TM joint
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have rich, comprehensive content. Let me compile the full answer.
Temporomandibular Joint (TMJ)
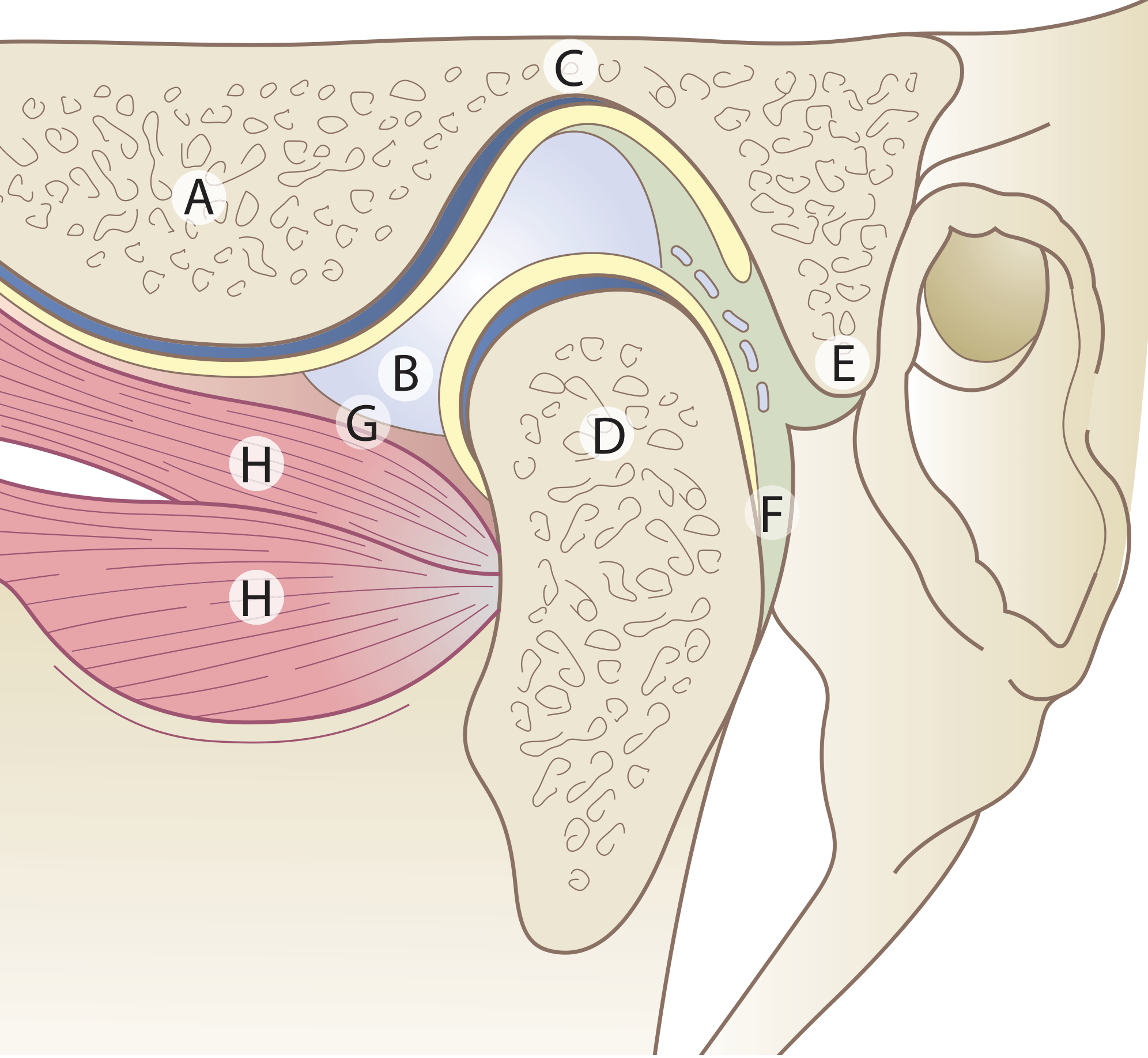
Figure: The TMJ - A = Articular eminence; B = Articular disc; C = Mandibular fossa; D = Condyle; E = Upper lamina (fibro-elastic); F = Lower lamina (non-elastic); G = Capsule; H = Lateral pterygoid muscle
Type and Formation
The TMJ (craniomandibular joint) is a synovial joint formed by the mandibular condyle articulating with the mandibular (glenoid) fossa of the temporal bone, just anterior to the external auditory canal. - Scott-Brown's Otorhinolaryngology, p. 693
Unique Features
The TMJ has several unusual characteristics that distinguish it from other synovial joints:
- Divided joint space - An intra-articular disc divides the joint into upper and lower cavities
- Fibrocartilage, not hyaline - Articular surfaces are fibrous tissue, reflecting the joint's intramembranous development
- Secondary condylar cartilage - Present in the condyle head until adolescence
- Tooth influence - Movements are influenced by the occlusion of teeth
Articular Disc
- A biconcave fibrocartilaginous disc sits between the condyle and temporal fossa
- Divides the joint into:
- Upper compartment (disc-temporal): permits gliding/translatory movement
- Lower compartment (disc-condylar): permits hinge/rotatory movement
- Anteriorly attached to the superior head of the lateral pterygoid muscle (in ~60% of people, fibres insert directly into the medial aspect of the disc's anterior border)
- Posteriorly, the bilaminar zone connects the disc to the retrodiscal tissue: the upper lamina is fibro-elastic (aids disc return), the lower lamina is non-elastic
Joint Capsule
- Attached above to the mandibular fossa (extending to just anterior to the articular eminence crest and posteriorly to the squamotympanic and petrotympanic fissures)
- Attached below to the neck of the condyle
- Thin and lax capsule
Ligaments
| Ligament | Role |
|---|---|
| Lateral (temporomandibular) ligament | Main ligament; limits lateral movement; runs from articular tubercle downward/backward to neck of condyle |
| Sphenomandibular ligament | Accessory; most influential on mandibular movement |
| Stylomandibular ligament | Reinforced band of deep cervical fascia; less functionally significant |
