Positioning for craniotomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have comprehensive material to write a detailed, well-sourced answer on positioning for craniotomy. Let me compile it.
Positioning for Craniotomy
Proper positioning is one of the most important preparatory steps for any craniotomy. The goals are to optimize surgical access to the target region, reduce intracranial pressure (ICP), maintain adequate cerebral perfusion, and prevent position-related complications.
General Principles
- Head fixation: The head is rigidly fixed in a three-point pin (Mayfield) skull clamp to prevent any movement during surgery.
- Head elevation: The head is kept 15-30° above the level of the heart to promote venous drainage and reduce ICP. Elevating the head to 30° increases venous drainage and lowers ICP. The head must be in the midline to prevent obstruction of jugular venous return from the brain. - Miller's Anesthesia, 10e
- Neck position: Avoid excessive flexion or rotation - either obstructs jugular venous drainage and raises ICP, or risks cervical cord injury.
- Padding: All pressure points (elbows, ischial spines, heels, bony prominences) must be carefully padded.
Specific Positions by Approach
1. Supine
- Used for: frontal, temporal, and pterional (frontotemporal) craniotomies.
- The head may be turned to one side and secured in the Mayfield clamp.
- Indications: anterior circulation aneurysms, suprasellar tumors, cavernous sinus lesions, frontal lobe tumors, and most intracranial hematomas.
- The pterional approach (access to the pterion, where frontal, parietal, temporal, and sphenoid bones meet) is one of the most common. - Neuroanatomy through Clinical Cases, 3e
2. Lateral (Park Bench / Semi-lateral)
- Used for: temporal and parieto-occipital lesions; also an alternative for posterior fossa surgery.
- Patient on their side; the head is secured in a three-point holder with neutral neck position.
- Avoids the risks of the sitting position (see below), so is often preferred for posterior fossa over prone or sitting.
3. Prone
- Used for: suboccipital/posterior fossa craniotomies, midline occipital and cerebellar lesions.
- Patient is prone with the head fixed in a pin holder, neck slightly flexed.
- Risks include pressure injury to the face/eyes, venous engorgement, and abdominal compression impairing ventilation.
4. Sitting (Semi-recumbent)
- Used for: posterior fossa and pineal region surgery, by surgeons who prefer it for access and visualization.
- The back is elevated to 60°, legs are raised with knees flexed, head is fixed in a three-point holder with neck flexed, and arms rest in the lap. - Morgan & Mikhail's Clinical Anesthesiology, 7e
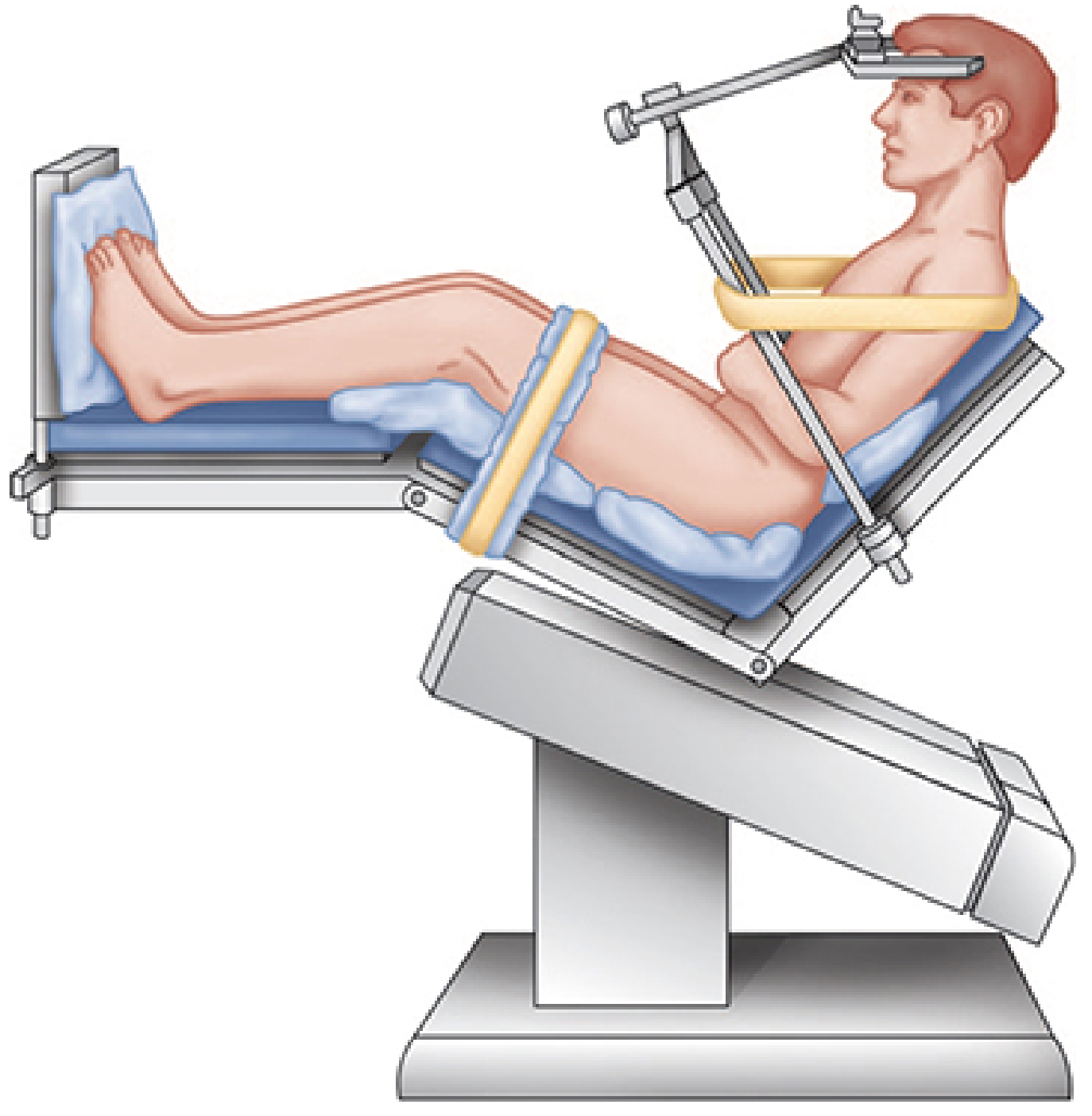
Although most posterior fossa explorations can be performed in either a modified lateral or prone position, the sitting position may be preferred by some surgeons. - Morgan & Mikhail's Clinical Anesthesiology, 7e
Complications of the Sitting Position
The sitting position carries the highest risk and requires the most anesthetic vigilance:
Venous Air Embolism (VAE)
- The most feared complication. Occurs when venous pressure in an open vein is subatmospheric (wound above heart level).
