Angiography
Reading File
Asking for Preferences
Finding Sources
Searching the Web
angiography types indications technique overview 2025
Reading File
Reading File
Finding Sources
Searching Images
angiography technique catheter contrast injection blood vessel
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Excellent — I now have thorough, multi-source textbook content. Here is the comprehensive overview:
Angiography — Overview
Definition
Angiography is an imaging technique used to visualize the lumen of blood vessels (arteries, veins, or cardiac chambers) by injecting radiopaque contrast medium and capturing images — most commonly with X-ray fluoroscopy, CT, or MRI. The term derives from Greek: angeion (vessel) + graphia (writing/recording).
Types of Angiography
| Type | Modality | Key Features |
|---|---|---|
| Conventional / DSA | X-ray fluoroscopy | Catheter-based; gold standard for many vascular beds |
| CT Angiography (CTA) | Multi-detector CT | Non-invasive; fast; widely available |
| MR Angiography (MRA) | MRI | No radiation; limited by metal implants and claustrophobia |
| Catheter / Invasive | Fluoroscopy | Allows simultaneous diagnosis + therapy |
| Nuclear / Radionuclide | Scintigraphy | Tagged RBCs; sensitive for slow/intermittent bleeding |
Digital Subtraction Angiography (DSA)
The classic invasive form. Pre-contrast ("mask") images are digitally subtracted from post-contrast images, removing overlying bone and soft tissue to leave only the opacified vessel. Intra-arterial DSA (IA-DSA) uses smaller volumes of dilute contrast, reducing renal toxicity and discomfort compared to older film-based methods. — Yamada's Textbook of Gastroenterology
CT Angiography (CTA)
Contrast is injected IV through a peripheral cannula; a rapid CT acquisition captures the arterial or venous phase. CTA can detect active bleeding extravasation down to 0.1–0.5 mL/min — superior to nuclear scintigraphy for localization.
MR Angiography (MRA)
Uses gadolinium contrast or flow-sensitive pulse sequences without ionising radiation. MRA can identify vessel anomalies and plaque morphology (fibrous cap, lipid core, intraplaque haemorrhage). Cannot be used in patients with ferromagnetic metal implants. — Current Surgical Therapy 14e
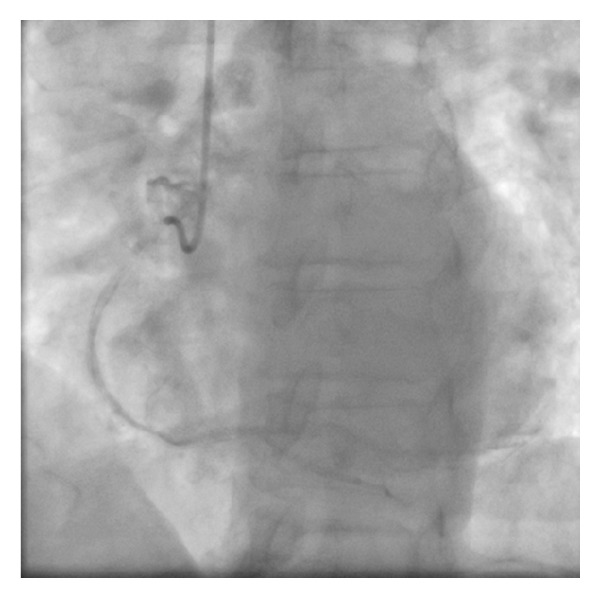
Fluoroscopic coronary angiogram: catheter in the aortic sinus, RCA being opacified with contrast.
Technique — Invasive Catheter Angiography
Vascular Access (Seldinger Technique)
- Needle puncture — An 18-gauge needle is most commonly used (accepts 0.035-inch guidewire). The Seldinger needle permits single- or double-wall puncture.
- Femoral artery (most common) — The common femoral artery (CFA) is punctured over the medial third of the femoral head under fluoroscopic guidance. Pulsatile back-bleeding confirms intraluminal position.
- Guidewire advancement — Always performed gently under fluoroscopy to prevent subintimal dissection or plaque disruption.
- Sheath placement — An arterial sheath is inserted over the guidewire; catheters are then exchanged through this sheath.
- Alternative access sites — Radial artery (increasingly preferred for coronary angiography), left brachial artery (avoids carotid origin; used when aorto-iliac disease precludes femoral access), or antegrade femoral access.
"Retrograde femoral access is the most common arterial access technique. Care should be taken to avoid puncturing the external iliac artery above the inguinal ligament because this can result in retroperitoneal haemorrhage." — Schwartz's Principles of Surgery
Selective vs. Non-selective Catheterisation
- Selective: Catheter tip placed directly into the target vessel's ostium (e.g., left or right coronary artery, coeliac axis). Provides superior image quality.
