

Present this history in correct format and give me physical examination of this case
Reading File
Based on the notes in both images, here is the case presented in correct clinical format, followed by a structured Physical Examination:
CASE PRESENTATION
Patient Demographics
| Name | Rods Hassan |
| Age/Sex | 40 years, Male |
| Occupation | Driver |
| Address | Sachon Mohion, LT, Gulbarga Road No. 1 |
| Date of Admission | 27/04/2026 |
| Date of Examination | 29/04/2026 |
| Informant | Patient (reliable) |
| Diagnosis | ILQ – JY (Liver disease / Portal hypertension) |
| Ward | DCIB |
Chief Complaints
- Pain abdomen × 1 year — on and off, fatigue
- Diarrhoea — on and off
- Chest pain — with abdominal pain (4 years)
History of Present Illness
Patient is a 40-year-old male, driver by occupation, presenting with pain abdomen for 1 year — insidious, non-progressive onset. Pain is:
- Site: LLQ
- Onset: Insidious, non-progressive
- Character: Null (aching start)
- Radiation: After passing stool — medication used
- Duration/Timing: ~6 months
- Aggravating factors: Nil
- Relieving factors: Medication
Diarrhoea:
- Consistency: Semi-solid, undigested food
- Amount: Moderate amount
- No blood stained, no mucus
- Non-projectile
- Nausea (+), Flatulence (+)
- Takes O₂ (OTC)
- No aggravating factors
Past History
- No CLD — 8 years
- Hospitalized — on every hospitalization (2–3 passes); last hospitalized 4 times
- Went to RIMS, hospitalized (2019)
- ICU per 2d → Haematemesis / vomiting blood
- 150 ml hospitalized → often alcohol intake
- To SHMS
- Alcohol — 1 month's last → quadrate for R/o (8 gm base)
- All haematemesis (upper GI bleed) — hospitalised 4×
Investigations:
- Hospitalized → 4 weeks; closed transfusion done → 3 passes RBC (4 months)
No vaccination history
H/o: HTN, DM, Asthma, Thyroid disorder, TB, Jaundice, Hepatitis B, Hep C — referred 7 years ago (diagnosed at 10 years age)
Family History
- No informative family history
- Rad⁺: On every hospitalization → suggestive of HTE (haematemesis, confusion) — Diasonin, confusion
- 760 g per alcohol → 7 years started → 10 years age
Personal History
| Diet | Mixed diet |
| Bowel & Bladder | Normal |
| Appetite | Normal |
| Sleep | Daytime somnolence, restlessness |
| Allergy | Pollen allergy |
| Alcohol | 28 years of use; stopped 1 year ago; 1–2 bottles/day (~1 L), 1 unit = 60 mL/day |
| Smoking | Occasional smoker |
| Tobacco | Occasional tobacco chewing |
General Examination (from notes)
- Oriented to TPP (Time, Place, Person) — C/C oriented
- Dilated veins — peri-umbilical (caput medusae)
- Splenomegaly — palpable; 10 cm below costal margin in MCL
PHYSICAL EXAMINATION (Expected / Standard for this Case)
Given this is a case of chronic liver disease (CLD) with portal hypertension (alcohol-related cirrhosis), the physical examination should be documented as follows:
General Physical Examination
| Parameter | Finding |
|---|---|
| Consciousness | Conscious and cooperative / oriented to TPP |
| Built & Nourishment | Moderately built, moderately nourished |
| Pallor | Present / Absent (anaemia expected in GI bleed) |
