Multiparametric mri in prostate malignancy Trans rectal usg vs mri of prostate gland Development ,imaging modalities of prostate MRI prostate Answer each of these radiology questions for 10 marks each for radiology pg exam use standard radiology textbooks or radio Pedia also collect diagrams from internet which can be easily drawn for respective ans
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
multiparametric MRI prostate PI-RADS zones diagram radiology
Finding Sources
Finding Sources
Finding Sources
Searching the Web
PI-RADS v2 scoring prostate MRI zones diagram radiology exam
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Here are four comprehensive 10-mark answers for your Radiology PG exam, based on Grainger & Allison's Diagnostic Radiology, Campbell-Walsh Urology, and standard radiological practice:
RADIOLOGY PG EXAM ANSWERS - PROSTATE GLAND
Q1. MULTIPARAMETRIC MRI (mpMRI) IN PROSTATE MALIGNANCY (10 Marks)
Introduction
Multiparametric MRI (mpMRI) of the prostate combines anatomical and functional sequences to optimise prostate cancer (PCa) detection, localisation, local staging, risk stratification, biopsy guidance, and treatment planning. It has become the gold-standard imaging tool in the prostate cancer diagnostic pathway.
Sequences in mpMRI (the "Multi" Parameters)
mpMRI comprises THREE essential components:
| Sequence | Abbreviation | Role |
|---|---|---|
| T2-weighted imaging | T2WI | Zonal anatomy, lesion detection, staging |
| Diffusion-weighted imaging | DWI/ADC | Tumour cellularity (primary sequence for PZ) |
| Dynamic contrast-enhanced MRI | DCE | Tumour vascularity/angiogenesis |
| T1-weighted imaging | T1WI | Post-biopsy haemorrhage detection |
(Source: Grainger & Allison's Diagnostic Radiology)
1. T1-Weighted Imaging (T1WI)
- Prostate parenchyma is isointense on T1 - no anatomical detail
- Primary use: detect post-biopsy haemorrhage (T1 hyperintense foci)
- Larger FOV up to aortic bifurcation: assess lymph nodes and bone metastases
- A minimum 6-week interval between biopsy and MRI is advised to reduce false-positive T2 staging due to haemorrhage
