Explain fibroadenoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
fibroadenoma breast
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Here is the complete explanation:
Fibroadenoma
Definition and Overview
A fibroadenoma is the most common benign tumor of the female breast and the most common cause of a breast lump in women aged 15-25 years. It is a fibroepithelial tumor - meaning it contains both stromal (fibrous) and epithelial (glandular) elements, both derived from the intralobular stroma and associated ducts of the breast lobule.
- Robbins Pathologic Basis of Disease, p. 984
- Bailey & Love's Short Practice of Surgery (28th ed.), p. 408
Pathogenesis and Molecular Biology
Fibroadenomas arise from hyperplasia of a single lobule under the influence of female sex hormones. At the molecular level:
- ~Two-thirds harbor driver mutations in MED12, a gene encoding a subunit of the mediator complex that regulates RNA polymerase II-dependent transcription. The same mutation is strongly associated with uterine leiomyoma - another stromal tumor in a hormone-responsive organ.
- ~One-third harbor mutations in RARA (retinoic acid receptor alpha), an estrogen target gene that cooperates with the estrogen receptor in regulating transcription.
These mutations likely derange sex hormone-regulated gene expression, promoting stromal cell proliferation and survival. - Robbins, p. 984
Epidemiology
| Feature | Detail |
|---|---|
| Peak age | 20s-30s (teens to early reproductive years) |
| Rarely new after | Age 40-45 |
