L5s1 compression disc protrusion effect on fertility with 1 month pain pelvic numbness and feet immobility
lumbar disc herniation L5S1 fertility sexual dysfunction
L5 S1 disc herniation effect on fertility pelvic numbness cauda equina
cauda equina syndrome sexual dysfunction fertility
cauda equina syndrome sexual dysfunction outcome recovery
L5–S1 Disc Protrusion: Neurological Effects, Pelvic/Fertility Impact, and Your Symptoms
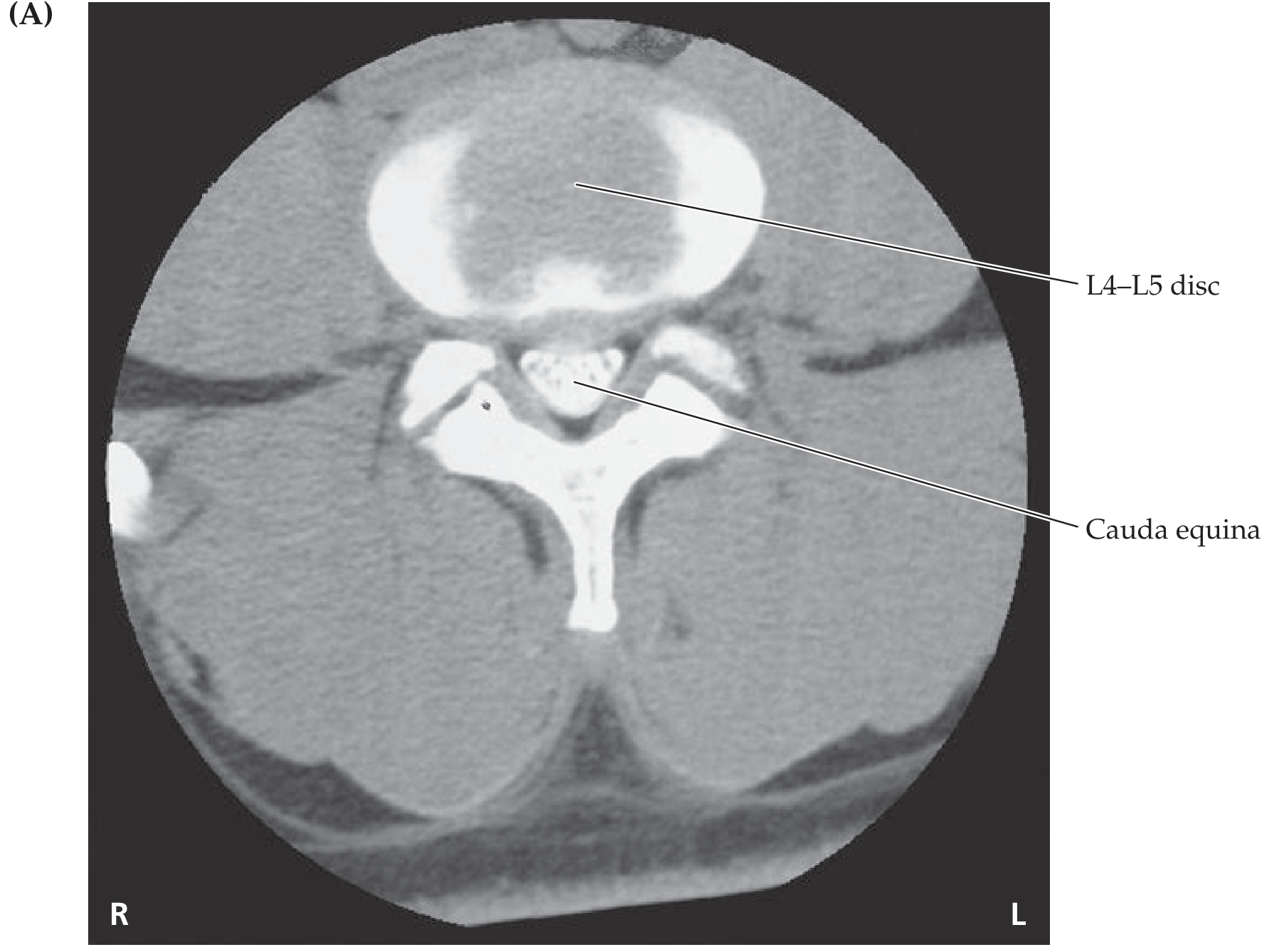
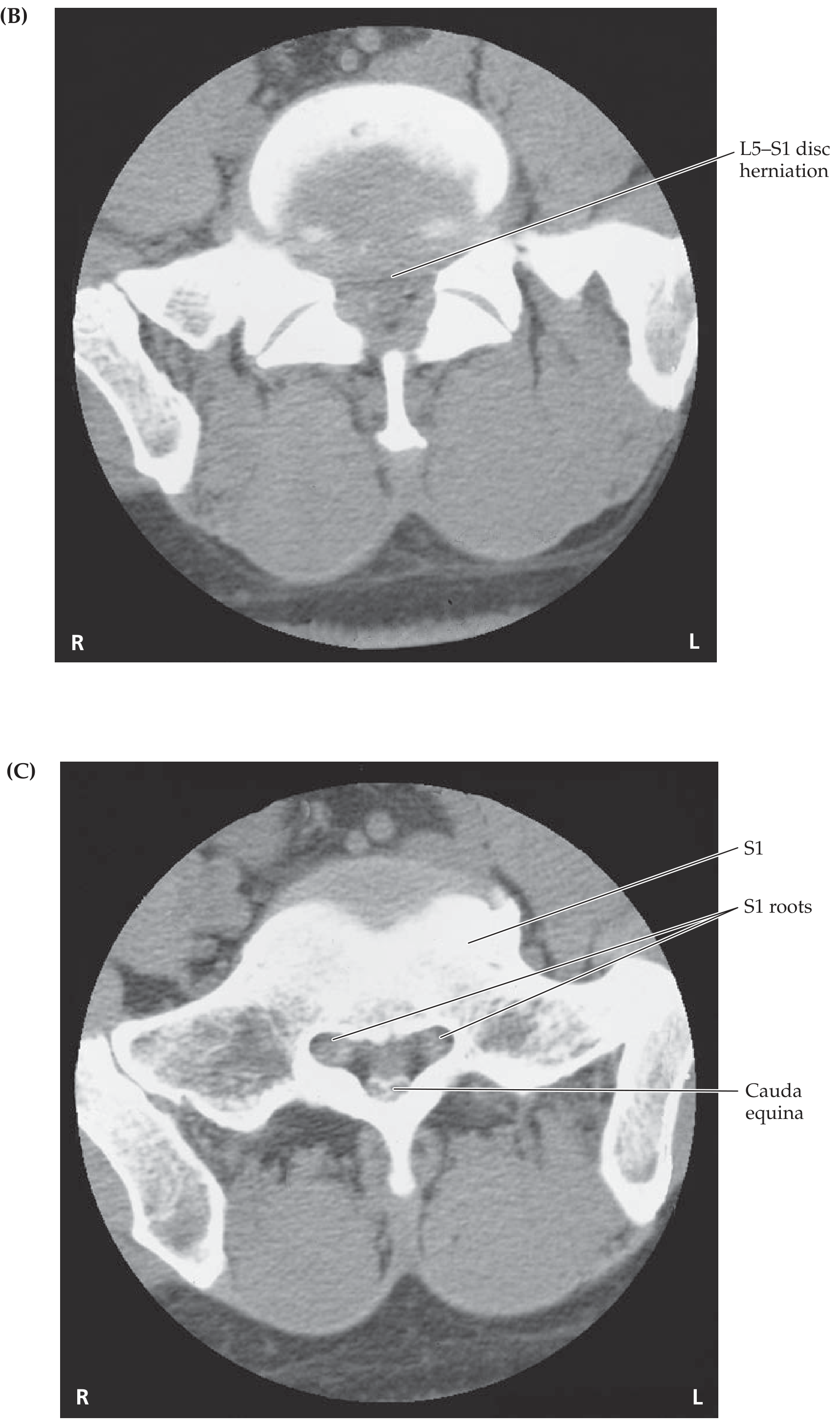
1. What Happens Anatomically at L5–S1
2. Interpreting Your Symptom Combination
A. S1 Radiculopathy (single root compression)
- Pain radiating down the posterior leg to the heel/lateral foot
- Sensory loss on the lateral foot and sole
- Weakness of plantarflexion (standing on tiptoe)
- Reduced or absent ankle jerk reflex
- This alone does not typically cause pelvic numbness or significant pelvic organ dysfunction
B. Cauda Equina Syndrome (CES) — the concern here
- Bladder dysfunction (~90% of cases) — initially sensory, then painless retention, then overflow incontinence
- Bowel dysfunction (~50%)
- Sexual dysfunction — erectile/ejaculatory dysfunction in males; genital arousal and lubrication dysfunction in females
- Saddle anaesthesia — numbness of the perineum, inner thighs, genitals (~80%)
- Bilateral leg weakness (radiculopathy)
