I have my university exam of 1 st year of subject physiology These are the important long answer give me answer of this question "Describe the referred & radiating pain. Explain the Gate Control Theory of Pain." and remeber it's a long question
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks (Guyton & Hall, Ganong's, Kandel's Principles of Neural Science, Neuroscience: Exploring the Brain). I have all I need to write a thorough exam answer.
Referred Pain, Radiating Pain, and the Gate Control Theory of Pain
INTRODUCTION
Pain is a complex sensory and emotional experience that arises from actual or potential tissue damage. Beyond the site of injury, pain can be perceived at distant locations - this gives rise to the clinically important concepts of referred pain and radiating pain. Understanding how pain signals are modulated in the spinal cord forms the basis of the Gate Control Theory. Together, these concepts are fundamental to both clinical diagnosis and pain management.
PART I: REFERRED PAIN
Definition
Referred pain is pain that is perceived at a body surface location that is anatomically distant from the actual site of tissue damage or disease. The patient feels pain "in the wrong place" - the organ responsible for generating the pain signal is not the organ at the location where pain is felt.
"Sometimes, a person feels pain in a part of the body that is fairly remote from the tissue causing the pain. This phenomenon is called referred pain. Knowledge of the different types of referred pain is important in clinical diagnosis because, in many visceral ailments, the only clinical sign is referred pain." - Guyton & Hall Textbook of Medical Physiology
Characteristics of Referred Pain
- Visceral origin - most commonly arises from diseased visceral (internal) organs
- Poorly localized - the patient cannot pinpoint the exact location
- Dull, aching quality - transmitted via slow unmyelinated C fibers
- Associated with cutaneous hyperalgesia - the skin over the referred area may become tender and hypersensitive
- Predictable patterns - referral follows dermatomal maps based on embryological origin
Classic Examples of Referred Pain
| Source Organ | Site of Referred Pain |
|---|---|
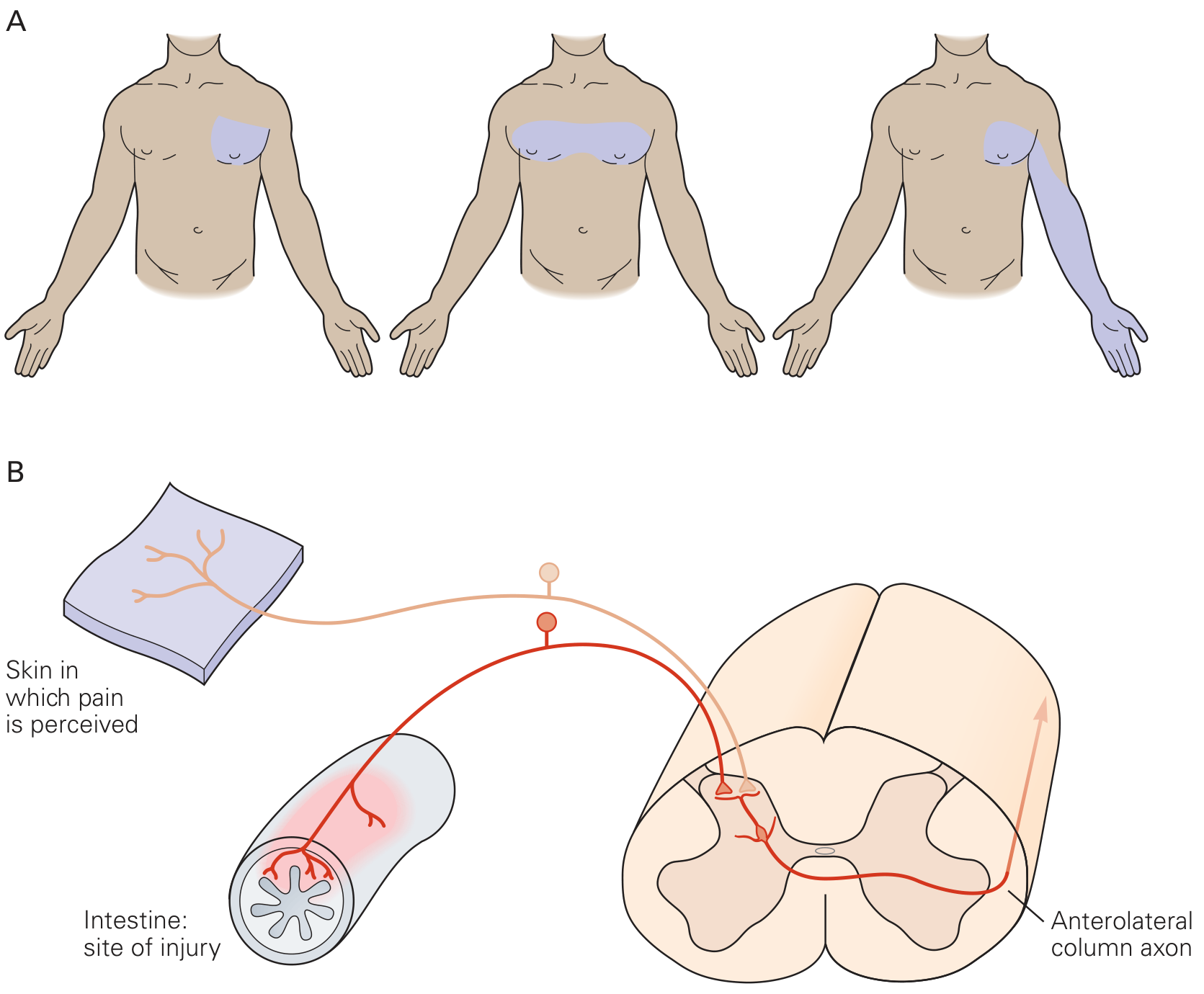
| Heart (myocardial infarction/angina) | Inner aspect of left arm, chest, jaw, neck |
| Diaphragm (central irritation) | Tip of shoulder (C4 dermatome) |
| Kidney / Ureter | Testis or labia (same embryological origin) |