| Icterus (Jaundice) | Present / Absent — assess scleral icterus |
| Cyanosis | Absent |
| Clubbing | Present (Grade I–II) — hepatic clubbing |
| Lymphadenopathy | Absent |
| Oedema | Bilateral pitting pedal oedema — present / absent |
| Leukonychia | May be present (hypoalbuminaemia) |
| Palmar erythema | May be present |
| Dupuytren's contracture | May be present (alcohol) |
| Parotid enlargement | May be present (alcohol) |
| Fetor hepaticus | Assess breath |
| Asterixis (flapping tremor) | Assess — suggest hepatic encephalopathy |
Vital Signs
| Parameter | Value |
|---|---|
| Pulse | ___ bpm, regular/irregular, volume, character |
| Blood Pressure | / mmHg |
| Temperature | ___ °F / afebrile |
| Respiratory Rate | ___ breaths/min |
| SpO₂ | ___% on room air |
Systemic Examination
Abdomen
| Finding | Details |
|---|---|
| Inspection | Distended / flat; dilated peri-umbilical veins (caput medusae); visible peristalsis absent; umbilicus — everted (if ascites present) |
| Palpation | Tenderness — LLQ; Splenomegaly — 10 cm below costal margin in MCL; Liver — palpable / not palpable (may be shrunken in cirrhosis); Fluid thrill / Shifting dullness — if ascites |
| Percussion | Spleen dull in left hypochondrium extending to lumbar; liver dullness — assess span; shifting dullness |
| Auscultation | Bowel sounds — present, normal / reduced; no bruit |
Cardiovascular System
| Finding | Details |
|---|---|
| Precordium | Normal |
| Heart sounds | S1 S2 heard, no murmurs |
| JVP | Normal / elevated |
Respiratory System
| Finding | Details |
|---|---|
| Chest | Bilateral air entry equal |
| Percussion | Resonant bilaterally |
| Auscultation | No added sounds / crepitations if aspiration |
Central Nervous System
| Finding | Details |
|---|---|
| Sensorium | Conscious, oriented to TPP |
| Higher functions | Intact / signs of encephalopathy |
| Asterixis | Present / Absent |
| Cranial nerves | Intact |
| Motor/Sensory | Normal |
Summary
This is a 40-year-old male, driver, with a 28-year history of significant alcohol intake, presenting with chronic abdominal pain, diarrhoea, fatigue, and recurrent haematemesis. Key findings pointing to alcoholic liver cirrhosis with portal hypertension include:
- Peri-umbilical caput medusae
- Massive splenomegaly (10 cm below costal margin in MCL)
- Recurrent upper GI bleeds (haematemesis) requiring multiple hospitalizations and ICU admissions
- History of blood transfusions (3 packs RBC)
- Daytime somnolence / restlessness (early encephalopathy)
- Past history of jaundice and hepatitis
Note (from examiner): Write H/o CVA — a history of cerebrovascular accident should also be documented.
Corticospinal tract
Finding Sources
Searching Images
corticospinal tract anatomy pathway
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
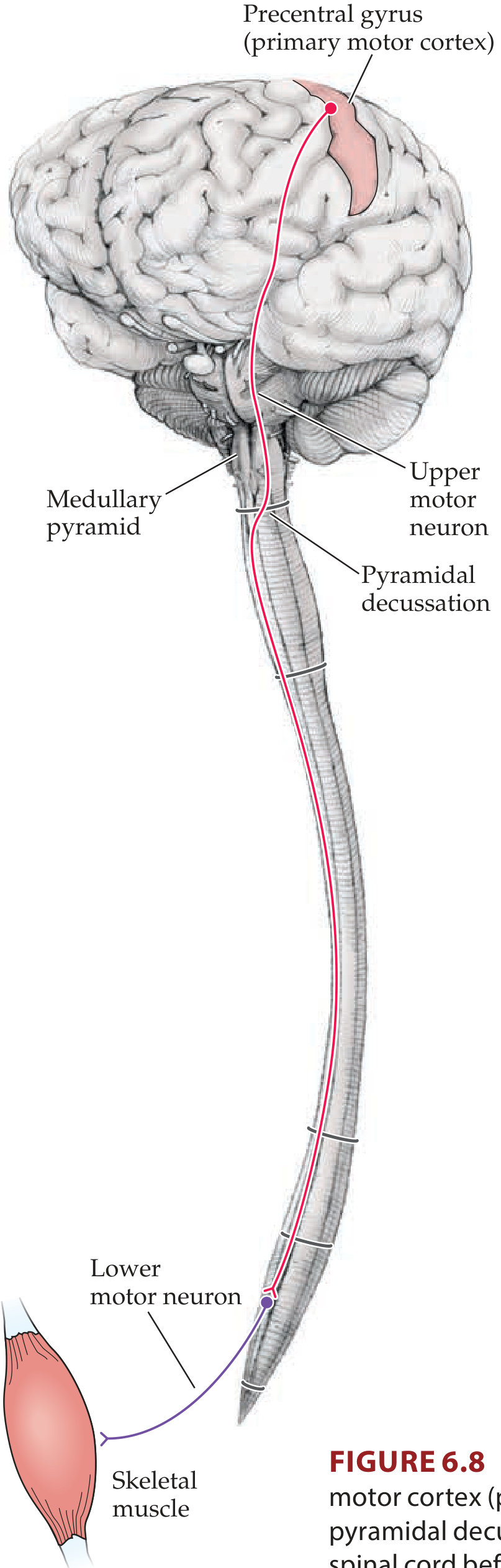
Corticospinal Tract
The corticospinal tract (CST) — also called the pyramidal tract — is the most clinically important descending motor pathway in the nervous system. It controls voluntary movement of the extremities and is the pathway whose lesions produce the classic UMN syndrome.