2. T2-Weighted Imaging (T2WI)
- High-resolution, multiplanar (axial, sagittal, coronal), slice thickness 3 mm, no gap
- Depicts zonal anatomy of the prostate, seminal vesicles, capsule
- Peripheral Zone (PZ): Normal = homogeneous intermediate-to-high signal; thin T2-hypointense rim = capsule
- PCa appears as focal low signal intensity area
- High-grade tumours (Gleason 4/5): lower SI; Low-grade (Gleason 2/3): mildly hypointense/isointense
- Transition Zone (TZ): Heterogeneous due to BPH ('organised chaos')
- PCa sign: ill-defined homogeneous T2 hypointense lesion = 'Erased Charcoal Drawing Sign'
- Also: lenticular/fusiform anterior lesion, spiculated margins, loss of pseudocapsule
- T2WI is the dominant (primary) sequence for Transition Zone in PI-RADS v2
3. Diffusion-Weighted Imaging (DWI) + ADC Map
- Shows random Brownian motion of water molecules
- PCa has high cell density → restricted diffusion → bright on high b-value DWI, dark on ADC map
- ADC values are inversely proportional to diffusion restriction; PCa has significantly lower ADC than normal tissue
- High-grade tumours (Gleason 4/5) show lower ADC than low-grade tumours
- Recommended b-values: 50-100 s/mm², 800-1000 s/mm², and computed/acquired ≥1400 s/mm²
- DWI is the dominant (primary) sequence for Peripheral Zone in PI-RADS v2
- Slice thickness ≤4 mm, in-plane dimension ≤2.5 mm
4. Dynamic Contrast-Enhanced MRI (DCE)
- Gadolinium-based contrast: exploits tumour angiogenesis (VEGF-driven)
- PCa shows early, intense enhancement + early washout compared to normal parenchyma
- Role: minor/adjunct when T2WI and DWI quality is good
- Key role: upgrades a PI-RADS 3 peripheral zone lesion to PI-RADS 4 if DCE is positive
- Does NOT influence scoring at PI-RADS 1, 2, 4, or 5
- Clinically significant cancer cannot be excluded solely based on absent early enhancement
PI-RADS v2 Scoring System
Developed jointly by ESUR + ACR + AdMeTech Foundation (2015), PI-RADS v2 standardises mpMRI reporting on a 5-point scale:
| PI-RADS | Likelihood | Action |
|---|---|---|
| 1 | Very low | No biopsy |
| 2 | Low | No biopsy |
