dermoid cyst
Reading File
Finding Sources
Searching PubMed
"dermoid cyst" pathology management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have thorough content from multiple textbooks. Let me compile a comprehensive answer.
Dermoid Cyst
Definition and Origin
A dermoid cyst is a choristoma - histologically normal tissue found in an abnormal location. It arises from displacement of ectodermal elements into a subcutaneous plane during embryonic development, specifically along lines of embryonic closure or fusion. It differs from an epidermoid cyst in that it contains skin appendages (hair follicles, sebaceous glands, sweat glands) within its wall, whereas epidermoids do not.
Dermoid cysts arise from both ectoderm and mesoderm and contain all the structures of normal skin.
- Kanski's Clinical Ophthalmology, 10th Ed.
- Andrews' Diseases of the Skin
Histology
The cyst wall is lined by keratinizing stratified squamous epithelium containing:
- Lanugo hair / hair follicles
- Sebaceous lobules
- Eccrine and apocrine glands
- Smooth muscle (sometimes)
Portions of the lining may show a wavy eosinophilic "shark tooth" pattern resembling steatocystoma. The wall has a fibrous outer layer.
- Andrews' Diseases of the Skin, p. 780
- Dermatology 2-Volume Set 5e
Locations
Dermoid cysts occur at multiple anatomic sites, each with its own clinical profile:
1. Cutaneous / Head and Neck (Most Common in Pediatrics)
- Along embryonic closure zones on the face:
- Lateral eyebrow (external angular dermoid) - most common facial site
- Nasal root and nasal dorsum
- Midline forehead
- Mastoid process region
- Floor of mouth
- Scalp midline (frontal to occipital)
- Also: chest, back, abdomen, perianal area
- Nasal and external angular dermoids may show familial clustering (genetic component)
- Usually present within the first year of life (70% identified by age 5)
- Typical lesion: few mm to several cm, firm, cystic, non-pulsatile, does not transilluminate
- Tethered to underlying tissues; overlying skin usually free
- A pit or punctum with a tuft of hair may be present
2. Orbital (Eye)
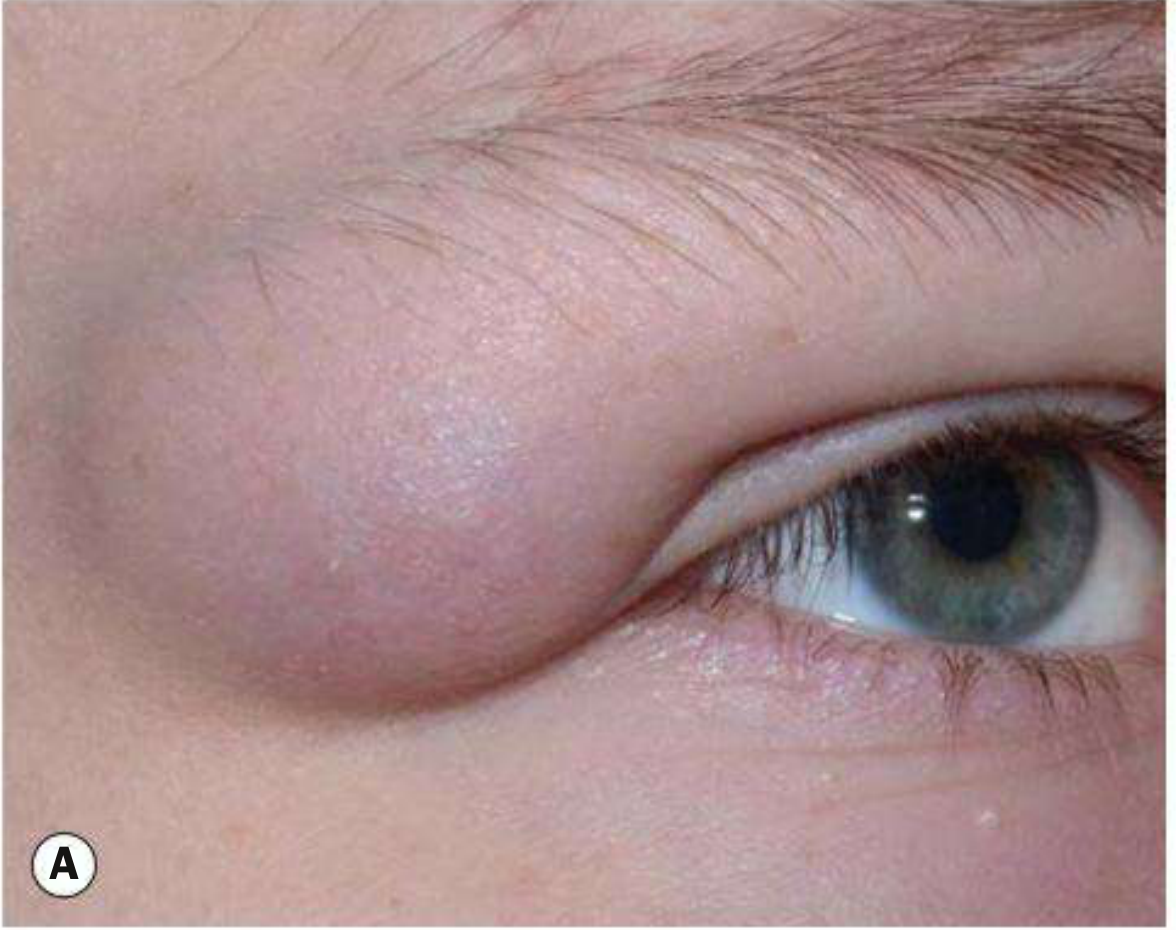
Fig: Superficial orbital dermoid cyst in a child (Kanski's Clinical Ophthalmology)