1. Origin
Fibres arise from multiple cortical areas:
| Area | Contribution |
|---|---|
| Primary motor cortex — Brodmann area 4 (precentral gyrus) | ~30% |
| Premotor + supplementary motor cortex — Brodmann area 6 | ~30% |
| Somatosensory cortex — Brodmann areas 3, 1, 2, 5, 7 (postcentral gyrus + parietal lobe) | ~40% |
Neurons contributing to the CST are found mainly in cortical layer V. About 3% are giant Betz cells (~60 µm diameter), found only in the primary motor cortex — these are the largest neurons in the human nervous system. Their fibres conduct at ~70 m/sec. Each tract contains >1 million fibres total.
2. Course — Level by Level
Cerebral Cortex → Internal Capsule
- Axons enter the corona radiata (fan-shaped white matter)
- Converge into the posterior limb of the internal capsule (between caudate nucleus and putamen)
Internal Capsule → Brainstem
- Pass through the basis pedunculi (crus cerebri) of the midbrain
- Scatter into the longitudinal fascicles of the pons (broken up by pontine nuclei)
- Reconverge at the medulla to form the pyramids of the medulla oblongata (giving the tract its alternative name — pyramidal tract)
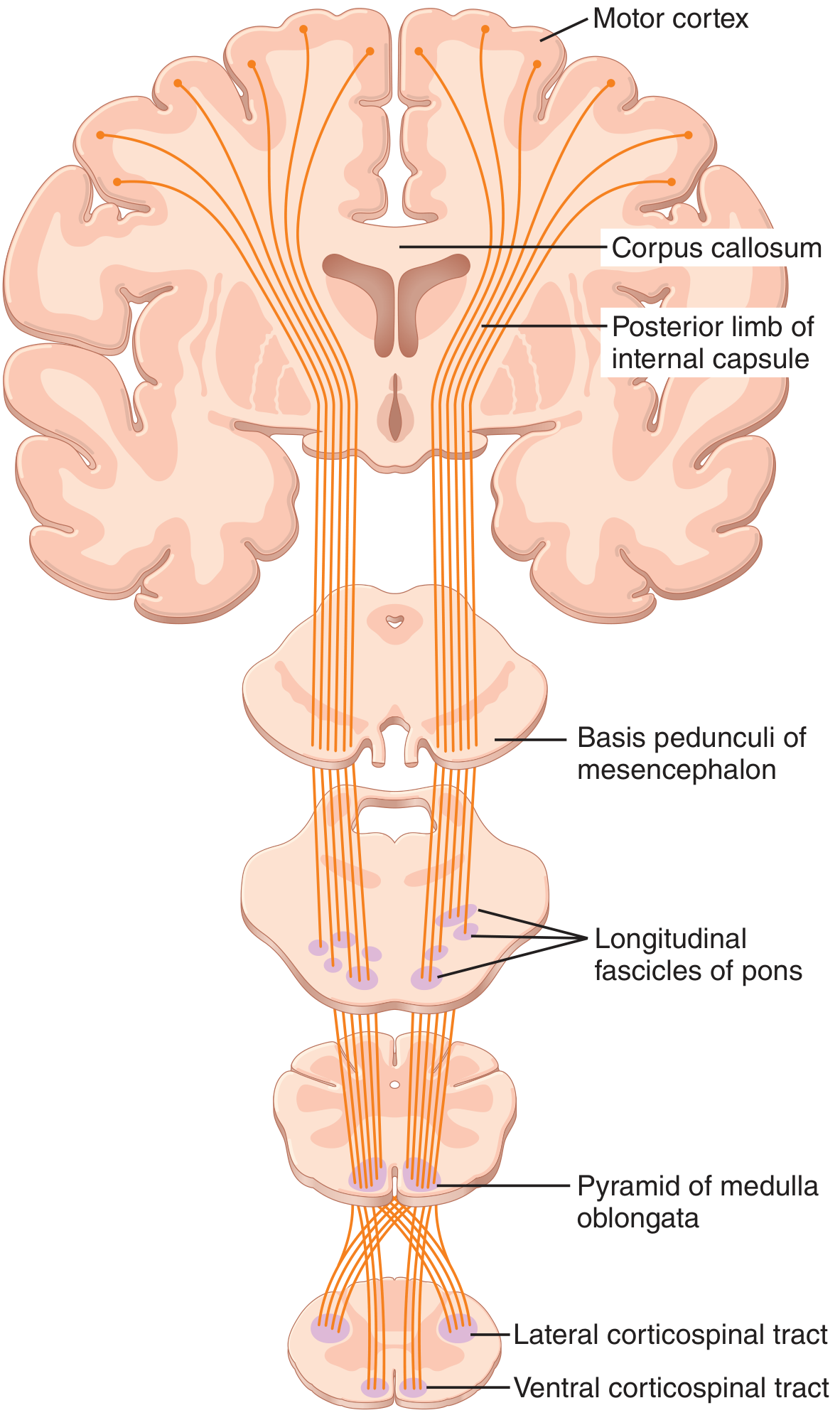
Pyramidal Decussation (caudal medulla)
- ~85–90% of fibres cross to the contralateral side in an interdigitated manner → descend as the lateral corticospinal tract in the lateral funiculus of the spinal cord
- ~10–15% do not cross → descend ipsilaterally as the anterior (ventral) corticospinal tract in the ventral funiculus; most of these eventually cross at their segmental level via the ventral white commissure (in cervical and upper thoracic segments)
3. Termination in the Spinal Cord
| Division | Location in cord | Termination | Function |
|---|---|---|---|
| Lateral corticospinal tract | Lateral funiculus | Laminae IV–VII and IX; extends throughout all cord levels | Controls distal limb muscles — fine voluntary movement |
| Anterior corticospinal tract | Ventral funiculus | Lamina III, cervical + upper thoracic only (after crossing) | Controls axial/bilateral postural muscles |