| 3 | Equivocal | Consider biopsy (DCE role here) |
| 4 | High | Biopsy recommended |
| 5 | Very high | Biopsy recommended |
Clinically significant PCa = Gleason ≥7 (including 3+4), and/or volume ≥0.5 cc, and/or extraprostatic extension
Scoring rule:
- Peripheral Zone: DWI is dominant; DCE can upgrade DWI 3 → PI-RADS 4
- Transition Zone: T2WI is dominant; DWI 5 can upgrade T2 score 3 → PI-RADS 4
PI-RADS v2 Flowchart (Grainger & Allison, Fig. 32.3)
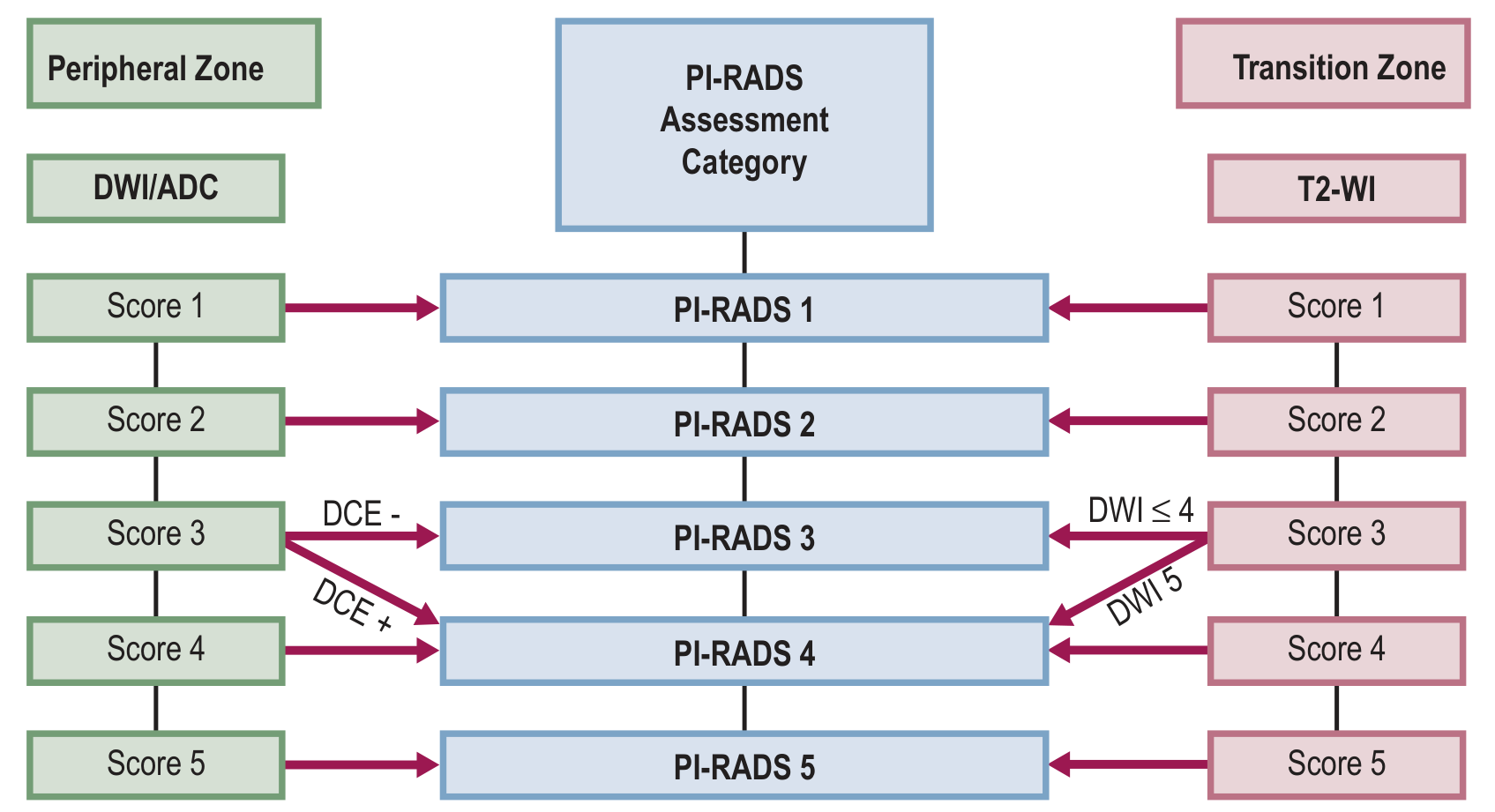
Diagram to draw in exam:
PI-RADS Assessment Category
|
PERIPHERAL ZONE | TRANSITION ZONE
(DWI dominant) | (T2WI dominant)
|
DWI Score 1 ---------> PI-RADS 1 <--------- T2 Score 1
DWI Score 2 ---------> PI-RADS 2 <--------- T2 Score 2
DWI Score 3 + DCE- --> PI-RADS 3 <--------- T2 Score 3 + DWI ≤4
DWI Score 3 + DCE+ --> PI-RADS 4 <--------- T2 Score 3 + DWI 5
DWI Score 4 ---------> PI-RADS 4 <--------- T2 Score 4
DWI Score 5 ---------> PI-RADS 5 <--------- T2 Score 5
Technical Requirements
- Field strength: 3 Tesla preferred (better SNR, spatial/temporal resolution)
- 1.5T acceptable without endorectal coil
- Endorectal coil: Optional - improves SNR but causes prostate deformation, artefacts, patient discomfort
- External phased-array coil recommended
- Protocol: T2WI + DWI + DCE (mandatory); T1WI (optional)
Clinical Applications
- Primary detection - triage to avoid unnecessary biopsy (PROMIS trial: 27% of patients avoided biopsy)
- Targeted biopsy guidance - via cognitive fusion, MRI/TRUS software fusion, or "in-bore" MRI biopsy
- Local staging - extracapsular extension, seminal vesicle invasion
- Active surveillance - monitor low-risk disease
- Treatment planning - radiation therapy targeting (MRI volumes 10% smaller than CT)
- Post-treatment recurrence - T2WI for biochemical recurrence localisation
(Source: Grainger & Allison's Diagnostic Radiology, Chapter 32; Campbell-Walsh Urology, Chapter 150)
Q2. TRANSRECTAL USG vs MRI OF THE PROSTATE GLAND (10 Marks)
Introduction
Both TRUS and MRI are established imaging modalities for prostate evaluation. The choice depends on indication, availability, and clinical context.