3. Does L5–S1 Disc Compression Affect Fertility?
Direct neurological effect on fertility:
- The uterus, cervix, vagina, and ovaries (in females)
- The testes, vas deferens, prostate, and seminal vesicles (in males)
- The bladder, rectum, and perineal muscles
| Effect | Mechanism |
|---|---|
| Erectile dysfunction (males) | Loss of parasympathetic (S2–S4) innervation to corpora cavernosa |
| Ejaculatory dysfunction (males) | Disruption of sympathetic/somatic pathways |
| Vaginal dryness / arousal failure (females) | Loss of parasympathetic genital innervation |
| Reduced orgasmic sensation | Sensory loss in pudendal nerve territory (S2–S4) |
| Pelvic floor weakness | Motor loss affecting levator ani and perineal muscles |
Does it affect the ability to conceive?
- In females: Neurological compression does not directly impair ovulation, egg quality, or tubal function — fertility in the biological sense (reproductive organ function) is governed by hormones, not by the L5–S1 nerve roots. However, if sexual intercourse becomes painful or impossible due to pelvic numbness and muscle dysfunction, functional infertility may result. Uterine contractility during labor could also be impaired in severe CES.
- In males: Significant cauda equina compression can cause anejaculation or retrograde ejaculation, directly impairing the ability to deliver sperm naturally — a genuine fertility concern.
Key distinction: The L5–S1 disc does not affect hormones (FSH, LH, estrogen, testosterone) or gonadal function. Its impact on fertility is neurogenic — through pelvic organ innervation — not endocrine.
4. The Urgency of Your Situation
"The syndrome can result in permanent motor deficit and bladder, bowel and sexual dysfunction. It represents a true spinal emergency and requires urgent surgical decompression. The outcome for patients who undergo surgical decompression within 24 hours of the onset of loss of bladder or bowel control is significantly better than those who undergo surgery beyond this 24-hour period."