| Gallbladder | Right shoulder/scapular area |
| Appendix | Umbilical region (T10 dermatome) - early phase |
| Pancreas | Back |
| Peptic ulcer | Epigastric region |
Ischemic cardiac pain is a particularly instructive example - it may be referred to the right arm, abdomen, back, neck, or jaw - demonstrating that referral sites are not always stereotyped.
Mechanism of Referred Pain - Convergence-Projection Theory
This is the most widely accepted explanation.
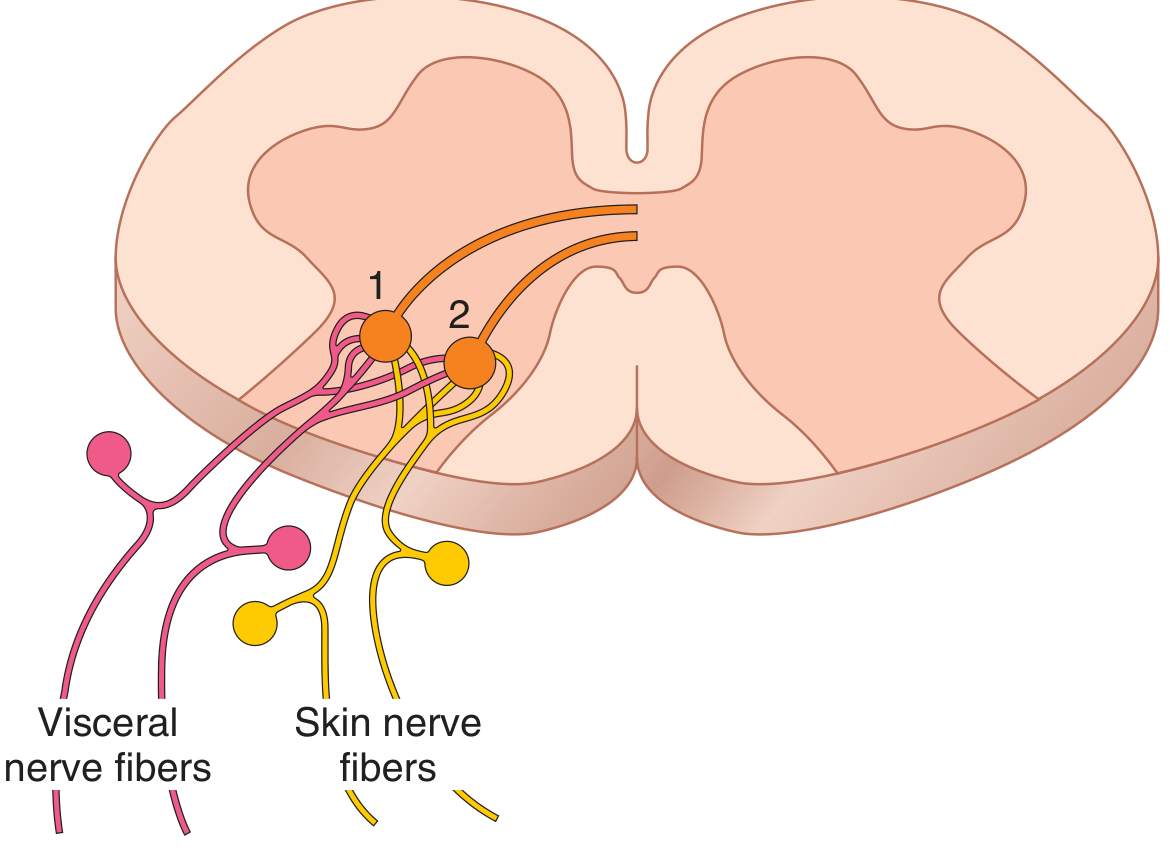
The Convergence-Projection Theory states:
- Both visceral pain fibers and somatic (skin) pain fibers from the same spinal segment synapse on the same second-order neurons (projection neurons) in the dorsal horn of the spinal cord
- These second-order neurons then project up the spinothalamic tract to the thalamus, and finally to the somatosensory cortex
- When visceral pain fibers are activated, the brain interprets the signal as coming from the skin (or somatic structure) - because the brain has been "trained" by a lifetime of cutaneous stimuli to associate those particular projection neurons with the corresponding skin area
- The brain cannot determine the true source of the stimulus and mistakenly attributes the pain to the somatic structure
As described in Ganong's Review of Medical Physiology:
"Somatic and visceral neurons converge in the ipsilateral dorsal horn. When the visceral stimulus is prolonged, facilitation of activity from the somatic fiber endings occurs. They now stimulate the second-order neurons, and of course the brain cannot determine whether the stimulus came from the viscera or from the area of referral."
Embryological Basis of Referred Pain Patterns
The pattern of referral is not random - it follows embryological segmental organization:
- Pain is usually referred to a structure that developed from the same embryonic segment (dermatome) as the painful organ
- The heart and the arm share the same spinal segmental origin (C8-T1/T2) - explaining cardiac pain referred to the arm
- The testicle migrated with its nerve supply from the primitive urogenital ridge, from which the kidney and ureter also developed - explaining testicular pain from ureteric pathology
Clinical Importance of Referred Pain
- It is often the only clinical sign of visceral disease
- Misdiagnosis is common if the clinician does not recognize referral patterns
- Referred hyperalgesia (increased sensitivity of referred area) can mislead the examining physician