- Non-selective / flush: Contrast injected into the aorta; used when selective engagement is not possible or to survey all branches simultaneously.
Contrast & Image Acquisition
- Iodinated contrast medium is injected; rate and volume tailored to the vessel.
- Arterial and parenchymal phases are usually acquired for maximum diagnostic value.
- The hepatic veins are visible on routine DSA; the portal vein is not normally visualised on an arteriogram unless flow reversal or an arterioportal shunt is present. — Grainger & Allison's Diagnostic Radiology
Indications by Clinical Domain
| Domain | Indication |
|---|---|
| Cardiovascular | Coronary artery disease assessment; pre-operative valvular evaluation; congenital heart disease |
| Neurovascular | Carotid stenosis (when duplex US and CTA conflict); aneurysm; AVM; stroke |
| Peripheral vascular | Peripheral artery disease; limb ischaemia; aortic aneurysm |
| Gastrointestinal | Active GI haemorrhage (detects ≥0.5 mL/min); lower GI bleeding localisation + embolisation |
| Hepatic/Portal | Portal hypertension; TIPSS planning; transjugular hepatic venous pressure measurement |
| Trauma (neck) | Zone I and III penetrating neck injuries; carotid laceration, pseudoaneurysm; four-vessel angiography of bilateral carotid and vertebral arteries in bilateral zone I/III injuries — Cummings Otolaryngology |
| Urological | Renal artery stenosis; renal vascular lesions |
Accuracy: Angiography has a reported diagnostic accuracy of 96.5% for vascular injuries near zones I/III of the neck. — Cummings Otolaryngology
Contraindications
| Absolute / Relative | Condition |
|---|---|
| Absolute | Expanding haematoma with active bleeding; profound shock; uncontrolled haemorrhage |
| Relative | Contrast allergy (premedicate); contrast-induced nephropathy risk (hydration, N-acetylcysteine, low-osmolar agents); coagulopathy; severe renal failure |
Complications
- Contrast reactions: Severe allergy in ~0.1% of invasive angiographic procedures — Goldman-Cecil Medicine
- Contrast-induced nephropathy: Risk increases with pre-existing CKD, diabetes, and high contrast volume
- Access site: Haematoma (~4%), pseudoaneurysm, arteriovenous fistula, retroperitoneal haemorrhage
- Neurological: 2.6% neurologic complication rate reported in a review of ~20,000 DSA procedures (higher with atherosclerotic disease, frequent TIA, or intracranial haemorrhage) — Sabiston Textbook of Surgery
- Bowel ischaemia: Particularly during mesenteric angiography/embolisation
- Radiation exposure: Cumulative dose relevant in repeated procedures; the anesthesiologist must leave the room during DSA runs — Miller's Anesthesia
Therapeutic Applications (Interventional Angiography)
Beyond diagnosis, catheter access enables:
- Embolisation: Microcoil/microcatheter embolisation for GI bleeding (75–90% clinical success rate), trauma haemostasis, tumour devascularisation
- Thrombolysis / Thrombectomy: Intra-arterial tPA for stroke or peripheral occlusion
- Angioplasty + Stenting: PTA and stenting of peripheral, renal, carotid, or coronary arteries
- TIPSS: Transjugular intrahepatic portosystemic shunt for portal hypertension
- Intraarterial vasopressin infusion: For GI haemorrhage — potent vasoconstrictor
- Provocative angiography: Anticoagulant (heparin) + vasodilator (nicardipine) + urokinase administered to provoke intermittent/obscure bleeding for capture and embolisation
Current Role vs. Non-Invasive Imaging
| Scenario | Preferred Modality |
|---|---|
| Coronary artery disease screening | CTA (calcium score + CTA angiography) |
| Carotid stenosis workup | Duplex ultrasound → CTA (DSA only if both conflict) |
| Suspected PE | CT pulmonary angiography |
| Renal artery stenosis | CTA or MRA first-line |
| Active GI haemorrhage | CTA first → DSA if positive or haemodynamically unstable |
| Cerebral aneurysm | CTA/MRA for screening; DSA for treatment planning |
DSA is no longer recommended as a routine first-line diagnostic tool given improvements in CTA and MRA. Its current role is primarily therapeutic (interventional procedures) and as arbiter when non-invasive tests conflict. — Current Surgical Therapy 14e, Sabiston Textbook of Surgery
Sources: Grainger & Allison's Diagnostic Radiology | Schwartz's Principles of Surgery 11e | Sabiston Textbook of Surgery | Current Surgical Therapy 14e | Cummings Otolaryngology | Yamada's Textbook of Gastroenterology | Goldman-Cecil Medicine | Miller's Anesthesia 10e
Is angiography can be fatal procedure
Finding Sources
Searching PubMed
angiography mortality complications risk
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
coronary angiography mortality rate risk of death statistics
Reading File
Finding Sources
I now have solid data from multiple authoritative sources. Here is a thorough, honest answer:
Can Angiography Be Fatal?