- Incidence is 20-40% with sitting craniotomies - far higher than any other position.
- Entry into large cerebral venous sinuses increases risk.
- Paradoxical air embolism can occur through a patent foramen ovale (PFO, present in 10-25% of people), causing stroke or coronary occlusion.
- N₂O markedly worsens VAE by diffusing into bubbles and expanding them (reduces lethal volume to one-third to one-half). Nitrous oxide is therefore rarely used for sitting craniotomies.
Detection:
| Monitor | Sensitivity |
|---|---|
| Transesophageal echocardiography (TEE) | Highest - detects bubbles ≥0.25 mL; also detects PFO |
| Precordial Doppler | High - also detects ≥0.25 mL |
| End-tidal CO₂ | Moderate - sudden decrease due to increased dead space |
| "Mill wheel" murmur / BP drop | Late signs |
Treatment of VAE:
- Notify surgeon immediately - flood field with saline, pack with wet gauze, apply bone wax to skull edges
- Discontinue N₂O; ventilate with 100% oxygen
- Aspirate entrained air via central venous catheter (multiorificed catheter at cavoatrial junction)
- Infuse IV fluids to raise central venous pressure
- Vasopressors for hypotension
- Bilateral jugular vein compression to slow air entrainment and help locate the entry site
- Consider turning patient left lateral decubitus (Durant's maneuver) if severe - Morgan & Mikhail's Clinical Anesthesiology, 7e
Central line positioning: For sitting craniotomies, a multiorificed catheter is placed at the right atrium-SVC junction. Correct position is confirmed by intravascular ECG (maximally biphasic P wave), radiography, or TEE.
Pneumocephalus
- Sitting position significantly increases risk; air enters subarachnoid space as CSF is lost during surgery.
- In cerebral atrophy, air can replace CSF across the brain surface and lateral ventricles.
- Tension pneumocephalus after dural closure can compress the brain and cause delayed awakening.
- This is another reason N₂O is avoided - it diffuses into pneumocephalus and expands it.
Postural Hypotension
- Venous pooling in the lower extremities can reduce cardiac output.
- The legs are elevated with knees flexed to mitigate this.
Excessive Neck Flexion
- Can cause: (1) upper airway swelling from venous obstruction, (2) quadriplegia from cervical cord compression - especially if pre-existing cervical stenosis is present. - Morgan & Mikhail's Clinical Anesthesiology, 7e
Summary Table
| Position | Approach | Common Use | Key Risks |
|---|---|---|---|
| Supine (head turned) | Pterional, frontal, temporal | Aneurysms, suprasellar tumors, hematomas | ICP if neck rotated |
| Lateral | Temporal, parieto-occipital, posterior fossa | Same as above, CPA tumors | Pressure injuries |
| Prone | Suboccipital, posterior fossa, occipital | Cerebellar, brainstem, posterior midline | Eye/face pressure, venous engorgement |
| Sitting | Posterior fossa, pineal | Cerebellar, CPA, 4th ventricle | VAE (20-40%), pneumocephalus, hypotension, neck flexion injury |
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 27: Neuroanesthesia (Positioning, Venous Air Embolism sections)
- Neuroanatomy through Clinical Cases, 3e - Section 5.11: Craniotomy
- Miller's Anesthesia, 10e - Head positioning and ICP management
This is a shared conversation. Sign in to Orris to start your own chat.