Treatment of status epilepticys
Reading File
Finding Sources
Searching PubMed
"status epilepticus" AND treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Treatment of Status Epilepticus
Definition
Status epilepticus (SE) is defined as:
- A single seizure lasting ≥5 minutes, OR
- Two or more seizures without recovery of consciousness between them
The 5-minute threshold is used because after this point, seizures are less likely to terminate spontaneously, less responsive to antiepileptic drugs, and more likely to cause neuronal damage. Treatment must begin at this point - don't wait for 30 minutes.
Common Causes
Subtherapeutic antiepileptic drug levels, acute stroke, anoxia/hypoxia, CNS infection, metabolic abnormalities, alcohol/drug withdrawal, autoimmune encephalitis (a leading cause in recent data).
Immediate Stabilization (0-5 minutes)
Before any anticonvulsant:
- Airway, Breathing, Circulation (ABCs) - position patient, suction, oxygen
- Large-bore IV access (or IO if IV unavailable)
- Bedside glucose - correct hypoglycemia immediately
- Monitor: cardiac, pulse oximetry, end-tidal CO2
- Thiamine 100 mg IV before glucose in adults at risk for deficiency
- Labs: electrolytes, glucose, calcium, magnesium, CBC, renal/liver function, AED levels, toxicology
Staged Pharmacological Treatment
Phase 1 - First-Line: Benzodiazepines (0-10 min)
Benzodiazepines terminate SE in ~70% of cases. They act by enhancing GABA-A receptor activity.
| Drug | Route | Dose | Notes |
|---|---|---|---|
| Lorazepam | IV | 0.1 mg/kg at 2 mg/min (typically 4 mg) | Preferred IV agent - longer CNS duration than diazepam due to less peripheral redistribution |
| Diazepam | IV | 5-10 mg bolus at 5 mg/min | Rapid CNS entry but short effective duration due to redistribution into fat |
| Midazolam | IM | 10 mg | First choice if IV not available; RAMPART trial showed IM midazolam = IV lorazepam |
| Diazepam | Rectal | 0.2-0.5 mg/kg | Prehospital/pediatric use |
| Midazolam | Intranasal/buccal | Weight-based | Acceptable prehospital alternatives |
- If seizure persists 5 minutes after the first dose, give a second benzodiazepine dose
- A third dose may be given before escalating to second-line agents
Watch for: respiratory depression, hypotension, impaired consciousness.
Phase 2 - Second-Line: Established SE (10-30 min)
If benzodiazepines fail, load one of the following. All three have equivalent efficacy (~45-50% seizure cessation) per the ESETT trial:
| Drug | Dose | Rate | Notes |
|---|---|---|---|
| Fosphenytoin | 20 mg PE/kg IV | 150 mg PE/min | Water-soluble phenytoin prodrug; can be given IM; less cardiotoxic and less sclerosing than phenytoin; preferred over phenytoin |
| Phenytoin | 20 mg/kg IV | ≤50 mg/min | Requires cardiac monitoring (hypotension, arrhythmias); incompatible with glucose solutions |
| Levetiracetam | 30-60 mg/kg (2,000-4,500 mg) IV | Over 10-15 min | Excellent safety profile; no hepatic/cardiac concerns; increasingly favored |
| Valproic acid | 30-40 mg/kg IV | 5 mg/kg/min | Avoid in liver disease, thrombocytopenia, or suspected metabolic disease; do NOT use in children <2 years |
| Lacosamide | 200-400 mg IV | Slower infusion | ECG monitoring needed (PR prolongation risk) |
| Phenobarbital | 10-20 mg/kg IV | 50-100 mg/min | Highly effective but causes prolonged sedation, respiratory depression, and hypotension |
A 2024 network meta-analysis (Kishihara et al., PMID 38941904) evaluated second-line agents in adult SE. No agent was clearly superior to the others, consistent with the ESETT trial findings.
Phase 3 - Refractory Status Epilepticus (>30-60 min)
Defined as SE persisting despite adequate doses of two antiepileptic agents. Requires ICU admission, intubation, continuous EEG monitoring.