Orbital dermoids are among the most frequently encountered orbital tumors in children.
- Superficial: presents in infancy as a painless, firm, smooth nodule 1-2 cm, usually superotemporal or superonasal orbit; mobile under skin, tethered to periosteum; posterior margins easily palpable
- Deep: presents in adolescence or adult life with gradual proptosis, dystopia, or acute inflamed orbit due to rupture
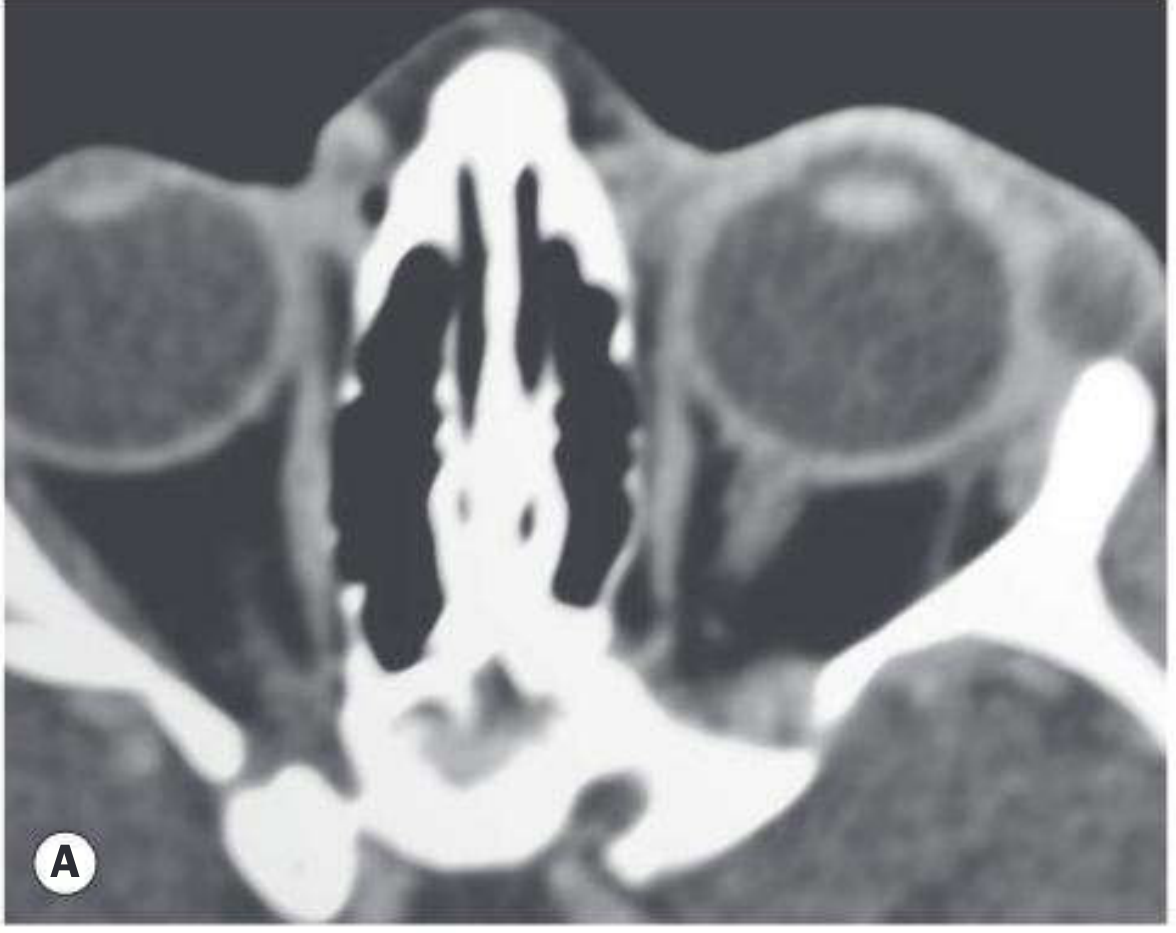
Fig: Axial CT showing a well-circumscribed heterogeneous superficial orbital dermoid (Kanski's)
- Kanski's Clinical Ophthalmology, 10th Ed.
3. Nasal / Midline
- Most common midline nasal mass
- Account for 1-3% of all dermoids
- Presents as a slowly growing midline cystic mass over the nasal dorsum with an associated pit (from nasal tip to glabella); hair may protrude
- 4-45% have an intracranial component - preoperative CT and MRI are mandatory
- Scott-Brown's Otorhinolaryngology
4. Neck (Midline)
- Usually asymptomatic midline neck lesion
- Does not elevate with tongue protrusion (unlike thyroglossal duct cyst, which does)
- May become infected
- Keratin-filled (vs. thyroglossal duct cysts which are mucus-filled - needle puncture can differentiate them)
- K.J. Lee's Essential Otolaryngology
5. Ovarian (Mature Cystic Teratoma)
Ovarian dermoid cysts (mature cystic teratomas) are the most common benign ovarian neoplasm. They can contain hair, teeth, sebaceous material, and other tissues.
- Most patients are asymptomatic; some have pelvic pain
- Complication: ovarian torsion - absent vascularity on Doppler is a key sign
- Can rarely secrete parathyroid hormone (causing hypercalcemia)
- Associated with autoimmune hemolytic anemia
- Evaluation: transvaginal ultrasound + tumor markers (CA125, b-HCG, AFP, LDH depending on concern for malignancy)
MRI findings of ovarian dermoid: High signal on T1 (fat content) with signal suppression on T1 fat-saturation sequences - classic and diagnostic.
- Sabiston Textbook of Surgery
- Grainger & Allison's Diagnostic Radiology
6. Spinal
- Patients with spina bifida frequently develop dermoid cysts of the repaired spinal column
- Dermoids overlying the lower spine may be associated with tethered cord and late ambulatory difficulties
