Arrhythmia
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"cardiac arrhythmia"[MeSH Terms] AND "review"[pt]
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive textbook content. Let me compile the full overview.
Cardiac Arrhythmia - Comprehensive Overview
Sources: Braunwald's Heart Disease, Washington Manual of Medical Therapeutics, Miller's Anesthesia
1. Definition
An arrhythmia is any disturbance of the normal cardiac rate, rhythm, or conduction. The term encompasses bradycardias (rate <60 bpm), tachycardias (rate >100 bpm), and abnormalities of conduction (heart blocks). The normal sinus rhythm originates in the sinoatrial (SA) node and propagates through the AV node, His bundle, and Purkinje fibers.
2. Mechanisms of Arrhythmia
All arrhythmias arise through one or more of three fundamental electrophysiologic mechanisms:
A. Abnormal Automaticity
- Normal enhanced automaticity: Increased phase-4 depolarization rate of pacemaker cells beyond normal (e.g., inappropriate sinus tachycardia). Treated with beta-blockers or I₁ (funny current) blockers like ivabradine.
- Abnormal automaticity: Non-pacemaker cells (atrial, ventricular) develop spontaneous depolarization, seen in ischemia, metabolic disturbances, or digoxin toxicity (e.g., ectopic atrial tachycardia).
B. Triggered Activity
- Early afterdepolarizations (EADs): Occur during phases 2-3 of the action potential, associated with prolonged QT (hypokalaemia, drug effects). Mechanism of Torsades de Pointes (TdP).
- Delayed afterdepolarizations (DADs): Occur during phase 4, driven by calcium overload. Seen in digitalis toxicity, catecholaminergic states.
C. Re-entry
The most common arrhythmia mechanism. Requires:
- Two anatomically or functionally distinct pathways
- Unidirectional block in one pathway
- Sufficient conduction slowing in the other to allow recovery of the blocked pathway
Examples: AVNRT, AVRT (WPW), atrial flutter, ventricular tachycardia in scar tissue.
3. Classification
Bradyarrhythmias (Rate <60 bpm)
| Arrhythmia | Key Feature | Common Cause |
|---|---|---|
| Sinus bradycardia | Rate <60, normal P-QRS | Vagal tone, beta-blockers, inferior MI, hypothyroidism |
| Sick sinus syndrome | Sinus pauses, SA exit block, tachycardia-bradycardia | SA nodal degeneration, post-cardiac surgery |
| 1st degree AV block | PR >200 ms, all P waves conduct | Vagal tone, medications |
| 2nd degree - Mobitz I (Wenckebach) | Progressive PR lengthening → dropped beat | AV node disease; usually benign |
| 2nd degree - Mobitz II | Fixed PR, sudden dropped beat | His-Purkinje disease; risk of progression to complete block |
| 3rd degree (complete) AV block | P waves and QRS dissociated | Ischemia, fibrosis, medications; urgent pacing needed |
Tachyarrhythmias - Supraventricular (SVT, QRS <120 ms)
Tachycardias requiring atrial or AV nodal tissue for initiation/maintenance. Prevalence of paroxysmal SVT is ~2.25/1000, with women affected twice as often as men.