Comparison Table
| Parameter | TRUS | MRI |
|---|---|---|
| Modality | High-frequency ultrasound (7-10 MHz) | Magnetic resonance (1.5T / 3T) |
| Radiation | None | None |
| Cost | Low, widely available | High, limited availability |
| Real-time | Yes | No |
| Guidance for biopsy | Direct, real-time | Indirect (fusion) or "in-bore" |
| Soft tissue contrast | Moderate | Excellent |
| Zonal anatomy | Limited | Excellent (T2WI) |
| Cancer detection sensitivity | Low (echogenicity overlap) | High (mpMRI) |
| Functional imaging | Limited (Doppler, elastography) | Full (DWI, DCE) |
| Staging accuracy | Lower | Higher (capsule, ECE, SVI) |
| Anterior prostate | Poor access | Excellent |
| Patient comfort | Mild discomfort | Claustrophobia possible |
| Operator dependence | High | Moderate |
TRUS - Details
Technique:
- 7-10 MHz bi-planar transducer inserted transrectally
- Sagittal + transverse planes
- Volume calculation: prolate ellipsoid formula = L × W × H × 0.523
Normal Sonographic Anatomy:
- Peripheral zone: uniform hypoechoic (central gland echogenic)
- Surgical capsule: echogenic line
- Seminal vesicles: symmetrical paired structures superior-posterior
Uses of TRUS:
- Prostate volume measurement (essential for PSA density calculation)
- TRUS-guided systematic biopsy - 12-core extended sextant biopsy (gold standard access route for random biopsy)
- Colour Doppler - increased vascularity at tumour sites
- TRUS + Elastography - tissue stiffness mapping
- Contrast-enhanced TRUS - emerging technique
- Guidance for brachytherapy seed implantation
- Drainage of prostatic abscess
Limitations of TRUS:
- 60-70% of PCa is isoechoic to background (invisible)
- Cannot assess anterior prostate, apex, or periurethral zone adequately
- Cannot assess extracapsular extension reliably
- Operator-dependent
- Cannot differentiate cancer from prostatitis, BPH nodules
MRI - Details (See also Q1 and Q4)
Advantages of MRI over TRUS:
- Superior soft tissue contrast
- Better zonal anatomy depiction
- Accurate capsular assessment - extracapsular extension (ECE), seminal vesicle invasion (SVI)
- Identifies anterior and transition zone tumours
- Multi-parametric functional data (DWI, DCE)
- Systematic staging via PI-RADS
- Nodal and bone marrow assessment on T1WI
- RDOG study: MRI shows higher sensitivity and specificity than endorectal ultrasound for ECE detection
MRI-TRUS Fusion Biopsy:
- Best of both worlds: MRI identifies suspicious lesion, TRUS guides real-time needle
- Software-based image co-registration
- Three techniques: (a) In-bore MRI biopsy, (b) Cognitive fusion, (c) MRI/TRUS software fusion
- Allows targeted biopsy of PI-RADS 3-5 lesions
Diagram to Draw in Exam:
PROSTATE IMAGING COMPARISON
TRUS MRI
├─ 7-10 MHz transducer ├─ 1.5T / 3T magnet
├─ Transrectal approach ├─ External phased-array coil
├─ Real-time guided biopsy ├─ mpMRI protocol
├─ Volume measurement ├─ T2WI: anatomy + staging
├─ Doppler vascularity ├─ DWI: cancer detection
└─ Limited cancer detection └─ DCE: vascularity
MRI-TRUS FUSION BIOPSY:
[MRI lesion map] + [Real-time TRUS] = Targeted needle placement
(Source: Grainger & Allison's Diagnostic Radiology, Chapters 32 & 81; Bailey and Love's Surgery)