- Dermal sinuses/dermoids associated with occult spinal dysraphism findings: hyperpigmented patches, skin tags, hemangiomas, hairy nevi
Complications
| Complication | Notes |
|---|---|
| Rupture | Triggers intense foreign body granulomatous reaction from extruded hair and keratin |
| Infection | May present as abscess; can spread to CNS (if intracranial connection) or lungs (if pleural connection) |
| Tethered cord | Spinal dermoids |
| Proptosis | Deep orbital dermoids |
| Ovarian torsion | Ovarian dermoids |
| Intracranial extension | Nasal and scalp dermoids (4-45% of nasal dermoids) |
| Malignant transformation | Rare; squamous cell carcinoma reported in ovarian dermoids |
Investigations
- CT: assesses bony anatomy and bony defects
- MRI: delineates CNS connection; mandatory for midline scalp, nasal, and spinal dermoids before surgery
- Ultrasound: first-line for ovarian dermoids (echogenic contents, Rokitansky protuberance)
- MRI pelvis: fat signal on T1, suppressed on fat-sat = pathognomonic for ovarian dermoid
- Needle puncture: keratin (dermoid) vs. mucus (thyroglossal duct cyst) at bedside differentiation
Key rule: Before operating on any midline dermoid of the back, scalp, nasal area, or face, CT and/or MRI must exclude intracranial or intraspinal communication. Lateral eyebrow dermoids may be an exception. - Andrews' Diseases of the Skin
Treatment
| Location | Treatment |
|---|---|
| Cutaneous / periorbital | Surgical excision in toto; imaging first if midline or near cleavage planes |
| Orbital (superficial) | Excision in toto - do not rupture the cyst wall (causes granulomatous inflammation) |
| Orbital (deep) | Surgical excision; neurosurgical referral if intracranial extension |
| Nasal / scalp | CT + MRI first; neurosurgical referral if intracranial component |
| Neck (midline) | Simple cystectomy after resolution of any infection |
| Ovarian | Laparoscopic ovarian cystectomy (appropriate regardless of size); oophorectomy for large ones replacing the ovary |
Critical surgical point: When removing any dermoid cyst, avoid rupturing the wall - spillage of contents (especially hair and sebaceous material) causes severe granulomatous or chemical inflammation in the surrounding tissue.
