copd in detail in easy languages
Reading File
Finding Sources
Searching PubMed
"COPD" AND "chronic obstructive pulmonary disease"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the information needed to write a comprehensive, easy-language explanation of COPD. Let me compose it now.
COPD (Chronic Obstructive Pulmonary Disease) - A Complete, Easy-Language Guide
What Is COPD?
COPD stands for Chronic Obstructive Pulmonary Disease. Let's break that down:
- Chronic = long-lasting, it does not go away
- Obstructive = something is blocking air from flowing out freely
- Pulmonary = related to the lungs
- Disease = a medical condition
Simply put, COPD is a lung disease where air gets trapped inside the lungs because the airways are damaged or blocked. The lungs can't empty properly, making it hard to breathe - especially to breathe OUT.
COPD is actually an umbrella term that covers two main conditions that almost always occur together:
- Emphysema - the air sacs in the lungs are destroyed
- Chronic Bronchitis - the airways are inflamed and produce too much mucus
How Do Healthy Lungs Work?
Think of your lungs like a sponge. When you breathe in, air travels through the windpipe (trachea) into two main tubes (bronchi), which branch into smaller tubes (bronchioles), and finally into millions of tiny balloon-like air sacs called alveoli. Oxygen passes through the thin walls of these alveoli into your blood, and carbon dioxide (a waste gas) goes the other way - from blood into the air sacs to be breathed out.
In healthy lungs, these walls are elastic - like rubber bands - and spring back easily to push air out.
What Goes Wrong in COPD?
1. Emphysema - "The Destroyed Sponge"
Toxic chemicals (mainly from cigarette smoke) trigger immune cells called neutrophils to flood into the lungs. These cells release enzymes called proteases that eat away at the elastic walls of the air sacs.
- The tiny air sacs merge into large, floppy spaces - like a sponge whose holes have merged into big, useless cavities
- The lungs lose their "spring-back" ability
- Air gets trapped inside - the chest puffs up (called a barrel chest)
- There is less surface area for oxygen to enter the blood
2. Chronic Bronchitis - "The Mucus Factory"
Smoke also damages the airways (bronchi and bronchioles):
- The mucus-producing glands in the airways grow bigger (hyperplasia)
- Normal cells transform into mucus-secreting cells (goblet cell metaplasia)
- The tiny hair-like structures (cilia) that normally sweep mucus out are paralyzed by smoke
- Mucus piles up and blocks the airways
- The airway walls thicken from inflammation and scarring
Clinical definition: Chronic bronchitis = a productive cough (coughing up mucus) for at least 3 months per year, for at least 2 consecutive years.
Most COPD patients have BOTH emphysema AND chronic bronchitis at the same time, just in different proportions.
Who Gets COPD? (Risk Factors)
The #1 cause is cigarette smoking - responsible for the vast majority of cases. About 15-30% of habitual smokers develop COPD, though new research shows lung changes happen in even more smokers than previously thought.
Other risk factors include:
| Risk Factor | Details |
|---|---|
| Cigarette / tobacco smoking | The biggest risk factor by far |
| Air pollution | Indoor (cooking fires, biomass fuel) and outdoor |
| Occupational dust/fumes | Coal, grain dust, chemical fumes |
| Alpha-1 antitrypsin deficiency | A genetic condition; causes early-onset emphysema |
| Childhood lung infections | Recurrent infections can impair lung development |
| Premature birth | Lungs may not develop fully |
| Family history | Genetic variants (MMP-12, IL-33 pathway) increase risk |
Alpha-1 antitrypsin is a protein made by the liver that normally protects lungs from protease damage. People who are born with low levels have weak lung defenses and can develop emphysema even without smoking. - Goldman-Cecil Medicine, p. 895
Symptoms - What Does COPD Feel Like?
Symptoms develop slowly over years - people often don't notice until the disease is already moderate or severe.
Early Symptoms
- Shortness of breath on exertion (breathlessness when climbing stairs or walking fast) - the #1 hallmark
- Chronic cough - often first dismissed as "smoker's cough"
- Mucus/sputum production - coughing up thick phlegm, especially in the morning
As the Disease Worsens
- Breathlessness even at rest
- Wheezing (a whistling sound when breathing)
- Chest tightness
- Barrel chest (the chest expands and stays puffed out due to trapped air)
- Pursed lip breathing - patients unconsciously breathe out through pursed lips to slow exhalation and keep airways open
- Use of accessory muscles (neck and shoulder muscles) to help breathe
- Cyanosis - bluish tinge to lips/fingers from low oxygen (more common in chronic bronchitis)
- Weight loss and muscle wasting (especially in emphysema)
Advanced/Late Symptoms
- Cor pulmonale - right-sided heart failure from strain caused by pulmonary hypertension
- Signs of right heart failure: swollen ankles, distended neck veins, enlarged liver
- Hypoxemia (low blood oxygen) and Hypercapnia (high CO2 buildup)
- Depression - a very common but under-recognized comorbidity
Classic textbook picture: A 65-year-old heavy smoker, barrel-chested, short of breath, with a history of winter bronchitis attacks that worsened over years. - Costanzo Physiology, p. 3036
How Is COPD Diagnosed?
