobe predominant (though ~25% occur in middle/lower zones)
- May cavitate - raising concern for mycobacterial/fungal superinfection
- Airways and vessels adjacent to lesions are distorted; within lesions they are destroyed
- Associated with background changes of simple CWP
Dust-Related Diffuse Fibrosis (DDF) - described as a bridging fibrosis connecting various stages of CMDLD lesions; found in ~12% of coal miners at autopsy. Radiographically shows lower lung zone-predominant reticular disease, similar to UIP.
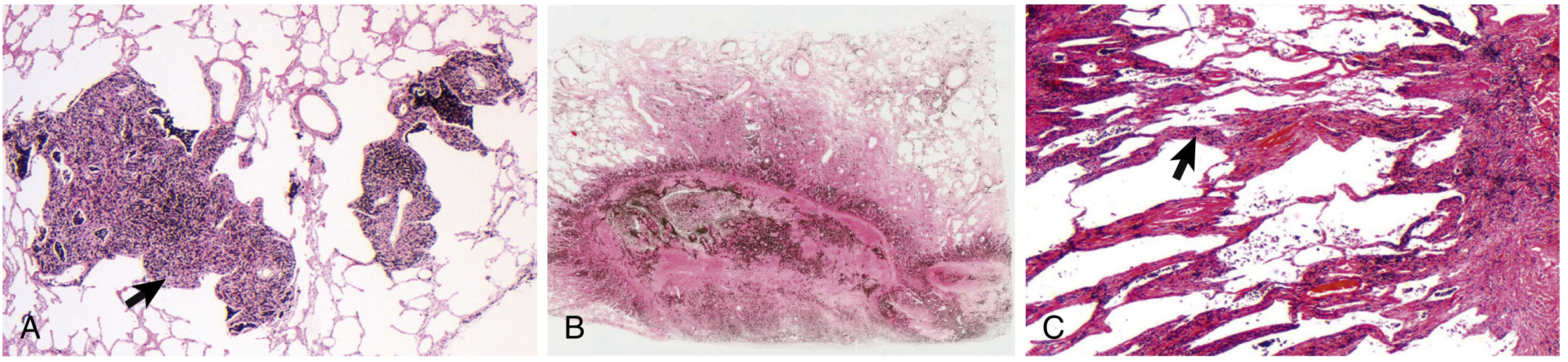
Figure - Pathologic lesions of CMDLD (Murray & Nadel's, p. 2348)
(Fishman's, p. 1547-1548; Murray & Nadel's, p. 2347-2348)
4. Epidemiology and Natural History
In the United States, after modern dust-control regulations were introduced, CWP prevalence declined from nearly one-third of working miners with 25 years tenure in the 1970s to less than 5% in the 1990s. However, simple CWP has since increased to >10% nationally and >20% in central Appalachian states (Kentucky, Virginia, West Virginia). The rate of PMF has also risen to levels not seen since the institution of modern dust controls.
Risk factors for developing CWP:
- Cumulative coal mine dust exposure (most important factor)
- Higher coal rank
- Greater RCS exposure
- Duration of exposure (typically at least 10 years needed for diagnosis)
- Older age and higher baseline profusion of simple CWP opacities (for PMF progression)
Rapidly progressive pneumoconiosis is defined as radiographic progression of more than one ILO profusion subcategory within 5 years, or development of PMF after 1985. It is concentrated in central Appalachia and histologically shows silicosis and mixed-dust pneumoconiosis patterns.
(Murray & Nadel's, p. 2347-2348; Fishman's, p. 1546)
5. Biology and Pathogenesis
Central to CMDLD biology is the alveolar macrophage. Dust particles reaching the distal airways are engulfed by alveolar macrophages and cleared via lymphatics. With excessive dust exposure, this system is overwhelmed - coal mine dusts and dust-laden macrophages accumulate in airway walls and interstitium, causing increasing fibrotic lesions.
Key immunologic findings:
- Elevated serum ANA (17%) and RF (10%) in miners with pneumoconiosis - ANA is 9% in simple CWP, rising to 27% in PMF (category C); RF 6% in simple CWP, 18% in category C
- Elevated BAL and serum IL-1β, IL-6, TNF-α (cytokines driving inflammation and fibrosis)
- Oxidative stress mediated by bioavailable iron (catalyzes oxidant formation)
- Elevated C3, α1-antitrypsin, IgA, IgG in miners with PMF (especially anthracite miners)
Host susceptibility factors remain poorly understood; specific genetic markers have not been confirmed, though polymorphisms in IL-18 may be protective.
(Fishman's, p. 1547-1548)
6. Clinical Features
The clinical presentation is variable:
- Simple CWP: Often asymptomatic, detected on screening radiograph
- Chronic cough and sputum production: Related to bronchitic changes - thickened airway walls, mucus gland enlargement, hypersecretion; chronic bronchitis in ~35% of seasoned US miners
- Dyspnea: With more severe airflow obstruction or advanced pneumoconiosis
- Cor pulmonale: Muscular thickening of pulmonary arteries with right ventricular hypertrophy; can occur in both simple and complicated CWP
- Melanoptysis (expectoration of black sputum): Rare but unique; results from excavation and liquefaction of a PMF lesion - harmless but alarming to patients
- Clubbing and crackles are NOT typical features of CWP - if present, they should prompt further investigation (e.g., chronic interstitial pneumonia)
No specific laboratory test exists for CMDLD. Levels of ACE, ANA, or RF may be abnormal.
(Fishman's, p. 1548; Murray & Nadel's, p. 2349)
7. Radiological Features
The ILO classification system (International Labour Office) is used to categorize radiographic changes, including standard radiographs for comparison. Digitally acquired images on a high-resolution viewing system are now accepted (since 2011).