Key Differentials
- Epidermoid cyst: No adnexal structures in wall; both epidermoid and dermoid present as smooth subcutaneous nodules
- Thyroglossal duct cyst: Elevates with tongue protrusion; mucus-filled; midline neck; Sistrunk procedure required (not simple cystectomy)
- Branchial cleft cyst: Lateral neck; lined by squamous or ciliated columnar epithelium
- Nasal glioma: Firm nasal mass; contains glial tissue; does not transilluminate or pulsate
- Encephalocele: Pulsatile; transilluminates; expands with crying
Sources: Andrews' Diseases of the Skin, Kanski's Clinical Ophthalmology 10th Ed., Scott-Brown's Otorhinolaryngology Head & Neck Surgery, K.J. Lee's Essential Otolaryngology, Dermatology 2-Volume Set 5e, Sabiston Textbook of Surgery, Grainger & Allison's Diagnostic Radiology
epdermoid cyst vs dermoid cyst
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have excellent content from multiple authoritative sources. Here is the full comparison:
Epidermoid Cyst vs. Dermoid Cyst
These two entities are often confused because they look similar clinically and share a stratified squamous epithelial lining - but they are distinct in origin, histology, contents, location, and clinical behavior.
Side-by-Side Comparison
| Feature | Epidermoid Cyst | Dermoid Cyst |
|---|---|---|
| Synonyms | Epidermal inclusion cyst, infundibular cyst, sebaceous cyst (misnomer) | Congenital inclusion dermoid cyst |
| Origin | Follicular infundibulum (hair follicle); also from traumatic/surgical implantation of epidermis | Displacement of ectoderm along embryonic closure lines during development |
| Embryology | Acquired (traumatic) or follicular disruption; developmental in some cases | Purely congenital - forms during embryonic fusion |
| Epithelial lining | Keratinizing stratified squamous epithelium WITH granular layer | Keratinizing stratified squamous epithelium WITH granular layer |
| Skin appendages in wall | ABSENT - no hair follicles, no sebaceous glands, no sweat glands | PRESENT - hair follicles, sebaceous glands, eccrine glands, apocrine glands, smooth muscle |
| Cyst contents | Laminated keratin (white, cheesy, malodorous) | Laminated keratin + hair, sebum, oily material |
| Punctum | Often present (derived from follicle) | May be present (pit); a tuft of hair may protrude |
| Common locations | Face, upper trunk, back, neck, scrotum - anywhere on skin | Along embryonic fusion lines: lateral eyebrow, nasal root, midline scalp, floor of mouth, orbit, midline neck/nasal dorsum |
| Age at presentation | Any age; adults most common | Usually infancy/childhood (70% by age 5); deep orbital type in adolescence/adults |
| Tethering | Mobile; not tethered to underlying bone | Often tethered to periosteum or deep structures |
| Intracranial/intraspinal connection | No | Yes - possible (4-45% of nasal dermoids have intracranial component) |
| Associations | Gardner syndrome (FAP), basal cell nevus syndrome, acne vulgaris, BRAF inhibitors, cyclosporine | Spina bifida, occult spinal dysraphism, tethered cord; familial clustering for nasal/eyebrow types |
| Malignant potential | Rare BCC or SCC within cyst | Rare (SCC); ovarian dermoids rarely undergo malignant transformation |
| Imaging differentiator | No fat signal | Fatty content on MRI/CT = pathognomonic for dermoid |
| Treatment | Excision (best when "cold"/non-inflamed); incision & drainage if infected; triamcinolone for inflammation | Surgical excision in toto; imaging mandatory before midline dermoids; neurosurgical referral if CNS connection |
The Single Most Important Histological Difference
"The difference between these two entities is histological - the more common dermoid cyst contains skin appendages such as sebaceous glands and hair follicles, while an epidermoid cyst is entirely ectodermal."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Both have a squamous epithelial lining with a granular layer - but the dermoid has skin appendages embedded in its wall; the epidermoid does not.