| Arrhythmia | ECG Feature | Mechanism |
|---|---|---|
| Sinus tachycardia | Rate 100-180, normal P-QRS | Physiologic (fever, pain, hypovolemia, anemia) |
| Inappropriate sinus tachycardia | Persistent elevated rate at rest >100 | Enhanced SA node automaticity |
| AVNRT | "Absent P waves" - P buried in QRS; pseudo-r' in V1 | Re-entry in dual AV nodal pathways (short RP) |
| AVRT (WPW) | Delta wave, short PR in sinus; may see narrow or wide tachycardia | Accessory pathway re-entry |
| Atrial fibrillation | Absent P waves, irregularly irregular, fibrillatory baseline (V1, II, III, aVF) | Ectopic foci in pulmonary veins + multiple reentrant circuits |
| Atrial flutter | Sawtooth pattern leads II, III, aVF; atrial rate 250-350 bpm, usually 2:1 conduction (ventricular rate ~150) | Macroreentrant circuit around tricuspid annulus (typical) |
| MAT | Irregularly irregular; ≥3 distinct P-wave morphologies | Enhanced automaticity; associated with COPD, CHF |
| EAT | Long RP tachycardia, abnormal P-wave axis | Automaticity, triggered activity, micro-reentry |
| Junctional tachycardia | P retrograde or absent; uncommon in adults | Automaticity; common post-cardiac surgery in children |
Tachyarrhythmias - Ventricular (QRS ≥120 ms unless aberrant conduction)
| Arrhythmia | ECG Feature | Notes |
|---|---|---|
| PVCs | Wide QRS, no preceding P; compensatory pause | Common; benign unless frequent/in structural disease |
| Ventricular tachycardia (VT) | Wide regular QRS tachycardia, AV dissociation, fusion/capture beats | Re-entry around scar; hemodynamically unstable VT = immediate cardioversion |
| Torsades de Pointes | Polymorphic VT, twisting QRS axis around baseline | Long QT (drug-induced, electrolyte, congenital); treat with IV magnesium |
| Ventricular fibrillation | Chaotic, no organized QRS | Cardiac arrest; immediate defibrillation required |
4. ECG-Based Diagnostic Approach
The diagram below (from Washington Manual) provides a systematic algorithm:
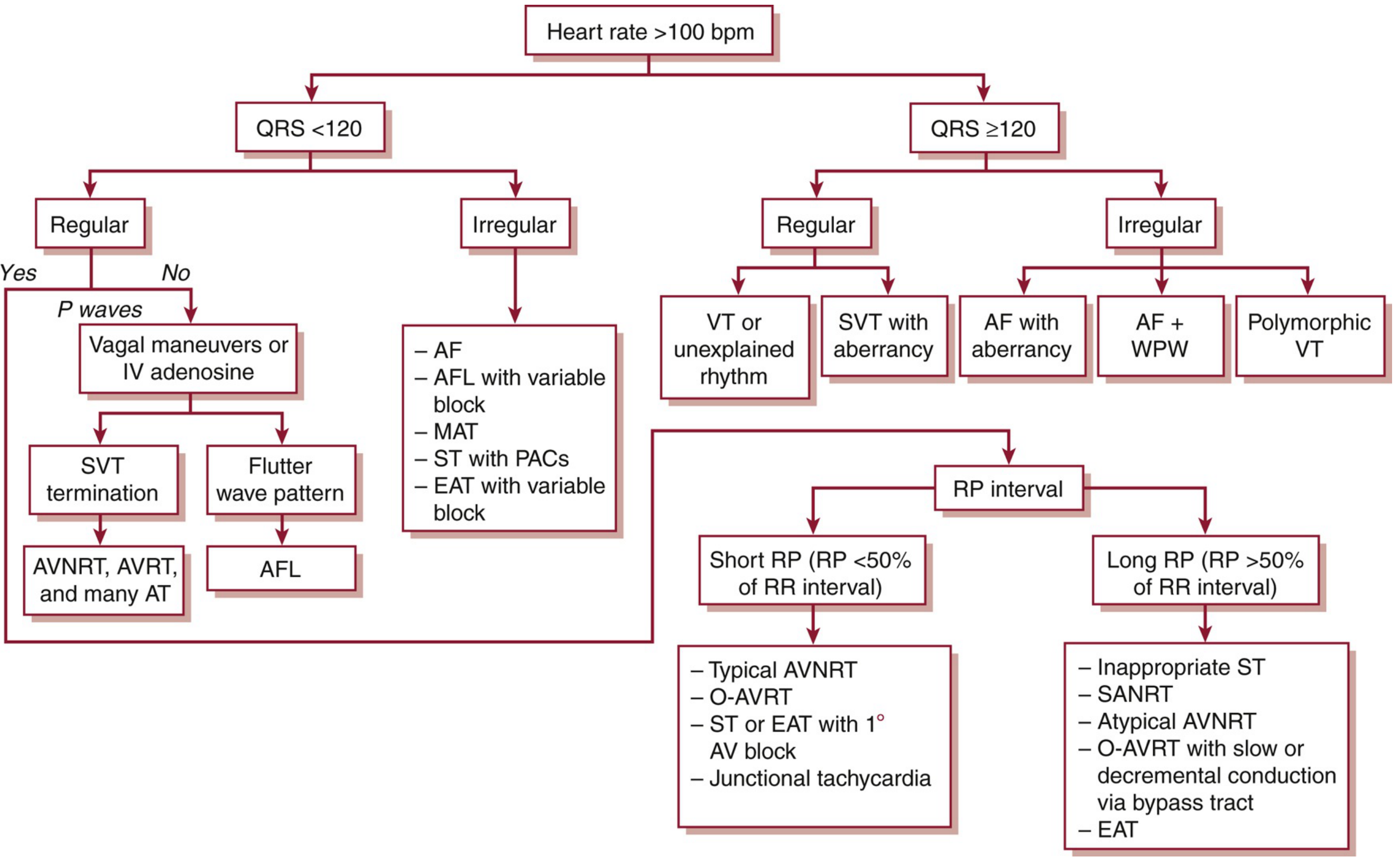
Step-by-step logic:
- Is the rate >100? → Tachyarrhythmia
- Is QRS narrow (<120 ms) or wide (≥120 ms)?
