RMGIC images
RMGIC resin modified glass ionomer cement microstructure images histology
RMGIC SEM scanning electron microscopy interface dentin images clinical
RMGIC (Resin-Modified Glass Ionomer Cement) - Images & Overview
Composition & Background
- Acid-base reaction (like conventional GIC) - forms a calcium/aluminum polyacrylate hydrogel matrix
- Free-radical polymerization (light or self-cure) - forms a poly-HEMA matrix
- The two matrices interpenetrate, producing the hybrid structure
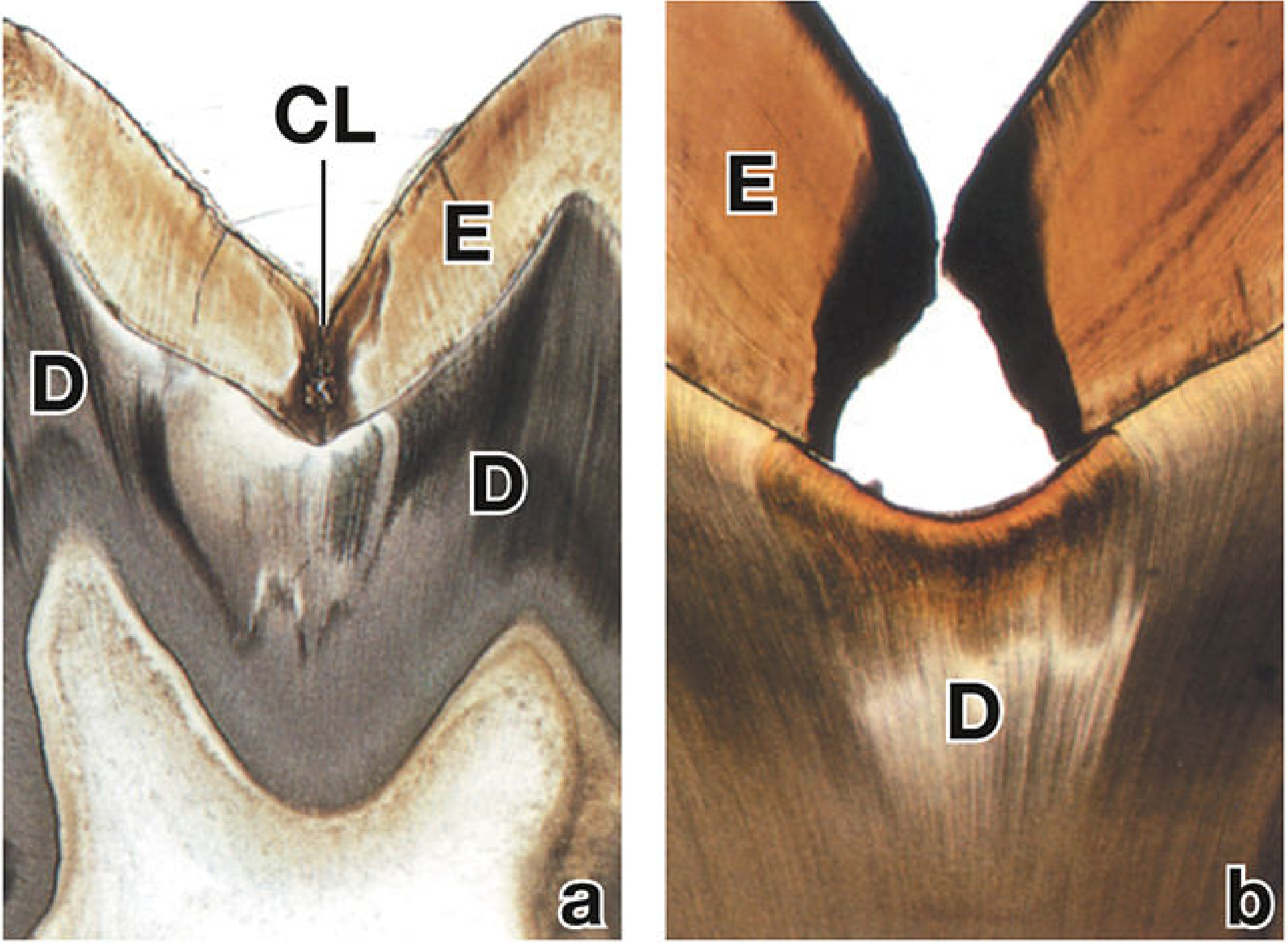
1. Carious Lesion Requiring Restoration (Ground Section, Light Microscopy)
2. SEM Microstructure - Comparative GIC/RMGIC Surfaces
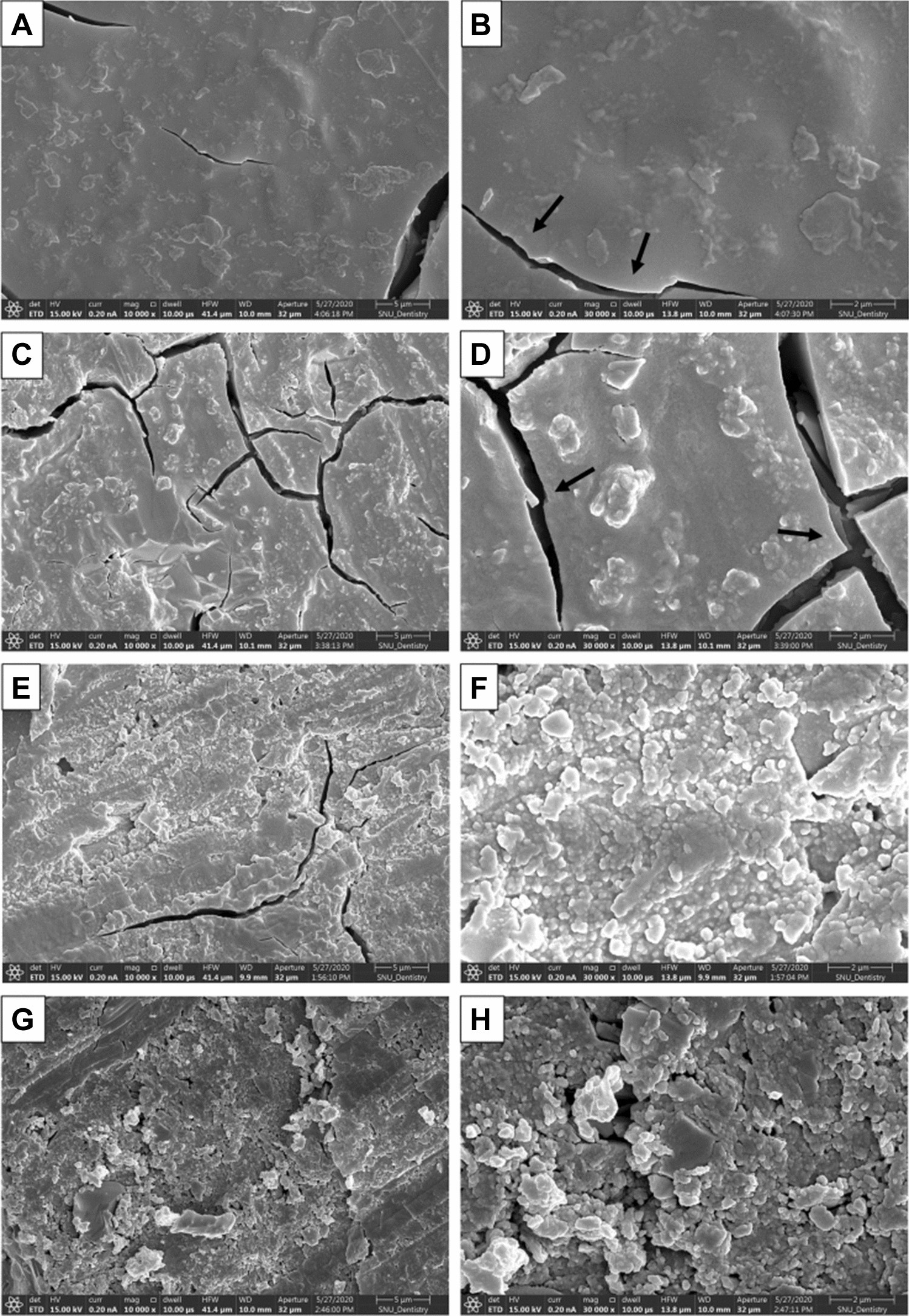
- A-B: Conventional GIC surface - relatively smooth matrix with scattered filler particles; surface cracks (arrows) from dehydration/shrinkage
- C-D: Early-generation RMGIC - increased cracking pattern, irregular filler particle distribution (arrows)
- E-F: Modern RMGIC - more homogeneous matrix, dense rounded filler particles, reduced cracking
- G-H: High-viscosity formulation - abundant irregular filler particle aggregates embedded in polyHEMA matrix
3. Internal Microstructure - Cross-section Backscattered SEM & Light Microscopy
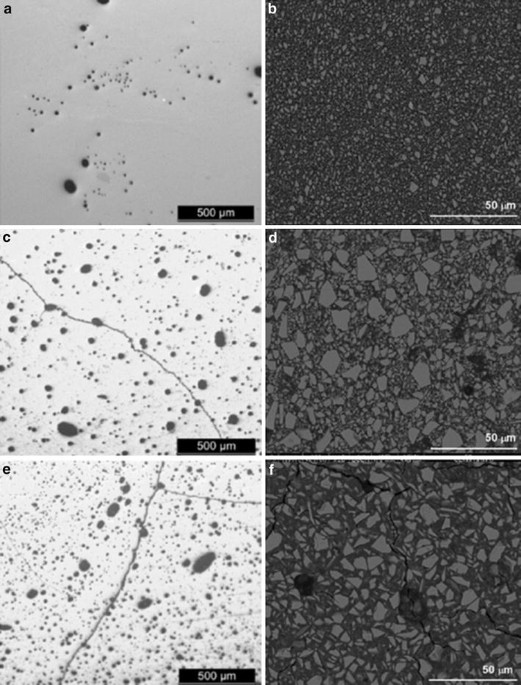