Q3. DEVELOPMENT AND IMAGING MODALITIES OF PROSTATE GLAND (10 Marks)
A. EMBRYOLOGICAL DEVELOPMENT
Origin:
- The prostate develops from the urogenital sinus (endodermal origin)
- Outgrowths of urogenital sinus epithelium invade the surrounding urogenital mesenchyme
- Begins at 10-12 weeks of gestation
- Development is androgen-dependent (dihydrotestosterone / DHT via 5-alpha reductase)
- Full secretory function only at puberty under testosterone influence
Key structures:
| Structure | Embryological Origin |
|---|---|
| Prostatic epithelium | Endodermal urogenital sinus |
| Prostatic stroma | Urogenital mesenchyme |
| Bladder trigone | Mesonephric (Wolffian) duct |
| Seminal vesicles | Mesonephric duct |
(Source: Campbell-Walsh Urology; Smith & Tanagho's General Urology)
B. ANATOMY (McNeal's Zonal Anatomy - 1981)
McNeal described four zones:
| Zone | % of prostate | Location | Significance |
|---|---|---|---|
| Peripheral Zone (PZ) | 70% | Posterior-lateral; palpable on DRE | 70-75% of PCa arise here |
| Transition Zone (TZ) | 5-10% | Periurethral; surrounds urethra | Site of BPH; 25% of PCa |
| Central Zone (CZ) | 20-25% | Surrounds ejaculatory ducts, base | Rarely involved by PCa |
| Anterior Fibromuscular Stroma | - | Anterior prostate | No glandular tissue |
Diagram to Draw in Exam (Zonal Anatomy - ESSENTIAL):
PROSTATE ZONAL ANATOMY - Axial View (Mid-gland)
ANTERIOR
___________________
| ANTERIOR |
| FIBROMUSCULAR |
| STROMA (AFS) |
|___________________|
| TRANSITION |CZ |
| ZONE (TZ) | | <- Ejaculatory ducts
|______________|___|
| |
| PERIPHERAL ZONE (PZ) |
|___________________________|
POSTERIOR
(Palpable on DRE)
Urethra runs through centre of TZ
C. IMAGING MODALITIES FOR PROSTATE
1. Plain X-Ray
- Not useful for prostate itself
- May show prostatic calcifications (corpora amylacea)
- IVU: Indentation on bladder base in BPH
2. Ultrasound (TRUS)
- First-line imaging for prostate
- Volume measurement, biopsy guidance
- Normal appearance: PZ hypoechoic, CG echogenic
- Colour Doppler: vascularity in PCa
- Limitations: PCa often isoechoic, operator-dependent
3. CT Scan
- NOT useful for primary tumour detection - poor soft tissue contrast
- Staging role: lymph node assessment (N staging), osseous metastases
- CT is primary for N/M staging in high-risk PCa
- Cannot distinguish tumour from BPH within prostate
4. MRI (mpMRI - See Q1 and Q4 for details)
- Gold standard for local staging
- T2WI: anatomy, capsular integrity
- DWI: tumour detection
- DCE: vascularity
- PI-RADS v2 reporting
- 3T preferred; no endorectal coil needed at 3T
5. Bone Scintigraphy (Tc-99m MDP)
- Standard for bone metastases detection
- Recommended for: PSA >20, Gleason >7, T3/T4 disease
- Hot spots at sites of osteoblastic metastases
- Superscan in widespread disease
6. PET-CT
- Choline PET-CT: Early PCa, biochemical recurrence
- PSMA PET-CT (Ga-68 PSMA): Highly sensitive for PCa; PCa cells overexpress PSMA
- Superior to bone scan + CT for staging and restaging
- Increasingly preferred over choline PET
- Detects disease at PSA levels as low as 0.2 ng/mL