1. History and Physical Exam
The doctor asks about:
- Smoking history (how many years, how many cigarettes per day)
- Cough and sputum history
- Breathing difficulty during daily activities
- Family history of lung disease
Physical findings: barrel chest, wheezing, use of accessory muscles, reduced breath sounds, cyanosis, signs of right heart failure.
2. Spirometry (Lung Function Test) - The Gold Standard
This is the key test. You blow as hard and fast as you can into a machine called a spirometer. It measures:
- FEV1 = how much air you can blow out in 1 second
- FVC = the total air you can blow out in a full breath
- FEV1/FVC ratio = the key number
In COPD: FEV1/FVC ratio < 0.70 (less than 70%) confirms airflow obstruction. - Goldman-Cecil Medicine, p. 896
Here is what the spirometry flow-volume loop looks like in COPD vs. normal lungs:
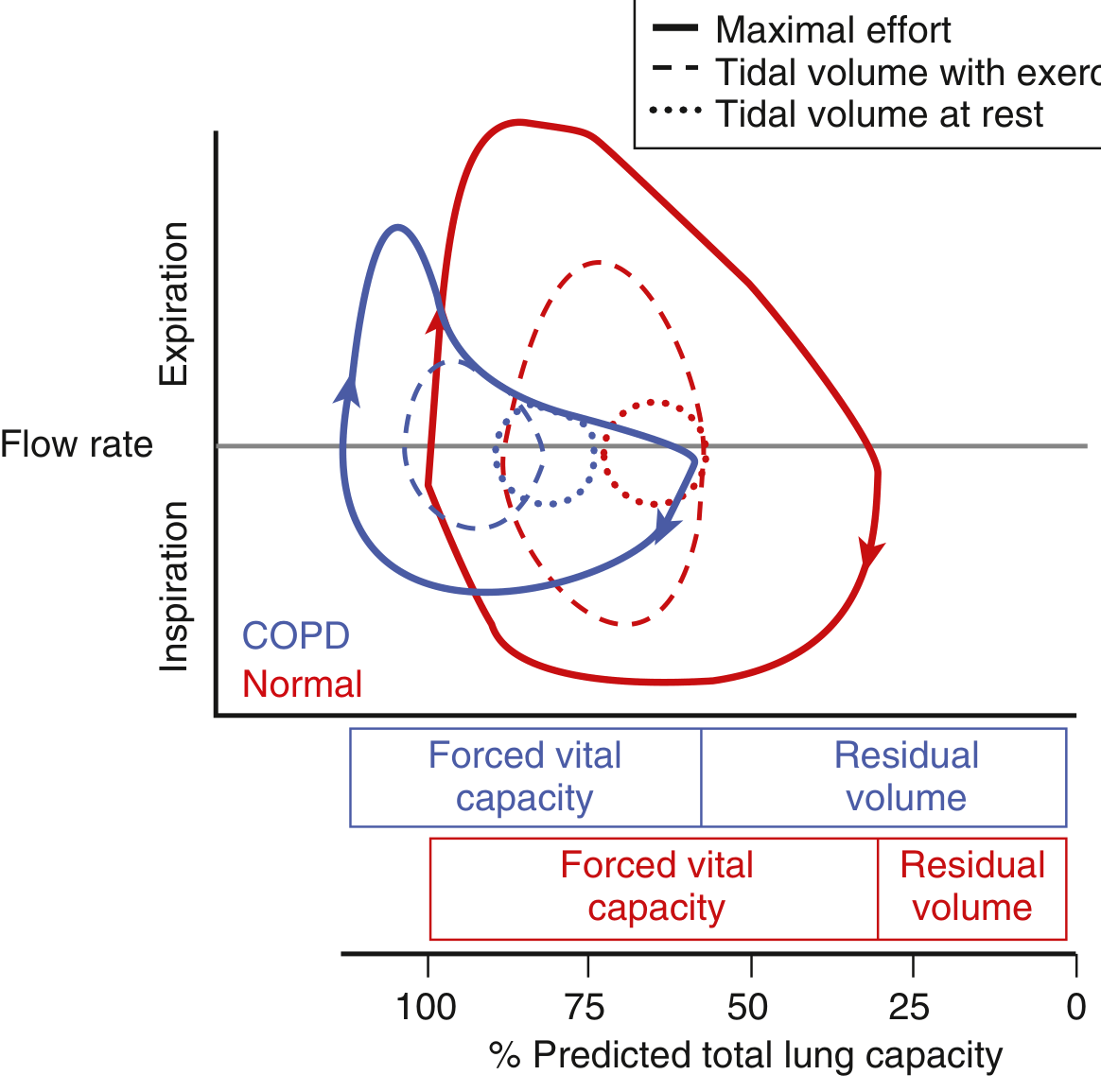
The blue (normal) loop is tight and efficient. The red (COPD) loop is much wider, shifted to the right - showing air trapped inside even after a full exhale.