- Is the rhythm regular or irregular?
- Are P waves present? What is the RP relationship?
- Short RP (<50% of RR): Typical AVNRT, orthodromic AVRT, junctional tachycardia
- Long RP (>50% of RR): Sinus tachycardia, atypical AVNRT, EAT, SANRT
- Wide-complex regular: VT vs. SVT with aberrancy (VT is more common and should be assumed until proven otherwise)
5. Common Arrhythmias In Depth
Atrial Fibrillation (AF)
The most common sustained tachyarrhythmia. Affects >10% of those aged >75 years.
Classification (5 forms):
- First occurrence
- Paroxysmal (<7 days, usually <48 hrs)
- Persistent (>7 days)
- Long-standing persistent (>1 year, amenable to cardioversion)
- Permanent (accepted; cardioversion not pursued)
Risk factors: Advanced age, male sex, HTN, CHF, DM, valvular disease, previous MI, obesity, OSA. Post-cardiothoracic surgery AF occurs in 20-50% of patients.
Pathophysiology: Initiated by rapid ectopic firing from pulmonary vein foci; maintained by multiple reentrant circuits. Structural and electrical remodeling (fibrosis, inflammation) perpetuates the arrhythmia. CRP and IL-6 are elevated and correlate with duration.
Management principles:
- Rate control: beta-blockers, non-dihydropyridine CCBs, digoxin
- Rhythm control: cardioversion (electrical or pharmacologic) + antiarrhythmics (amiodarone, flecainide, propafenone, sotalol)
- Anticoagulation: CHA₂DS₂-VASc score guides DOAC or warfarin use for stroke prevention
- Ablation: pulmonary vein isolation for symptomatic drug-refractory AF
Sinus Bradycardia
Benign in most cases (athletes, vagal tone, sleep). Treat only if symptomatic or hemodynamically unstable. Acute: atropine 0.5 mg IV. Chronic: pacing.
AV Blocks
- Mobitz I: usually AV nodal; benign; may resolve with atropine
- Mobitz II: His-Purkinje; high risk of complete block; requires pacemaker
- Complete AV block: pacing is definitive therapy
6. Antiarrhythmic Drug Classes (Vaughan Williams)
| Class | Mechanism | Key Drugs | Use |
|---|---|---|---|
| IA | Na⁺ channel block (moderate, ↑APD) | Quinidine, procainamide, disopyramide | AF, VT |
| IB | Na⁺ channel block (fast on-off, ↓APD) | Lidocaine, mexiletine | Ventricular arrhythmias |
| IC | Na⁺ channel block (slow on-off, no APD change) | Flecainide, propafenone | SVT, AF (no structural disease) |
| ID | Late Na⁺ current block | Ranolazine | Reduces EAD-triggered activity |
| II | Beta-adrenergic blockade | Metoprolol, carvedilol, propranolol | Rate control, post-MI, VT |
| III | K⁺ channel block (↑APD, ↑refractoriness) | Amiodarone, sotalol, dronedarone, ibutilide | AF, VT/VF |
| IV | L-type Ca²⁺ channel block | Verapamil, diltiazem | Rate control (SVT, AF) |
- Braunwald's Heart Disease, Ch. 64
7. Acute Management Summary
| Presentation | Immediate Action |
|---|---|
| Hemodynamically unstable tachyarrhythmia (any type) | Synchronized cardioversion (or defibrillation for VF/pVT) |
| VF / pulseless VT | Immediate defibrillation + ACLS |
| Stable narrow-complex regular SVT | Vagal maneuvers → IV adenosine |
| Stable AF with rapid ventricular response | Rate control (IV beta-blocker or CCB) |
| TdP | IV magnesium sulfate, correct electrolytes, remove offending drugs |
| Symptomatic bradycardia | IV atropine → temporary pacing |
8. Chronic / Invasive Options
- Catheter ablation: Curative for most SVTs (AVNRT ~96%, AVRT ~95%, typical AFL ~90%). Also increasingly used for AF (pulmonary vein isolation) and scar-related VT.