- NaF PET-CT: Bone-specific, more sensitive than bone scan for skeletal metastases
7. TRUS-Guided Biopsy
- 12-core extended sextant systematic biopsy
- MRI-TRUS fusion for targeted biopsy
8. Multiparametric TRUS (mpTRUS)
- Analogous to mpMRI: combines B-mode + Doppler + contrast enhancement + elastography
- Emerging alternative/complement to mpMRI
Q4. MRI OF THE PROSTATE GLAND (10 Marks)
Introduction
MRI of the prostate is the most accurate imaging modality for local staging of prostate cancer. The development of multiparametric MRI (mpMRI) has transformed the prostate cancer diagnostic pathway.
Technical Requirements
Scanner:
- 3T preferred (higher SNR, better spatial and temporal resolution)
- 1.5T is acceptable without endorectal coil
- 3T without endorectal coil = diagnostic quality equivalent to 1.5T with endorectal coil
Coils:
- External phased-array pelvic coil - standard of care
- Endorectal coil (optional): improves SNR but deforms prostate, increases cost, patient discomfort, artefacts
Contraindications:
- Metallic implants, pacemakers, claustrophobia
- Post-biopsy waiting: 6 weeks (haemorrhage resolution)
MRI Sequences and Protocols
1. T1-Weighted Imaging
- Prostate isointense: no zonal anatomy
- Detects post-biopsy haemorrhage (T1 hyperintense)
- Large FOV: nodal + bone marrow assessment
- Fat-saturation versions: improves nodal detection
2. T2-Weighted Imaging (Anatomical Sequence)
- Key sequence for anatomy and staging
- Multiplanar: axial (mandatory), coronal, sagittal
- Slice thickness 3 mm, no gap; in-plane ≤0.7 mm × 0.4 mm
- FOV 12-20 cm, covering prostate + seminal vesicles
Normal Zonal Anatomy on T2WI:
| Zone | T2 Signal |
|---|---|
| Peripheral zone | Homogeneous high signal (bright) |
| Transition zone | Heterogeneous intermediate (BPH = 'organised chaos') |
| Central zone | Low-intermediate signal |
| Capsule | Thin T2-hypointense rim |
| Seminal vesicles | High signal (fluid-filled) |
T2WI: PCa Features:
Peripheral Zone (PZ):
- Focal low signal intensity area
- High-grade: markedly low SI
- Low-grade: mildly hypointense or isointense
Transition Zone (TZ):
- 'Erased charcoal drawing' sign - ill-defined homogeneous T2 hypointense lesion
- Lenticular/fusiform anterior lesion
- Spiculated/irregular margins
- Loss of pseudocapsule
T2WI PI-RADS Categories (Peripheral Zone) - Fig. 32.5, Grainger & Allison
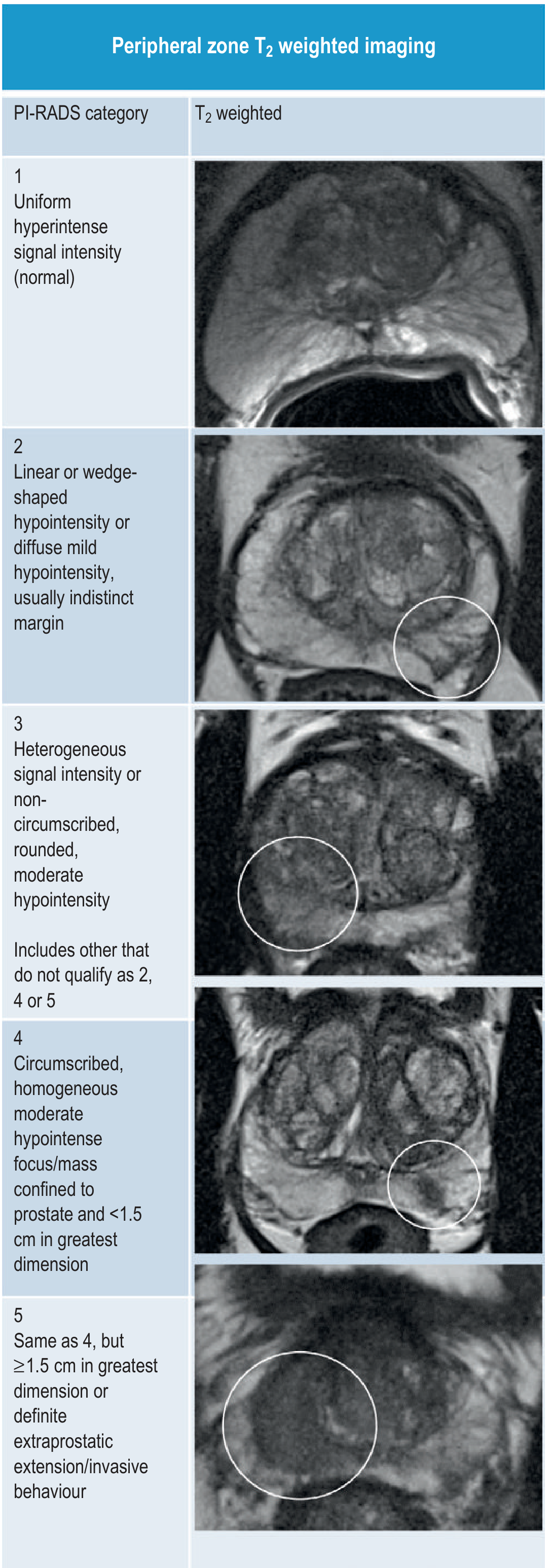
Peripheral Zone T2WI PI-RADS:
- 1: Uniform hyperintense (normal)
- 2: Linear/wedge-shaped hypointensity, indistinct margin
- 3: Heterogeneous, non-circumscribed, rounded moderate hypointensity
- 4: Circumscribed, homogeneous, moderate hypointensity, <1.5 cm
- 5: Same as 4 but ≥1.5 cm OR definite extraprostatic extension
3. Diffusion-Weighted Imaging (DWI)
Physics: Brownian motion of water molecules
- High b-value images: Restricted diffusion = bright signal (cancer)
- ADC map: Restricted diffusion = dark (low ADC value); inverse relationship
- Cancer has HIGH cell density → RESTRICTED diffusion → HIGH signal on DWI, LOW ADC
ADC values:
- Normal PZ: high ADC (fluid-rich tubular structures, especially >50 years)
- PCa: significantly lower ADC than normal tissue