- (a, c, e) - Light microscopy at 500 µm scale: shows distribution of pores (dark ovals) and filler particles throughout the cement matrix. RMGIC (e) shows fewer large pores compared to conventional GIC (a)
- (b, d, f) - Backscattered SEM at 50 µm scale: shows filler glass particles (bright/grey) embedded in the polyacrylate-polyHEMA hybrid matrix (dark). RMGIC (f) shows denser, more uniform filler packing
Key Clinical Properties Illustrated by These Images
| Property | Relevance |
|---|---|
| Dual matrix (polyacrylate + polyHEMA) | Better mechanical properties than conventional GIC |
| Fluoride release | Anti-cariogenic - remineralizes adjacent tooth structure |
| Chemical adhesion to tooth | No need for separate bonding agent |
| Translucency | Aesthetic use in anterior restorations |
| Lower solubility than GIC | Better marginal integrity |
Clinical Applications
- Class III/V cavity restorations
- Core build-up
- Liner/base under composite
- Cementation of crowns/bridges/orthodontic brackets
- Pediatric dentistry (primary teeth)
mesoporous zinc oxide nanoparticles in GIC showing antimicrobial properties ..generate a image
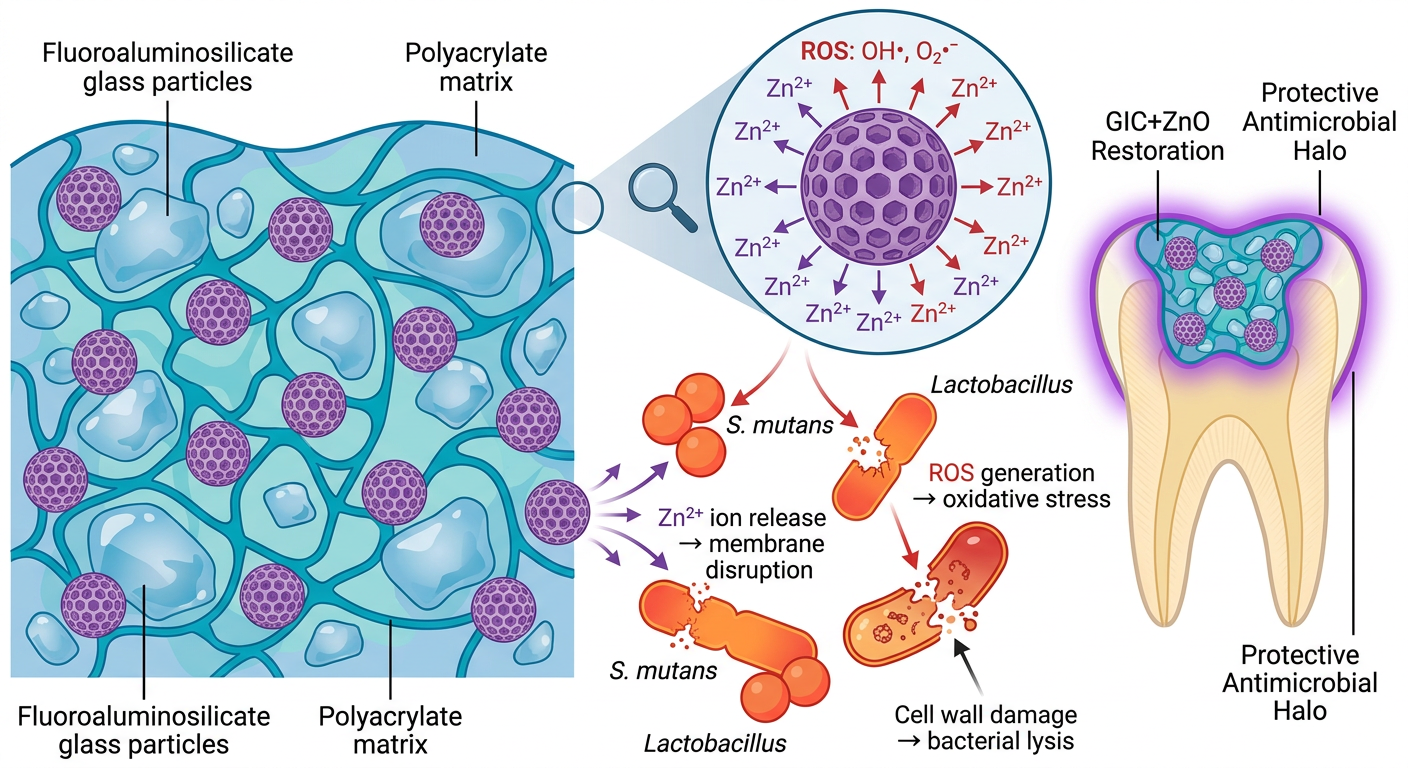
- Mesoporous ZnO nanoparticles are distributed within the conventional GIC matrix (fluoroaluminosilicate glass + polyacrylate)
- The porous architecture gives a high surface-area-to-volume ratio, maximizing ion release