Muscles of Mastication
The muscles that move the TMJ:
| Muscle | Action |
|---|---|
| Masseter | Elevation (jaw closing) |
| Temporalis | Elevation + retraction |
| Medial pterygoid | Elevation + protrusion |
| Lateral pterygoid | Depression/opening + protrusion; both heads act together with functional heterogeneity; the superior head is active during opening |
| Digastric, mylohyoid, geniohyoid | Depression (jaw opening) |
Movements
- Mouth opening: combined rotation (lower compartment) + anterior translation of condyle down the articular eminence (upper compartment)
- Normal interincisal opening: 3-6 cm
- Protrusion / retrusion: gliding in upper compartment
- Lateral excursion: working side condyle rotates, balancing side condyle translates
Nerve and Blood Supply
- Nerve: Auriculotemporal nerve (branch of V3) - the main sensory supply; also masseteric and deep temporal branches
- Blood supply: Superficial temporal and maxillary arteries
Clinical Examination
- Palpate just anterior to the external auditory canal with jaw opening/closing and lateral excursion
- Assess for clicking, crepitus, tenderness, and range of motion
- Measure interincisal distance (normal 3-6 cm) - Firestein & Kelley's Rheumatology, p. 4608
TMJ Disorders
1. Internal Derangements
- Disc displacement (most common): anterior displacement with or without reduction
- With reduction: audible/palpable click on opening and closing
- Without reduction ("closed lock"): inability to fully open the mouth
2. TMJ Syndrome / Temporomandibular Disorder (TMD)
- Presents with: jaw pain, limited opening, clicking/crepitus, referred ear pain (close anatomical proximity to EAC)
- Thought to be related to bruxism and is considered a form of myofascial pain, similar to fibromyalgia
- Inflammatory cytokines (IL, TNF), matrix metalloproteinases, and VEGF may be elevated in synovial fluid
3. Arthritis
- Multiple arthritides affect the TMJ including juvenile and adult RA, osteoarthritis, psoriatic arthritis
- In children, RA of the TMJ can cause micrognathia (arrested mandibular bone growth)
4. Anterior Dislocation
- Condyle slips anteriorly over the articular eminence; muscle spasm prevents spontaneous reduction
- Unilateral: jaw deviates away from affected side
- Bilateral: jaw protrudes, mouth locked open, drooling, garbled speech, depression palpable over the TMJ