- Implantable cardioverter-defibrillator (ICD): Primary/secondary prevention of sudden cardiac death in patients with VT/VF or high risk (EF <35%).
- Permanent pacemaker: Sick sinus syndrome, high-degree AV block, symptomatic bradycardia.
Sources: Braunwald's Heart Disease (2 Vol Set), Washington Manual of Medical Therapeutics, Miller's Anesthesia 10e, Fuster and Hurst's The Heart 15e.
How to differentiate ventricular tachy and ventricular fibrillation
Finding Sources
Searching PubMed
"ventricular tachycardia"[MeSH Terms] AND "ventricular fibrillation"[MeSH Terms] AND diagnosis
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have all the content needed for a thorough, well-illustrated answer. Let me compile it.
Differentiating Ventricular Tachycardia (VT) vs. Ventricular Fibrillation (VF)
Sources: Braunwald's Heart Disease, Fuster and Hurst's The Heart 15e, Rosen's Emergency Medicine
The Core Distinction at a Glance
| Feature | Ventricular Tachycardia (VT) | Ventricular Fibrillation (VF) |
|---|---|---|
| QRS complexes | Present - wide, defined | Absent - no identifiable QRS |
| Rhythm | Regular (monomorphic) or semi-regular | Completely chaotic, irregular |
| Rate | 100-250 bpm, countable | Cannot be counted - indeterminate |
| Organization | Organized electrical activity | Totally disorganized |
| ECG appearance | Wide, repetitive QRS complexes | Rapid, irregular, dysmorphic squiggles |
| Cardiac output | May be present (can be hemodynamically stable) | None - immediate hemodynamic collapse |
| P waves | Often dissociated from QRS (AV dissociation) | Absent |
| Defibrillation | Synchronized cardioversion (if pulseless: defibrillation) | Unsynchronized defibrillation immediately |