| Common presentation | Palpable lump or mammographic density |
| Multiplicity | Frequently multiple and bilateral |
| Sex | Almost exclusively female |
Sabiston Textbook of Surgery, p. 1384
Histological Types
Two classical patterns are recognized based on the relationship of stroma to ducts:
1. Pericanalicular Fibroadenoma
- Fibrous tissue surrounds small, round, patent tubular glands
- Relatively smaller and harder
- Seen in younger women (15-30 years)
2. Intracanalicular Fibroadenoma
- Proliferating stroma compresses and distorts ductal elements into elongated, cleft-like, spidery spaces
- Relatively larger and softer
- Seen in middle-aged women (35-50 years)
In practice, both patterns often coexist within the same tumor. - S. Das Manual on Clinical Surgery (13th ed.), p. 434
Morphology
Gross:
- Well-circumscribed, rubbery, gray-white nodule
- Sharply demarcated from surrounding tissue, bulging above it on cut surface
- Contains slit-like spaces (particularly in the intracanalicular pattern)
- Usually 2-3 cm; can range from <1 cm to very large
Microscopic:
- Delicate, often myxoid stroma resembling normal intralobular stroma
- In older women, stroma becomes densely hyalinized and epithelium atrophic
Robbins, p. 984
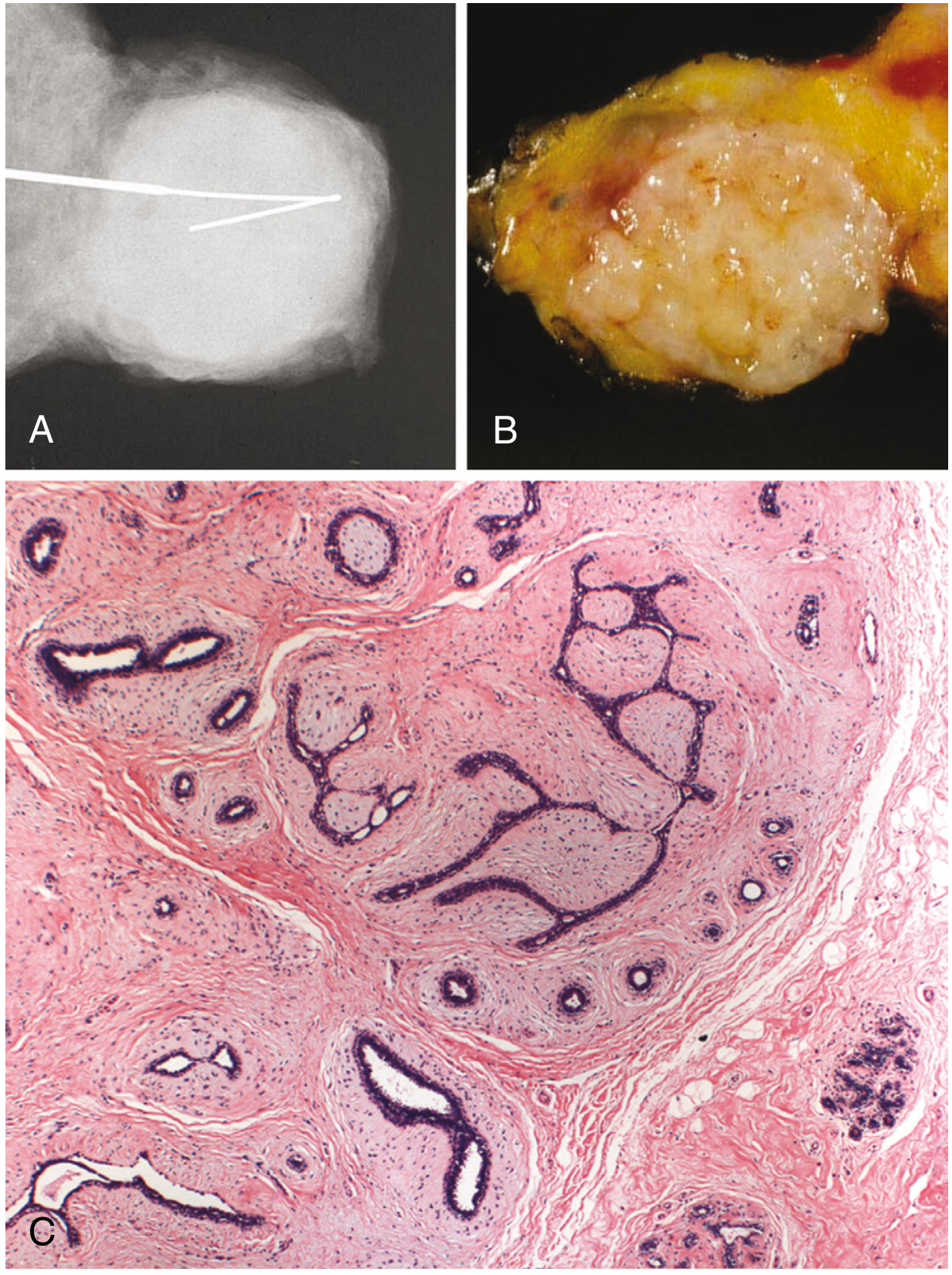
The image below (from Robbins) shows: (A) mammographic appearance as a well-circumscribed mass, (B) gross specimen - rubbery, white, well-encapsulated, (C) histology demonstrating proliferating intralobular stroma surrounding/distorting epithelial elements, with a sharp border from surrounding tissue.