- Zn²⁺ ion release - zinc ions leach from the pores, disrupting bacterial cell membrane integrity and inhibiting enzyme activity
- ROS generation - ZnO produces reactive oxygen species (OH•, O₂•⁻) under ambient/light conditions, causing oxidative stress and DNA damage in bacteria
- Physical membrane disruption - direct contact of nanoparticles with bacterial cell walls (S. mutans, Lactobacillus) causes structural lysis
- Targets secondary caries at restoration margins - a key failure mode of conventional GIC
- Synergistic with GIC's own fluoride release (remineralization + antimicrobial dual action)
- Mesoporous structure sustains slow, prolonged Zn²⁺ release rather than a burst effect
- Particularly relevant for high-caries-risk patients and pediatric restorations
140 human molar crowns were used after separating them from their roots at the cementoenamel junction with a water-cooled, low-speed diamond saw (Mecatome T201 A, Presi, Grenoble, France). The roots were discarded, and the crowns were randomly assigned into two groups: 70 samples for testing bond strength to enamel, and 70 for evaluating adhesion to dentin. To prepare enamel surfaces, a 0.5 mm-deep flat area was created in the center of the buccal surface of each crown using the cutting machine mentioned above. Each crown was then embedded in acrylic resin blocks (Acropars, Marlic Medical Industries Co., Tehran, Iran), positioning the buccal surface facing upward and level with the base. The enamel was polished gently with 320-grit silicon carbide abrasive paper (Starcke GmbH & Co. KG, Melle, Germany) to ensure surface uniformity. Enamel quality and flatness were examined using a stereomicroscope (Stemi 305, Carl Zeiss AG, Oberkochen, Germany). For the dentin group, the occlusal enamel and superficial dentin layers were removed to expose flat mid-coronal dentin using the same saw, under continuous water cooling. The dentin surfaces were also embedded in acrylic blocks with the surface aligned parallel to the base. A smear layer was created by polishing the exposed dentin for 60 s with 320-grit silicon carbide paper. Finally, the surfaces were rinsed and lightly dried using an air–water spray syringe (DABI Atlante, São Paulo, Brazil). Before bonding the RMGIC to the prepared enamel and dentin surfaces, a conditioning step was performed using GC Cavity Conditioner (GC Corporation, Tokyo, Japan) in accordance with the manufacturer's guidelines. The conditioner was applied to the tooth surface using a cotton pellet or applicator sponge. It was allowed to react for 10 s, after which the surface was thoroughly rinsed with water and gently blotted dry, leaving the surface moist but not desiccated.