- Always perform a thorough examination of the organ actually causing the pain, not just the region where pain is felt
PART II: RADIATING PAIN
Definition
Radiating pain (also called projected pain or radicular pain) is pain that travels or "radiates" from its point of origin along the course of a nerve or nerve root. Unlike referred pain, it follows a definite anatomical path corresponding to the distribution of the affected nerve.
Key Distinction from Referred Pain
| Feature | Referred Pain | Radiating Pain |
|---|---|---|
| Origin | Visceral (internal organ) | Nerve root or peripheral nerve |
| Pattern | Follows dermatome of same embryological segment | Follows the anatomical course of a specific nerve/nerve root |
| Quality | Dull, aching, poorly localized | Sharp, shooting, burning, lancinating |
| Pathway | Via convergence of visceral + somatic fibers | Via irritation/compression of the nerve itself |
| Example | Cardiac pain to left arm | Sciatica - L4/L5/S1 nerve root pain down the leg |
Characteristics of Radiating Pain
- Sharp, stabbing, or shooting quality - often described as electric-shock-like
- Follows a dermatomal distribution - corresponds to a specific spinal level
- Associated neurological deficits - sensory loss, motor weakness, and reflex changes in the same dermatomal/myotomal distribution
- Exacerbated by nerve-stretching maneuvers - e.g., straight leg raise (Lasegue's sign) for sciatica, neck flexion for cervical radiculopathy
- Worsened by increased intraspinal pressure - coughing, sneezing, straining (Valsalva maneuver)
- Dermatomal localization helps identify the level of nerve root compression
Common Examples of Radiating Pain
- Sciatica - L4, L5 or S1 nerve root compression → pain radiating from the back, through the buttock, down the posterior/lateral leg to the foot
- Cervical radiculopathy - C6 root compression → pain radiating from the neck to the thumb
- Carpal tunnel syndrome - median nerve compression → pain/paresthesia radiating to the first three fingers
- Angina pectoris - left arm radiation (some overlap with referred pain)
- Herpes zoster (shingles) - radiating burning pain along a dermatome before rash appears
As described in Bradley and Daroff's Neurology:
"When a nerve root is irritated or injured, the projected pain is radicular. Radicular pain commonly has a sharp, stabbing quality or causes dysesthesia. It may be exacerbated by activities that stretch the affected nerve root."