Yes — but the risk of death is very low in elective, routine cases. Angiography is generally considered a safe procedure, yet it is not without risk, and fatal outcomes can occur, particularly in high-risk patients or emergency settings.
Mortality Figures
| Procedure | Risk of Death |
|---|---|
| Diagnostic coronary angiography | 0.07–0.25% (approximately 1 in 400–1,400 patients) |
| Diagnostic angiography in low-risk patients | As low as ~0.05% (~1 in 2,000) |
| DSA (cerebral/carotid) | Included in ~2.6% neurologic complication rate; death is a subset |
| Interventional PCI (therapeutic, not just diagnostic) | 30-day mortality ~1.55% overall; much higher (~10–40%) in patients with complex/obstructive CAD |
The mortality rate for coronary angiography ranges from 0.10% to 0.25% across different studies, with modern rates approaching 0.07% in experienced centres — almost all deaths occurring in patients already identified as high risk. — PubMed PMID 8972650; Goldman-Cecil Medicine
How Can Death Occur? — Life-Threatening Complications
1. Cardiovascular Collapse
- Coronary artery dissection or spasm during catheter manipulation → acute MI
- Ventricular fibrillation / cardiac arrest triggered by contrast injection into a coronary artery
- Acute occlusion of the left main coronary artery (the single highest-risk scenario)
2. Neurological (Stroke)
- Stroke risk: 0.05–0.1% in diagnostic procedures; 0.18–0.4% in interventional procedures
- Caused by catheter dislodging atheromatous plaques or air/thrombus embolism
- In a review of ~20,000 DSA patients, 2.6% had a neurologic complication — Sabiston Textbook of Surgery
- Cholesterol embolism: In a retrospective autopsy study, 27% of patients who died after arteriography had cholesterol embolism, vs. 4.3% in matched controls who did not undergo angiography — Fuster and Hurst's The Heart
3. Severe Contrast Reactions (Anaphylaxis)
- Severe contrast allergy occurs in ~0.1% of invasive angiographic procedures
- Anaphylactic shock from iodinated contrast can be fatal if not immediately treated
- Risk is higher in patients with prior contrast allergy, asthma, or atopy
4. Contrast-Induced Acute Kidney Injury (CI-AKI)
- Occurs in ~7.1% of coronary interventions
- Can progress to acute renal failure requiring dialysis; rarely fatal directly but contributes to mortality in critically ill patients
5. Haemorrhage
- Access site haematoma: ~4% with DSA
- Retroperitoneal haemorrhage: if the needle punctures the external iliac artery above the inguinal ligament — can be life-threatening
- Bowel ischaemia after mesenteric embolisation
6. Air Embolism / Catheter-Related Embolism
- Air introduced into the arterial system can cause coronary or cerebral air embolism
Patients at Highest Risk of Death
The following groups carry substantially higher procedural mortality:
- Left main coronary artery disease or 3-vessel CAD — the highest-risk subgroup
- Severe left ventricular dysfunction (EF <35%)
- Unstable angina / acute MI at time of procedure
- Haemodynamic instability / cardiogenic shock
- Advanced age with multiple comorbidities
- Severe renal impairment
- Previous stroke or frequent TIAs
"Almost all deaths occurred in patients known to be at higher risk." — PubMed data on coronary angiography mortality
What Minimises the Risk?
| Safety Measure | Effect |
|---|---|
| Experienced centre & operator | Mortality approaches 0.07% |
| Radial (wrist) access vs. femoral | Lower bleeding & vascular complications |
| Pre-medication for contrast allergy | Reduces anaphylaxis risk |
| IV hydration ± N-acetylcysteine | Reduces CI-AKI |
| Fluoroscopic guidance for access | Avoids retroperitoneal haemorrhage |
| Minimum contrast volume | Reduces nephropathy |
| Patient selection & timing | Elective > emergency in terms of safety |
Bottom Line
Angiography can be fatal, but in routine diagnostic cases performed in appropriate patients at experienced centres, the death rate is very low (~0.07–0.1%). The procedure becomes significantly more dangerous in haemodynamically unstable patients, those with severe coronary disease (especially left main disease), and those with contrast allergy or renal failure. The benefits of diagnosis and potential treatment almost always outweigh the risks — which is why it remains a standard procedure performed over 1 million times per year in the US alone.
Sources: Goldman-Cecil Medicine | Sabiston Textbook of Surgery | Fuster & Hurst's The Heart | Current Surgical Therapy 14e | PubMed (PMID 8972650)
What is door to needle time of angiography
Finding Sources
Finding Sources
Searching the Web
door to balloon time door to needle time STEMI angiography guidelines 2024
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.