Simple CWP:
- Small pneumoconiotic opacities, 1-9 mm in diameter
- 62% show mainly rounded (p, q, r type) opacities; 38% predominantly irregular
- Upper zone predominant, but significant proportions have lower zone or irregular lesions
Complicated CWP / PMF:
- One or more opacities >1 cm in long-axis diameter
- Upper zone predominant; ~25% confined to middle and/or lower zones
- Bilateral distribution with progressive disease
- Architectural distortion, emphysema, volume loss in severe disease
- PMF is always associated with background smaller opacities
HRCT is more sensitive for emphysema, early pulmonary fibrosis, and evaluation of symptomatic workers with normal/borderline CXR. PMF can mimic malignancy; PET scanning is not reliably discriminatory (PMF may also show increased FDG uptake).
(Fishman's, p. 1548-1549; Murray & Nadel's, p. 2348-2349)
8. Pulmonary Function
There is no characteristic pattern of physiologic abnormality in CMDLD, reflecting its heterogeneous manifestations.
- Simple CWP with small rounded opacities: Generally no significant lung function impairment in early disease (contrary to prior dogma, profusion of simple opacities is associated with reduced lung function)
- PMF: Moderate-to-severe restriction or mixed obstructive-restrictive pattern
- Diffusing capacity (DLCO): Small rounded opacities do not generally impair DLCO; larger opacities of PMF reduce it significantly
- Coal mine dust exposure is associated with lung function impairment even in the absence of radiographic CWP
- The magnitude of FEV1 decline is proportional to cumulative dust exposure; the correlation is greater in nonsmokers
- FEV1 decline is of the same order of magnitude as that caused by tobacco smoke
- Emphysema: Centrilobular emphysema is the most common type associated with coal dust; all pathologic types (centriacinar, panacinar, bullous) are associated with dust exposure; cigarette smoking adds an additive effect
(Fishman's, p. 1549; Murray & Nadel's, p. 2349)
9. Complications
| Complication | Notes |
|---|---|
| Progressive Massive Fibrosis (PMF) | Commonest serious complication; may cavitate |
| Emphysema | Centrilobular; severity proportional to dust load |
| Caplan Syndrome (Rheumatoid Pneumoconiosis) | Association of CWP with rheumatoid arthritis; large well-defined nodules 5-50 mm; <1% of autopsied cases |
| Cor pulmonale / Pulmonary hypertension | Can occur in both simple and complicated CWP |
| Tuberculosis | Increased risk in coal miners (mainly due to silica component); cavitary PMF warrants mycobacterial workup |
| Lung Cancer | More recent studies suggest association between coal mine dust/silica exposure and bronchogenic carcinoma |
| DDF | Lower zone reticular fibrosis; less aggressive than IPF |
Caplan Syndrome is an uncommon manifestation seen in less than 1% of autopsied cases. The chest radiograph shows large, well-defined nodules or masses (5-50 mm), typically without a background of smaller opacities (distinguishing it from PMF).
(Fishman's, p. 1548; Murray & Nadel's, p. 2349)
10. Diagnosis
Diagnosis is made on the basis of:
- Compatible radiographic findings (ILO classification)
- History of coal mine dust exposure (at least 10 years, though shorter high-intensity exposures may cause disease)
- Exclusion of alternative diagnoses when atypical features are present
Lung biopsy is NOT routinely indicated. Surgical biopsy may be appropriate when there is diagnostic uncertainty, particularly to exclude malignancy. Biopsy material should be examined under polarized light microscopy or submitted for mineralogic analysis. Histoplasmosis and miliary tuberculosis should be considered when profuse small opacities are present.
(Murray & Nadel's, p. 2349-2350; Fishman's, p. 1548)
11. Management
There is no specific treatment for CWP/CMDLD. Management is directed at:
- Removal from further exposure to coal dust and other respiratory hazards (secondary prevention)
- Smoking cessation - imperative
- Bronchodilators for COPD/airflow obstruction
- Oxygen supplementation in severe disease
- Lung transplantation - for end-stage disease
- Whole-lung lavage: Advocated to remove coal mine dust and inflammatory mediators; insufficient evidence to support routine use
- Monitoring: CMDLD may progress after cessation of exposure (PMF can develop or worsen even after leaving mining); regular physiologic and radiographic evaluation is required for all former coal miners
- Treatment of infections: Thorough sputum examination for typical and atypical mycobacteria in progressive/cavitary lesions
(Murray & Nadel's, p. 2350; Fishman's, p. 1549)
12. Prevention and Legal Aspects
The Federal Coal Mine Health and Safety Act of 1969 (United States) established mandatory standards for working conditions, enforcement, miner health monitoring, and financial compensation. The Black Lung Benefits Act (1972) defined pneumoconiosis as "a chronic dust disease of the lung and its sequelae, including respiratory and pulmonary impairments arising out of coal mine employment." Mines are now regulated by the Mine Safety and Health Administration (MSHA).
Total disability is defined as any one of: (1) Department of Labor thresholds of FEV1, FVC, FEV1/FVC, MVV, or arterial blood gas values; (2) presence of cor pulmonale; (3) radiographic evidence of complicated pneumoconiosis/PMF; (4) a reasoned medical opinion.
(Fishman's, p. 677)
Sources:
- Fishman's Pulmonary Diseases and Disorders, 5th edition (ISBN 9781260473940) - Chapters 36 and 87
- Murray & Nadel's Textbook of Respiratory Medicine, 7th edition (ISBN 9780323655873) - Chapter 101
This is a shared conversation. Sign in to Orris to start your own chat.