PART III: GATE CONTROL THEORY OF PAIN
Historical Background
The Gate Control Theory was proposed in 1965 by Ronald Melzack (a psychologist) and Patrick Wall (a physiologist), then working at MIT. Prior to this, two competing theories existed:
- Specificity Theory - specific pain receptors send signals directly to the brain
- Pattern Theory - pain results from overactivation of any receptor
Melzack and Wall revolutionized pain science by proposing that pain transmission is not a simple relay - it is actively modulated (gated) at the level of the spinal cord dorsal horn.
Basic Premise
Pain signals are regulated by a "gate" in the dorsal horn of the spinal cord. This gate can be:
- Opened - allowing more pain signals to reach the brain
- Closed - preventing or reducing pain signal transmission
The state of the gate is determined by the relative balance of activity in large-diameter and small-diameter nerve fibers.
Nerve Fiber Types Involved
| Fiber Type | Diameter | Myelination | Function | Effect on Gate |
|---|---|---|---|---|
| Aβ fibers (large) | Large | Heavily myelinated | Touch, pressure, vibration (non-nociceptive) | CLOSE the gate (inhibit pain) |
| Aδ fibers (medium) | Medium | Thinly myelinated | Fast, sharp pain; temperature | OPEN the gate |
| C fibers (small) | Small | Unmyelinated | Slow, burning, aching pain (nociceptive) | OPEN the gate |
Components of the Gate Control Circuit