1. Ventricular Tachycardia (VT)
ECG Characteristics
- Wide QRS (≥120 ms) at rate typically 100-250 bpm
- Regular rhythm (monomorphic VT) - complexes look the same beat to beat
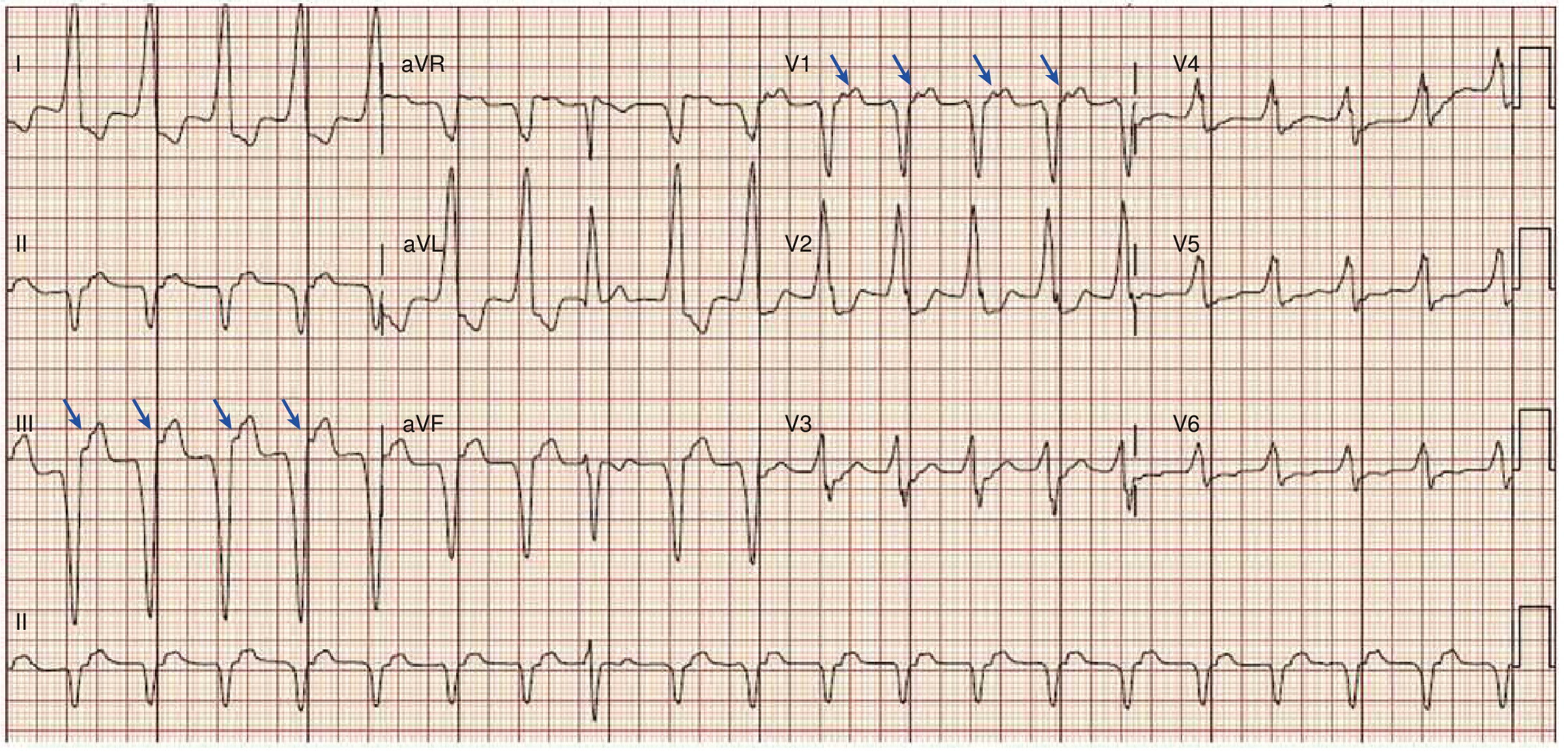
- AV dissociation - P waves march through at a slower rate, independent of the QRS complexes. This is the single most specific sign of VT. It may be subtle - look for small bumps distorting the QRS/ST-T waves.
- Fusion beats - a hybrid complex formed when a sinus impulse partially activates the ventricle simultaneously with the VT focus (pathognomonic of VT)
- Capture beats - a normal narrow QRS occurring during the tachycardia when a sinus impulse briefly "captures" the ventricle (also pathognomonic of VT)
The ECG below (from Braunwald's) shows VT with AV dissociation - arrows in leads III and V1 mark independent P waves marching through the wide-complex tachycardia:
Types of VT
- Monomorphic VT: QRS morphology is identical beat to beat - most common; usually from re-entry around a scar
- Polymorphic VT: QRS morphology constantly changes - seen in ischemia, long QT
- Torsades de Pointes (TdP): A specific polymorphic VT where the QRS axis appears to "twist" around the isoelectric baseline. Associated with prolonged QT interval. Often self-terminating but can degenerate to VF.
Clinical Features
Patients may present with palpitations, dyspnea, chest pain, or be completely asymptomatic. Rapid VT (>200 bpm) usually causes hypotension and may present as syncope or cardiac arrest. Hemodynamic stability during VT does NOT exclude VT - do not be falsely reassured by a conscious patient with a pulse.