Clinical Features
- Presentation: Painless, smooth, firm, well-defined, highly mobile lump - classically described as a "breast mouse" or "floating tumour" because it slides freely under the examining fingers with no tethering or fixation to skin or deep structures. (S. Das, p. 434)
- No axillary lymphadenopathy
- Hormonally responsive: May enlarge during pregnancy (sometimes rapidly, even undergoing infarction - mimicking carcinoma) and tend to regress after menopause
- Cyclosporin A association: Almost half of renal transplant patients on cyclosporin A develop multiple bilateral fibroadenomas, which regress after stopping the drug
Subtypes
| Subtype | Definition | Management |
|---|---|---|
| Simple fibroadenoma | Standard; <5 cm | Observation if typical features |
| Giant fibroadenoma | >5 cm in size | Surgical excision recommended |
| Juvenile fibroadenoma | Large, cellular, in adolescents/young adults | Observe if <5 cm; excise if >5 cm, growing, or persists to adulthood |
| Complex fibroadenoma | Contains cysts >0.3 cm, sclerosing adenosis, epithelial calcifications, or papillary apocrine change | Slightly increased cancer risk |
| Myxoid fibroadenoma | Prominent myxoid stroma; may be sporadic or associated with Carney complex (PRKAR1A germline mutation) | Consider genetic evaluation |
Sabiston, p. 1385; Robbins, p. 984
Cancer Risk
Fibroadenomas are not directly premalignant, but risk varies by type:
| Type | Relative Risk (RR) of Breast Cancer |
|---|---|
| Simple fibroadenoma | 1.5-1.7 |
| Complex fibroadenoma | 3.4-3.7 (with epithelial hyperplasia) |
| Complex fibroadenoma + family history | 3.0-4.0 (especially lobular carcinoma) |
Cancer arising within a newly discovered fibroadenoma is exceedingly rare (~0.2%). Complex fibroadenomas likely increase risk because they are associated with "at-risk" lesions in the surrounding breast tissue (e.g., atypical hyperplasia) rather than the fibroadenoma itself being the direct driver. - Bailey & Love, p. 414-415; Robbins, p. 984
Diagnosis
- Clinical: Smooth, mobile, firm mass - especially in a young woman
- Ultrasound: Preferred imaging; distinguishes solid (fibroadenoma) from cystic lesion. Typical features: well-circumscribed, oval, homogeneous hypoechoic mass
- Mammography: Shows a radiopaque, well-circumscribed density; less helpful than ultrasound for distinguishing cysts vs. fibroadenomas. In older women, calcifications may appear
- Triple assessment (clinical + imaging + cytology/biopsy) is the standard approach
- Biopsy is indicated if the patient is >25, features are atypical on US, or there is clinical suspicion
Management
Conservative (observation):
- Young women (<25 years) with clinically and sonographically typical fibroadenoma
- Tissue diagnosis confirming fibroadenoma - patient can be reassured; excision not mandatory
Surgical excision is indicated for:
- Age >30 years
- Suspicious imaging features (e.g., microlobulation)
- Atypia on histology
- Size >5 cm (giant fibroadenoma)
- Family history of breast cancer
- Rapid growth (to exclude phyllodes tumor)
- Histological difficulty distinguishing from phyllodes tumor (especially >3 cm or rapidly growing)
- Patient preference
Medical: Regression has been observed with antiestrogens (tamoxifen, ormeloxifene).
Minimally invasive options:
- Percutaneous excision (vacuum-assisted device) for smaller masses
- Cryoablation - a 2025 systematic review (PMID 41061430) confirms it as a safe, effective option for benign fibroadenomas, with good cosmetic outcomes
In elderly patients: Excision should include a rim of normal tissue, as lesions may harbor malignancy or a phyllodes tumour. - Bailey & Love, p. 419-423; Sabiston, p. 1384
Fibroadenoma vs. Phyllodes Tumor
This is the key differential diagnosis clinically and histologically:
| Feature | Fibroadenoma | Phyllodes Tumor |
|---|---|---|
| Age | Teens-30s | Usually >30 years |
| Growth | Slow | Can be rapid |
| Size | Usually 2-3 cm | Often larger, can be massive |
| Stroma cellularity | Low | High, with mitotic activity |
| MED12/RARA mutations | Present (~two-thirds) | Also present, plus TERT, TP53, RB |
| Malignant potential | Nil (benign) | Borderline or malignant forms exist |
| Margins | Sharp | Infiltrating in malignant forms |
| Management | Enucleation or observation | Wide local excision with 2-cm margin |
A 2026 meta-analysis (PMID 41979873) specifically examined histological features that distinguish phyllodes tumor from fibroadenoma on core needle biopsy, reflecting ongoing clinical relevance of this distinction.
Summary in one sentence: Fibroadenoma is a benign, hormonally responsive fibroepithelial breast tumor, most common in young women, presenting as a smooth, mobile "breast mouse," driven by MED12 mutations, and managed conservatively in typical cases with surgical excision reserved for atypical, large, or rapidly growing lesions.
This is a shared conversation. Sign in to Orris to start your own chat.