Three key cell types in the dorsal horn:
- Primary afferent fibers (Aβ and C fibers) - bring signals from the periphery
- Inhibitory interneuron (Substantia Gelatinosa cell, lamina II of dorsal horn) - acts as the "gate keeper"
- Projection neuron (Transmission/T cell) - sends pain signals up the spinothalamic tract to the brain
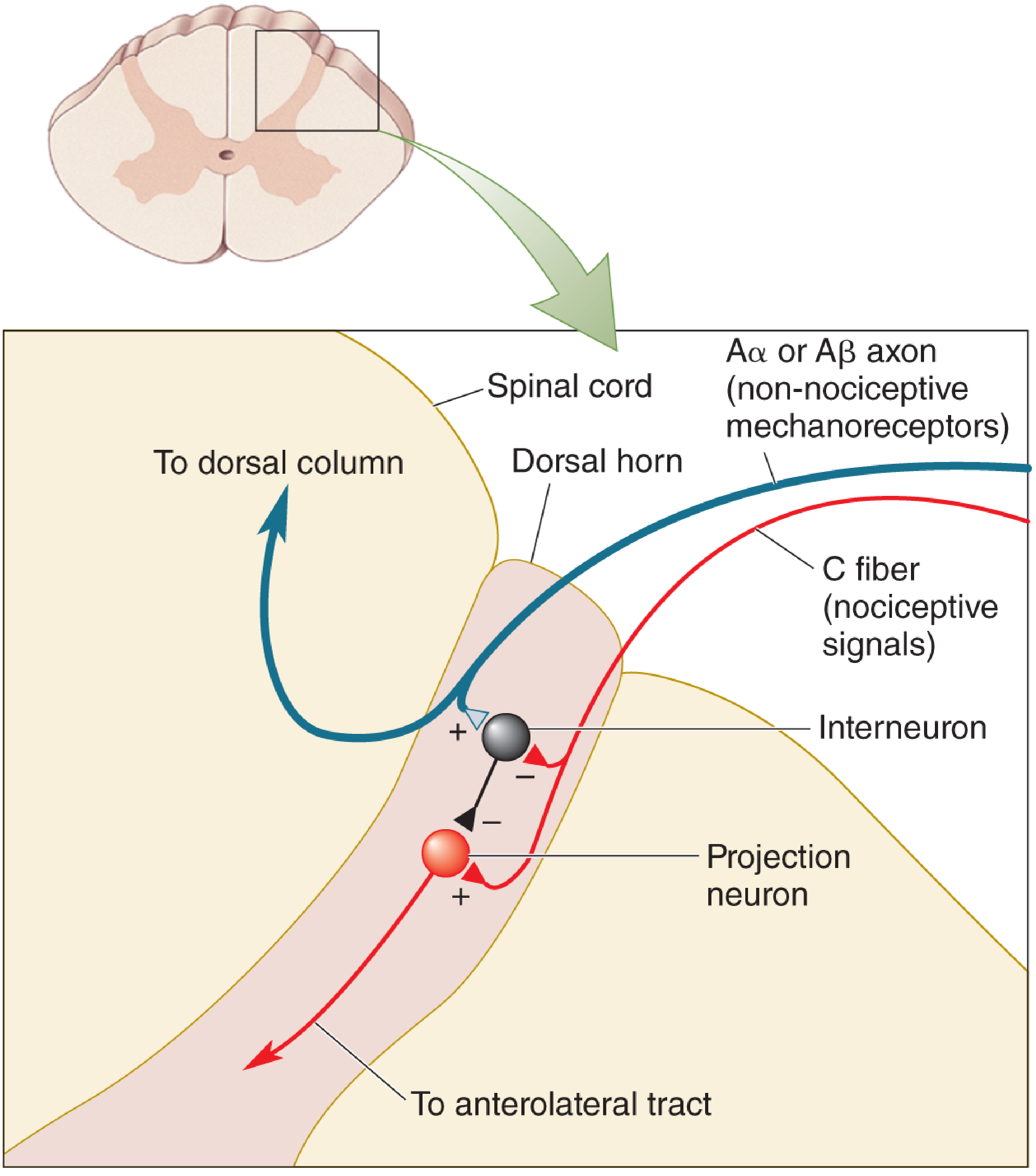
Mechanism of the Gate - Step by Step
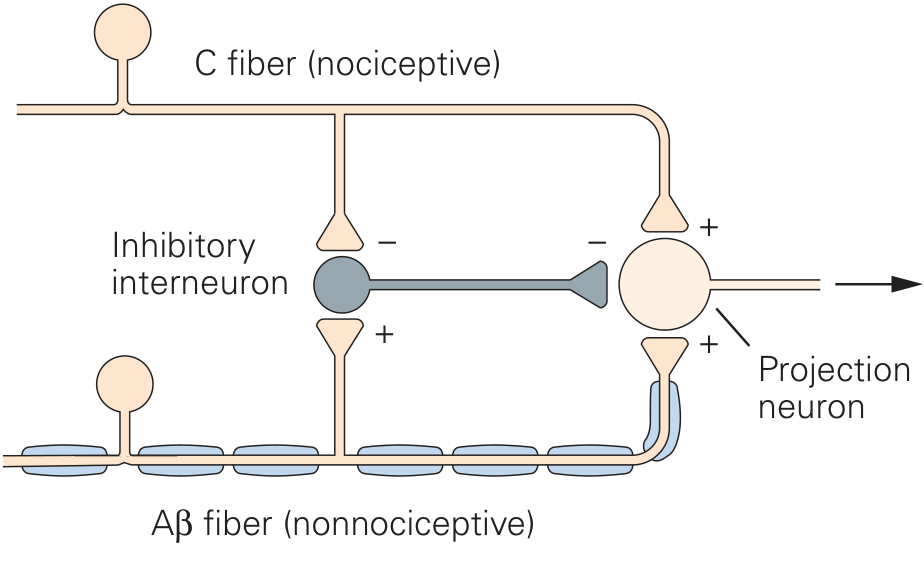
When C fibers (pain fibers) are active - Gate OPENS:
- C fibers directly excite the projection neuron (+) → pain signal travels to brain
- C fibers simultaneously inhibit the inhibitory interneuron (-)
- Inhibitory interneuron is now suppressed, so it cannot inhibit the projection neuron
- Result: projection neuron fires strongly → pain is perceived
When Aβ fibers (touch fibers) are active - Gate CLOSES:
- Aβ fibers excite the inhibitory interneuron (+)
- The activated inhibitory interneuron now inhibits the projection neuron (-)
- The projection neuron is suppressed and cannot fire
- Result: pain signals are blocked → pain is reduced or abolished
As stated in Kandel's Principles of Neural Science:
"The C fibers indirectly inhibit the interneurons, thus increasing the activity of the projection neurons (thereby 'opening the gate'), whereas the Aβ fibers excite the interneurons, thus suppressing the output of the projection neurons (and 'closing the gate')."