| Stage | Definition | Action |
|---|---|---|
| CES-E (Early) | Perineal sensory change, normal bladder/bowel | Urgent decompression |
| CES-I (Incomplete) | Impaired bladder sensation, voluntary control maintained | Urgent decompression |
| CES-R (Retention) | Bladder retention + overflow incontinence | Emergency surgery |
| CES-C (Complete) | Complete loss of cauda equina function | Surgery if recovery possible |
5. What You Need Right Now
- Urgent MRI of the lumbosacral spine — this is the gold-standard investigation to confirm disc compression of the cauda equina
- Neurological assessment — sensory mapping of saddle area, bladder post-void residual, anal tone
- Neurosurgical/spinal surgery consultation — for decision on microdiscectomy or laminectomy
- Urodynamic studies — if bladder dysfunction is present
6. Prognosis
- Sexual dysfunction after CES is common and persistent, particularly in cases with delayed decompression
- Micturition and sexual function show the worst recovery rates compared to motor deficits
- Early surgery (within 48 hours of symptom onset) gives the best chance of recovery; after 1 month, outcomes are less predictable but surgery can still halt progression
Find recent surgical guidelines for cauda equina syndrome decompression in 1st 2 weeks
cauda equina syndrome surgical decompression timing guidelines
cauda equina syndrome decompression 24 hours 48 hours outcome
cauda equina syndrome surgical guidelines 2023 2024 decompression timing within 2 weeks
PMID: 41991105
PMID: 39937930
PMID: 34581849
PMID: 38835174
cauda equina syndrome late presentation delayed surgery 2 weeks outcome
NICE guideline cauda equina syndrome 2024 surgical timing decompression recommendation
Actually ces is ruled out only one legs was involved and saddle numbness was for first two weeks only and then the ejection and ejacculation were perfect
L5 S1 radiculopathy pelvic pain referred unilateral
lumbar radiculopathy pelvic pain numbness fertility impact
Revised Assessment: Unilateral L5–S1 Radiculopathy (Not CES)
Why CES Is Ruled Out
- Only one leg affected ✓ (CES typically bilateral)
- Saddle numbness was transient — only first 2 weeks, then resolved ✓
- Erection and ejaculation are intact ✓ — this is the most important confirmation. CES causes neurogenic sexual dysfunction that doesn't resolve on its own; normal sexual function means the S2–S4 parasympathetic and pudendal motor pathways are working correctly
Your Actual Diagnosis: Unilateral S1 Radiculopathy
"A posterolateral protrusion at L5–S1 causes symptoms referable predominantly to an S1 distribution... whereas a very lateral disc protrusion at L5–S1 affects the L5 root."
Classic S1 Root Signs (unilateral):
| Feature | S1 Involvement |
|---|---|
| Pain | Posterior thigh → calf → heel / lateral foot |
| Sensory loss | Lateral foot, sole, little toe |
| Motor weakness | Plantarflexion (standing on tiptoe) — foot "immobility"/heaviness |
| Reflex loss | Ankle jerk absent or reduced |
| Pelvic pain | Referred pain into the buttock and posterior pelvis (S1 dermatome) |
Effect on Fertility: The Revised Answer
Negligible to none.
| Concern | Verdict |
|---|---|
| Sperm production | Unaffected — testicular function is governed by the hypothalamic-pituitary axis (hormones), not L5–S1 |
| Erection | Normal — confirms intact S2–S4 parasympathetics |
| Ejaculation | Normal — confirms intact sympathetic chain (L1–L2) and pudendal nerve (S2–S4) |
| Sperm delivery | Unaffected |
| Female reproductive organs | Unaffected — uterus, ovaries, tubal function are hormonally driven |
| Intercourse | May be limited by pain during acute phase — a functional/mechanical issue, not a neurological fertility impairment |
The only fertility-relevant concern in your case is if persistent leg pain or pelvic pain makes sexual intercourse uncomfortable or less frequent — a pain-management problem, not a reproductive biology problem.
What the Remaining Symptoms Indicate
- Motor weakness (foot/ankle) at 1 month indicates the nerve root is still under pressure
- Without decompression, prolonged motor deficit can lead to partial permanent weakness
- The window for best motor recovery from surgery is within 3 days for severe deficits (MRC ≤3/5), within a few weeks for mild paresis (Kögl et al., Dtsch Arztebl Int 2024, PMID 38835174)
"Longer symptom duration and lower motor scores are associated with worse outcome and a lower chance of neurologic recovery. The recovery rate for motor deficits ranges from 33% to 75%, depending on timing and modality of treatment."
What You Need
- MRI lumbosacral spine (if not already done) — confirm level and degree of S1 compression
- Neurological exam — ankle reflex, plantarflexion strength grading (MRC scale)
- Physiotherapy — for 60–80% of uncomplicated radiculopathy cases, symptoms resolve in 6–12 weeks conservatively
- Surgical consultation — if foot motor deficit is significant (MRC ≤ 3/5) or failing to improve after 6 weeks, microdiscectomy is indicated to prevent permanent weakness
- No specific fertility workup needed — your reproductive function is neurologically intact based on your symptoms