3. GOLD Classification (Severity Staging)
The GOLD guidelines (Global Initiative for Chronic Obstructive Lung Disease) classify COPD severity by FEV1 (% of what's predicted/normal):
| GOLD Stage | FEV1 % Predicted | Severity |
|---|---|---|
| GOLD 1 | ≥80% | Mild |
| GOLD 2 | 50-79% | Moderate |
| GOLD 3 | 30-49% | Severe |
| GOLD 4 | <30% | Very Severe |
Modern GOLD guidelines also assess symptoms (using the COPD Assessment Test or mMRC dyspnea scale) and exacerbation history to guide treatment decisions.
4. Other Tests
- Chest X-ray - shows hyperinflation (flat diaphragm, increased airspace), bullae
- CT scan - better detail for emphysema, bullae, pulmonary hypertension; also used for lung cancer screening
- Arterial Blood Gas (ABG) - measures blood oxygen and CO2 levels
- Alpha-1 antitrypsin level - all adults with COPD should be tested once
- ECG - checks for heart involvement
- Blood eosinophil count - helps decide whether to use inhaled steroids
Pathophysiology in Plain English (What's Happening Physically)
The core problem is: air can get in, but can't easily get out.
- The damaged airways and destroyed air sac walls create resistance to airflow
- Expiration (breathing out) becomes slow and incomplete
- The lungs operate at a higher volume than normal - air gets "trapped"
- When you exercise and breathe faster, there's not enough time to fully exhale before the next breath - this is called dynamic hyperinflation
- Hyperinflation pushes the diaphragm flat and puts it at a mechanical disadvantage - it can't work as well
- The breathing muscles have to work much harder just to move a normal breath
- The gap between effort and result causes the distressing sensation of breathlessness
The body partially compensates by:
- Increasing breathing rate
- Pursed-lip breathing
- Using accessory muscles
- Raising red blood cell production (to carry more oxygen)
COPD Exacerbations ("Flare-Ups")
An exacerbation is a sudden worsening of symptoms beyond the normal day-to-day variation. These are medical emergencies that drive most hospitalizations and deaths.
Triggers
- Respiratory infections (viral - like cold/flu; or bacterial)
- Air pollution
- Non-compliance with medications
Symptoms of Exacerbation
- Increased breathlessness
- More coughing, often with more or different-colored sputum
- Wheezing, chest tightness
How Bad Is It? (Deciding on Hospital vs. Home)
Criteria for hospitalization:
- Severe worsening of symptoms
- Significant comorbidities (heart disease, etc.)
- Failure of initial treatment at home
- Confusion or altered mental status
- Very low oxygen saturation
Criteria for ICU:
- Need for mechanical ventilation (breathing machine)
- Hemodynamic instability
- Severe acidosis despite oxygen and non-invasive ventilation
Treatment of Exacerbations
- Short-acting bronchodilators (SABAs) - albuterol inhaler or nebulizer - first line
- Anticholinergics - ipratropium - added if SABAs not enough
- Systemic corticosteroids - prednisone 40 mg/day for 5 days reduces inflammation
- Antibiotics - because many exacerbations involve bacterial infection (H. influenzae, S. pneumoniae, Moraxella catarrhalis; Pseudomonas in high-risk patients)
- Oxygen therapy - carefully (excessive O2 can suppress the breathing drive in severe COPD)
- Non-invasive ventilation (NIV/BiPAP) - helps support breathing without intubation
Treatment of Stable COPD
COPD cannot be cured, but it can be managed to slow progression, reduce symptoms, and prevent exacerbations.