- High-grade PCa (Gleason 4/5): lower ADC than low-grade (Gleason 3)
Technique: Free-breathing spin-echo, spectral fat saturation; b-values: 50-100, 800-1000, and ≥1400 s/mm²; slice thickness ≤4 mm
DWI PI-RADS Categories (PZ):
- 2: Non-focal hypointense ADC
- 3: Focal, mildly/moderately hypointense ADC + iso/mildly hyperintense high b-value DWI
- 4: Focal, markedly hypointense ADC + marked hyperintensity on high b-value, <1.5 cm
- 5: Same as 4 but ≥1.5 cm or extraprostatic extension
4. Dynamic Contrast-Enhanced MRI (DCE)
Principle: Gadolinium-based CA → exploits tumour angiogenesis (VEGF-driven neovascularisation)
PCa kinetics:
- Early, intense enhancement + early washout (type 3 curve)
- Due to increased vascular permeability and AV shunting
Role in PI-RADS v2:
- Positive DCE = focal area of earlier onset enhancement than surrounding normal tissue
- DCE upgrades PZ PI-RADS 3 to PI-RADS 4 (the only upgrade role)
- Does NOT influence PI-RADS 1, 2, 4, or 5 scoring
- Visual assessment of early enhancement phase is recommended
- Gadolinium: dose 0.1 mmol/kg, temporal resolution <10 seconds per dynamic phase
Staging with MRI - TNM
| Stage | MRI Finding |
|---|---|
| T2a/b | Tumour confined to one/both lobes; intact capsule |
| T3a | Extracapsular extension (ECE) - irregular capsular bulge, obliteration of rectoprostatic angle |
| T3b | Seminal vesicle invasion - T2 low signal, non-tapering, asymmetric enlargement |
| T4 | Invasion of adjacent structures (bladder, rectum) |
Signs of ECE on MRI:
- Irregular or spiculated margin
- Asymmetric neurovascular bundle
- Obliteration of rectoprostatic angle
- Direct tumour extension beyond capsule
MRI in Prostate Cancer Pathway
Elevated PSA / Abnormal DRE
|
mpMRI (PI-RADS scoring)
|
PI-RADS 1-2 PI-RADS 3 PI-RADS 4-5
No biopsy Consider biopsy MRI-TRUS fusion
(monitor) (clinical factors) targeted biopsy
|
Histological diagnosis
|
Staging MRI (T/N/M staging)
|
Treatment planning (surgery / RT / surveillance)
MRI in Active Surveillance
- Serial mpMRI monitoring for low-risk PCa on active surveillance
- Detects disease upgrading or progression
- Guides repeat biopsy only when PI-RADS changes
MRI vs CT vs Bone Scan for Staging
| Modality | T staging | N staging | M (bone) |
|---|---|---|---|
| mpMRI | Excellent | Moderate | Poor |
| CT | Poor | Good | Moderate |
| Bone scan | Not applicable | Not applicable | Good |
| PSMA PET-CT | Good | Excellent | Excellent |
Prostate MRI - Summary Box (for quick revision)
Protocol: T2WI + DWI + DCE (+ T1WI optional)
PI-RADS v2: 5-point scale, PZ = DWI dominant, TZ = T2WI dominant
3T without endorectal coil: Standard recommendation
Key cancer sign T2WI PZ: Focal low signal intensity
Key cancer sign DWI: Bright on high b-value + dark on ADC map
Key cancer sign DCE: Early enhancement + early washout
Clinical significance threshold: Gleason ≥7, volume ≥0.5 cc, or extraprostatic extension
Sources: Grainger & Allison's Diagnostic Radiology (9780323760751), Chapter 32; Campbell-Walsh Urology (9780323546423), Chapter 150; Smith & Tanagho's General Urology; Bailey & Love's Short Practice of Surgery.
This is a shared conversation. Sign in to Orris to start your own chat.