- Reduction technique: patient seated upright; thumbs/fingers in buccal sulcus pressing angle of jaw downward while rotating the chin upward and backward; gauze protection advised
- Rule out fracture-dislocation with Panorex/CT before blind reduction if trauma suspected - Rosen's Emergency Medicine, p. 194
Imaging
| Modality | Use |
|---|---|
| Panorex / Plain X-ray | Fractures, condyle position |
| CT scan | Bony architecture, condylar morphology, fracture detail |
| MRI | Gold standard for disc position, internal derangements, soft tissue pathology |
Key Clinical Pearl
The TMJ's close anatomical proximity to the external acoustic meatus means TMJ pathology commonly presents as otalgia (ear pain), which must be distinguished from primary ear disease. - Scott-Brown's, p. 693
Photo
Asking for Preferences
Finding Sources
Reading File
Reading File
Searching Content
"cdn.orris.care" in /textbooks/9781138094642
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Here are the TMJ anatomy diagrams sourced directly from medical textbooks:
TMJ Anatomy Diagrams
1. Sagittal Cross-Section - Articular Disc & Lateral Pterygoid (Scott-Brown's Otorhinolaryngology)
Key: A = Articular eminence | B = Articular disc | C = Mandibular fossa | D = Condyle | E = Upper lamina (fibro-elastic) | F = Lower lamina (non-elastic) | G = Capsule | H = Lateral pterygoid muscle (two heads)
2. MRI - TMJ Disc Translation During Mouth Opening (Imaging Anatomy Atlas)
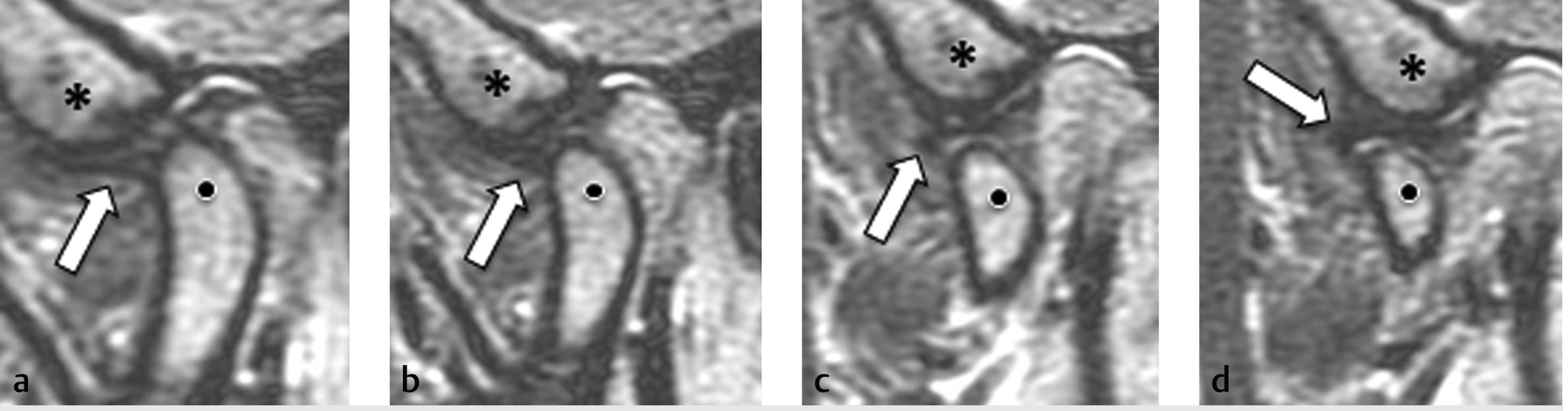
High-resolution proton-density MRI of a cadaveric TMJ in the open-mouth position. The articular disc (arrows) translates anteriorly as the condyle (dots) moves forward under the articular eminence (*). Panels a-d show progressive opening. Note the retrodiscal layers separating as the mouth opens.
3. UTE MRI - Condylar Fibrocartilage & Bone (Imaging Anatomy Atlas)
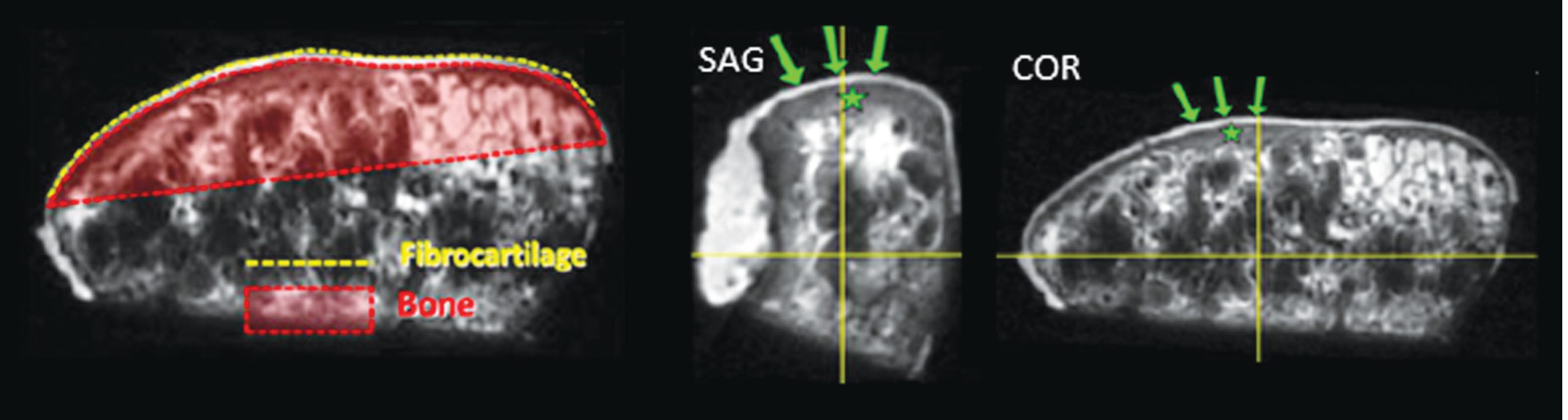
3D ultrashort time-to-echo (UTE) MRI of the harvested condyle in sagittal (SAG) and coronal (COR) planes. Green arrows point to the fibrocartilage surface of the condyle; the red-shaded zone = bone; yellow dashed = bone-cartilage interface. This confirms that TMJ articular surfaces are fibrocartilage, not hyaline cartilage.
This is a shared conversation. Sign in to Orris to start your own chat.