1. Stop Smoking (Most Important Step)
Quitting smoking is the single most effective thing a patient can do. It significantly slows the rate of lung function decline.
2. Bronchodilators (Open the Airways)
These relax the muscles around airways to make breathing easier.
- SABAs (Short-acting beta-agonists) - e.g., albuterol - for quick relief
- LABAs (Long-acting beta-agonists) - e.g., salmeterol, formoterol - daily use for ongoing symptoms
- SAMAs (Short-acting muscarinic antagonists) - e.g., ipratropium - quick relief
- LAMAs (Long-acting muscarinic antagonists) - e.g., tiotropium - considered first-line for persistent symptoms
- Combinations of LABA + LAMA work better than either alone
3. Inhaled Corticosteroids (ICS)
Less effective in COPD than in asthma. Recommended only for:
- Severe airflow obstruction
- Frequent exacerbations
- History of asthma
- High blood eosinophil count (a biomarker suggesting steroid response)
- Note: ICS increases risk of bacterial pneumonia, so it's not used routinely
4. Phosphodiesterase Inhibitors
- Roflumilast - a non-steroid anti-inflammatory pill that reduces exacerbation frequency in severe COPD with chronic bronchitis
5. Oxygen Therapy (Long-Term)
Given for patients with chronic low oxygen levels (resting SpO2 ≤ 88%). Improves survival.
6. Pulmonary Rehabilitation
Exercise training, breathing techniques, education, and nutritional support. Proven to reduce breathlessness and improve quality of life.
7. Vaccinations
- Annual flu vaccine
- COVID-19 and pneumococcal vaccines (Infections are the #1 trigger for exacerbations)
8. Surgical Options (Severe Cases)
- Lung volume reduction surgery (LVRS) - removing the worst-affected lung tissue so the rest can work better
- Lung transplantation - for end-stage COPD
- Bronchoscopic procedures - placing valves or coils to reduce hyperinflation
Complications
| Complication | What It Is |
|---|---|
| Pulmonary hypertension | High blood pressure in lung arteries from chronic hypoxia |
| Cor pulmonale | Right heart failure due to pulmonary hypertension |
| Respiratory failure | Severe drop in oxygen/rise in CO2 |
| Pneumothorax | A bleb (air bubble) on the lung surface ruptures, collapsing the lung |
| Lung cancer | COPD patients have ~2x the risk of lung cancer vs. smokers without COPD |
| Polycythemia | Body overproduces red blood cells to compensate for low oxygen |
| Malnutrition/sarcopenia | Emphysema patients often lose weight and muscle |
| Depression/anxiety | Very common, often under-treated |
COPD vs. Asthma - Key Differences
| Feature | COPD | Asthma |
|---|---|---|
| Age of onset | Usually >40 years | Often childhood/young adult |
| Main cause | Cigarette smoking | Allergens, triggers |
| Airflow obstruction | Mostly irreversible | Reversible (with treatment) |
| Inflammation type | Neutrophilic | Eosinophilic |
| Response to steroids | Partial/poor | Usually good |
| Progression | Slowly progressive | Usually episodic |
- Katzung's Basic and Clinical Pharmacology, p. 565
Prevention
- Don't smoke - or quit if you do. This is by far the most powerful prevention.
- Avoid occupational dust and chemical fumes
- Reduce indoor air pollution (e.g., improve ventilation for cooking fires)
- Get vaccinated against respiratory infections
- Treat childhood lung infections promptly
- Consider genetic testing (alpha-1 antitrypsin) if there's a family history
Key Numbers to Remember
| Parameter | Normal | COPD |
|---|---|---|
| FEV1/FVC ratio | >0.70 | <0.70 |
| SpO2 (resting) | 95-100% | May be <88% in severe cases |
| PaO2 | ~100 mmHg | May fall to 60 mmHg or lower |
| PaCO2 | ~40 mmHg | May rise (CO2 retention) |
Summary in 5 Simple Points
- COPD = damaged, blocked airways - mostly from years of smoking
- You can breathe in, but can't breathe out properly - air gets trapped
- Symptoms come on slowly - breathlessness, cough, mucus
- Diagnosed by a breathing test (spirometry) - FEV1/FVC < 0.70
- Cannot be cured, but can be managed - quitting smoking + inhalers + rehab
Sources: Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine, pp. 894-896; Katzung's Basic and Clinical Pharmacology, pp. 565-566; Costanzo Physiology (7th Ed.), pp. 3036-3059; Fishman's Pulmonary Diseases and Disorders; Washington Manual of Medical Therapeutics, p. 320
This is a shared conversation. Sign in to Orris to start your own chat.