The Substantia Gelatinosa (SG) as the Gate
- Located in Lamina I and II of the dorsal horn (Rexed's laminae)
- The inhibitory interneurons in the substantia gelatinosa are central to the gating mechanism
- SG cells tonically inhibit T-cells (transmission neurons)
- Large fiber (Aβ) input activates SG cells → more inhibition → gate closed
- Small fiber (C fiber) input inhibits SG cells → less inhibition → gate open
Descending Control (Supraspinal Modulation)
Melzack and Wall also recognized that the gate is influenced by descending signals from the brain:
- Periaqueductal gray (PAG) - stimulation produces profound analgesia
- Nucleus raphe magnus - releases serotonin in the dorsal horn → inhibits pain
- Rostral ventromedial medulla (RVM) - releases norepinephrine → inhibits pain
- Psychological factors (attention, emotion, expectation, memory) influence pain through descending pathways - explaining why soldiers wounded in battle may feel no pain initially
Clinical Applications of Gate Control Theory
| Application | Mechanism |
|---|---|
| Rubbing an injury (e.g., a bruised shin) | Activates Aβ mechanoreceptors → closes the gate |
| Transcutaneous Electrical Nerve Stimulation (TENS) | Electrodes activate large Aβ fibers → closes the gate |
| Spinal Cord Stimulation (SCS) | Stimulates dorsal columns (Aβ) → closes the gate |
| Acupuncture | May activate Aβ fibers and trigger endorphin release |
| Distraction / Cognitive focus | Descending cortical control closes the gate |
| Opioid analgesics | Act on mu-receptors in dorsal horn → suppress C fiber transmission |
| Emotional distress / anxiety | Removes descending inhibition → opens the gate, worsens pain |
Modifications and Limitations of the Original Theory
- The original 1965 model has been refined - interactions between large and small fibers also occur at supraspinal relay centers (thalamus, cortex), not just the spinal cord
- The exact wiring of the SG interneurons is more complex than originally proposed
- Central sensitization (wind-up phenomenon) was not fully accounted for in the original theory - prolonged C fiber activity leads to NMDA receptor activation and enhanced pain sensitivity
- Neuromatrix theory was later proposed by Melzack to account for phantom limb pain and chronic pain states not explained by peripheral input alone
Despite these limitations, the core principle - that pain-inducing signals are regulated by the balance of activity in convergent large and small sensory axons - has stood the test of time.
SUMMARY TABLE
| Feature | Referred Pain | Radiating Pain | Gate Control Theory |
|---|---|---|---|
| Definition | Pain felt distant from origin | Pain traveling along nerve course | Spinal modulation of pain signals |
| Mechanism | Convergence-projection (shared dorsal horn neurons) | Nerve/root irritation or compression | Balance of Aβ vs C fiber activity at dorsal horn |
| Quality | Dull, aching | Sharp, shooting, burning | - |
| Example | Cardiac pain to left arm | Sciatica down the leg | Rubbing a bruise relieves pain |
| Localization | Dermatomal (embryological) | Dermatomal (nerve distribution) | Substantia gelatinosa, dorsal horn |
| Clinical use | Diagnosis of visceral disease | Localizing nerve root level | TENS, SCS, opioids, acupuncture |
Sources: Guyton & Hall Textbook of Medical Physiology | Ganong's Review of Medical Physiology (26th ed.) | Kandel's Principles of Neural Science (6th ed.) | Neuroscience: Exploring the Brain (5th ed.) | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.