- Most fibres synapse on spinal interneurons in the intermediate zone
- Some synapse on sensory relay neurons in the dorsal horn
- A very few synapse directly on anterior motor neurons (alpha motor neurons) — these direct monosynaptic connections are especially important for fine finger movements
4. Somatotopic Organization
The CST maintains somatotopy throughout:
- In the motor cortex: face → hand → arm → trunk → leg (lateral to medial), with disproportionately large representation for hands and speech (Penfield homunculus)
- In the internal capsule: fibres in the posterior limb are arranged anterior (face) → posterior (leg)
- In the spinal cord lateral columns: cervical fibres are most medial; sacral fibres most lateral
5. UMN vs. LMN Lesions
| Feature | UMN Lesion (CST damage) | LMN Lesion |
|---|---|---|
| Weakness | Yes | Yes |
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Reflexes | Hyperreflexia | Hyporeflexia / areflexia |
| Babinski sign | Present | Absent |
| Atrophy | Mild (disuse) | Severe + early |
| Fasciculations | Absent | Present |
Note: In acute UMN lesions (e.g., stroke, spinal shock), flaccid paralysis and hyporeflexia may initially occur — spasticity develops over hours to months. Spasticity is thought to arise not from CST damage itself, but from concurrent damage to descending inhibitory pathways that run alongside the CST.
6. Clinical Correlate
A lesion above the pyramidal decussation (e.g., internal capsule stroke) → contralateral hemiplegia/hemiparesis with UMN signs.
A lesion below the decussation (e.g., lateral spinal cord) → ipsilateral UMN weakness below the lesion level.
The classic example: a 74-year-old woman waking with sudden right-sided face, arm, and leg paralysis with brisk reflexes and a Babinski sign on the right — pointing to a left-sided lesion above the pyramidal decussation (e.g., left internal capsule or motor cortex).
— Neuroanatomy through Clinical Cases, 3rd Ed. | Localization in Clinical Neurology, 8e | Guyton & Hall Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.