Histology in Detail
Epidermoid Cyst
- Cyst wall: stratified squamous epithelium with an intact granular layer
- Contents: laminated orthokeratotic debris (keratin)
- Rupture causes: foreign body giant cell / suppurative granulomatous inflammation
- In Gardner syndrome: characteristic shadow cells (pilomatricoma-like) may project into cavity
Dermoid Cyst
-
Cyst wall: keratinizing stratified squamous epithelium with a granular layer + skin appendages (hair follicles, sebaceous lobules, eccrine/apocrine glands, smooth muscle)
-
May show a "shark tooth" wavy eosinophilic pattern in portions of the lining (resembles steatocystoma)
-
Contents: keratin + hair + sebaceous/oily material
-
Rupture causes: intense foreign body granulomatous reaction (hair acts as a persistent irritant)
-
Dermatology 2-Volume Set 5e, Fitzpatrick's Dermatology
Clinical Differentiation Points
When they look the same:
Both are smooth, firm, skin-colored subcutaneous nodules. Both can have a punctum. Both can become infected or inflamed.
Clues pointing to epidermoid:
- Adult patient
- Located on face, back, trunk (non-midline)
- History of acne, trauma, or prior surgery at the site
- Not tethered to bone
- Multiple cysts in Gardner syndrome context
Clues pointing to dermoid:
- Infant/child
- Midline or along embryonic cleavage lines (lateral eyebrow, nasal root, midline scalp, floor of mouth)
- Tethered to periosteum - cannot be fully moved away from underlying bone
- Hair protruding from a pit
- Do not transilluminate
- Family history (nasal/angular dermoids)
- Fatty content on imaging = pathognomonic
Imaging: The Key Differentiator
| Modality | Epidermoid | Dermoid |
|---|---|---|
| Ultrasound | Anechoic to heterogeneous; no fat signal | Variable; fatty nodules may appear as "marbles" |
| CT | Homogeneous low-attenuation; no fat density | Low-attenuation central cavity; fat density may be visible |
| MRI | Low T1, high T2 (simple cyst signal) | High T1 signal (fat); suppressed on T1 fat-sat = pathognomonic |
"Fatty content is pathognomonic for a dermoid but in its absence, differentiation by imaging is not possible."
- Scott-Brown's Otorhinolaryngology
Critical Clinical Rule (Dermoid Only)
Before attempting excision of any dermoid cyst along the midline (nasal dorsum, scalp, spinal column), CT and MRI are mandatory to exclude intracranial or intraspinal communication. This rule does not apply to epidermoid cysts.
Summary Table: Quick Reference
| Epidermoid | Dermoid | |
|---|---|---|
| Appendages in wall | ✗ | ✓ |
| Congenital | Sometimes | Always |
| Midline / embryonic fusion | Occasionally | Characteristically |
| Tethered to periosteum | ✗ | ✓ |
| CNS connection risk | ✗ | ✓ |
| Fat on MRI | ✗ | ✓ |
| Pre-op imaging required | No (superficial) | Yes (midline locations) |
Sources: Dermatology 2-Volume Set 5e; Andrews' Diseases of the Skin; Scott-Brown's Otorhinolaryngology; Kanski's Clinical Ophthalmology 10th Ed.; Fitzpatrick's Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.