2. Ventricular Fibrillation (VF)
ECG Characteristics
- No identifiable QRS complexes - this is the defining feature
- Rapid, completely irregular, chaotic, dysmorphic deflections
- No organized waveforms - no P, QRS, or T waves
- Varying amplitude - subdivided into:
- Coarse VF: higher amplitude waves (>0.2 mV) - more responsive to defibrillation, more likely to be recent
- Fine VF: low amplitude, nearly flat - longer duration, harder to defibrillate; can be mistaken for asystole
- Mechanism: multiple simultaneously active functional reentrant wavelets traveling through the ventricles in non-stationary, rotating "spiral wave" patterns - the 3D complexity of ventricular geometry produces the chaotic ECG appearance
3. Key Differentiating ECG Signs in Detail
AV Dissociation (VT-specific)
The atria continue to fire from the sinus node while the ventricles fire independently at a faster rate. On ECG, P waves are visible at a slower, unrelated rate "walking through" the QRS complexes. This is the strongest ECG criterion for VT.
Fusion and Capture Beats (VT-specific, pathognomonic)
- Fusion beat: Sinus impulse + VT complex activate the ventricles simultaneously → the QRS is intermediate in morphology between normal sinus QRS and VT QRS
- Capture beat: Rare moment where a sinus impulse fully activates the ventricle during VT → produces a normal, narrow QRS amid wide complexes
QRS Morphology (VT vs. SVT with aberrancy)
When VT needs to be distinguished from SVT conducted with bundle branch block (both are wide-complex):
| Criterion | Favors VT |
|---|---|
| QRS width >160 ms | Yes |
| Extreme axis deviation ("northwest axis" - negative in I AND aVF) | Yes |
| Concordance in precordial leads (all QRS pointing same direction V1-V6) | Yes |
| No RS complex in any precordial lead | Yes |
| RS interval >100 ms in any V lead | Yes |
| Morphology doesn't fit typical LBBB or RBBB pattern | Yes |
| History of structural heart disease | Strongly favors VT |
4. The Polymorphic VT - VF Spectrum
This is the one area where the distinction can be genuinely difficult:
| Polymorphic VT | VF | |
|---|---|---|
| QRS complexes | Present, but constantly changing morphology | Absent - no defined QRS |
| Identifiability | Can identify individual complexes, count rate | Cannot identify individual complexes |
| Torsades de Pointes | A subtype of PMVT with twisting axis around baseline | - |
| Transition | PMVT can degenerate into VF | - |
As Fuster and Hurst's The Heart states: "Polymorphic VT, unlike VF, has clearly defined QRS complexes, but they are constantly changing with no clear pattern."
5. Clinical / Hemodynamic Differentiation
Both VT and VF can produce cardiac arrest, but:
| VT | VF | |
|---|---|---|
| Pulse | May be present (hemodynamically stable VT) or absent (pulseless VT) | Always pulseless |
| Blood pressure | Variable - may be maintained | Absent |
| Consciousness | May be preserved in slow VT | Always lost |
| Spontaneous termination | Possible (especially non-sustained VT <30s) | Does not self-terminate |
6. Emergency Management Based on the Distinction
WIDE COMPLEX TACHYCARDIA / NO PULSE
↓
Is there any organized QRS rhythm?
↙ ↘
YES NO
VT VF
↓ ↓
Pulseless VT Immediate unsynchronized
Treat same as VF defibrillation (200J biphasic)
+ CPR immediately after shock
- Stable VT (pulse present): Synchronized cardioversion OR antiarrhythmics (amiodarone 150 mg IV over 10 min, then infusion; or lidocaine)
- Pulseless VT / VF: Immediate unsynchronized defibrillation. Every minute of delay = 7-10% decrease in survival. CPR continues between shocks. Epinephrine 1 mg IV q3-5 min. Amiodarone 300 mg IV push (then 150 mg) if VF/pVT persists after 2-3 shocks.
Key clinical rule: In any wide-complex tachycardia, assume VT until proven otherwise. Treating SVT with aberrancy as VT is safe; treating VT as SVT (e.g., giving verapamil) can be fatal.
Sources: Braunwald's Heart Disease (Ch. 67), Fuster and Hurst's The Heart 15e (Ch. on VF/PMVT), Rosen's Emergency Medicine (Ch. 5)
This is a shared conversation. Sign in to Orris to start your own chat.