Use continuous IV infusion of an anesthetic agent:
| Agent | Loading Dose | Infusion Rate |
|---|---|---|
| Midazolam | 0.2 mg/kg IV | 0.05-2 mg/kg/h |
| Propofol | 1-2 mg/kg IV | 1-10 mg/kg/h (watch for propofol infusion syndrome with prolonged use) |
| Pentobarbital | 5 mg/kg IV | 0.5-3 mg/kg/h |
| Ketamine | 1.5-4.5 mg/kg IV | 2.2-5 mg/kg/h (NMDA antagonist; useful as GABA receptors are internalized) |
| Thiopental | 3-5 mg/kg IV | Titrated |
- EEG goal: burst suppression pattern
- A 2024 systematic review and meta-analysis (Chiriboga et al., PMID 38881333) specifically supports ketamine in pediatric refractory SE
Phase 4 - Super-Refractory Status Epilepticus (>24 hours on anesthesia)
Options with limited but growing evidence:
- Ketogenic diet (via NG tube)
- Immunotherapy (steroids, IVIG, plasmapheresis) - especially if autoimmune cause suspected
- Electroconvulsive therapy (ECT) - has shown benefit in some case series
- Hypothermia, magnesium sulfate (especially eclampsia)
- Transcranial magnetic stimulation (TMS) - experimental
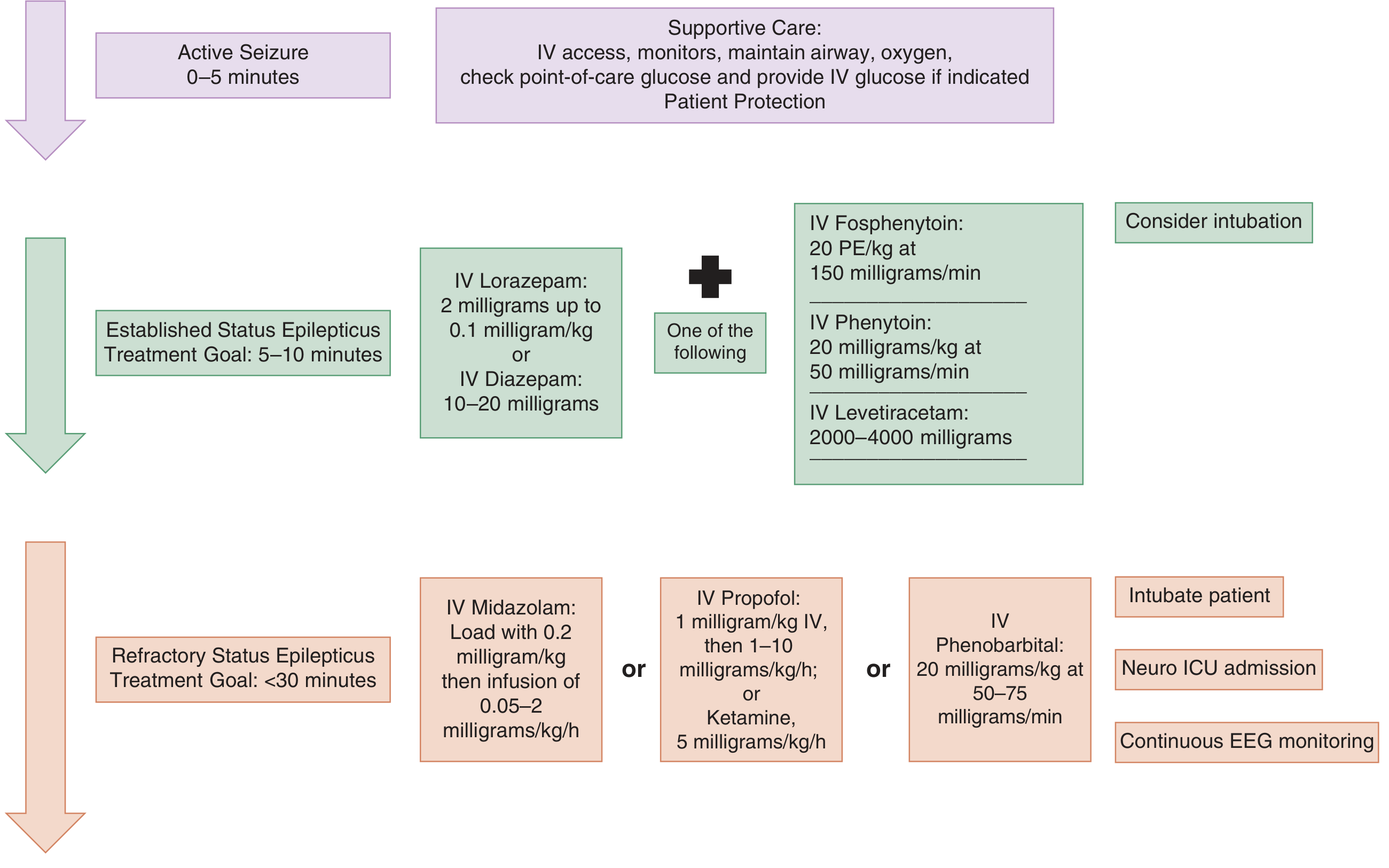
Treatment Algorithm (Tintinalli's EM)
Nonconvulsive Status Epilepticus (NCSE)
- Presents as coma, fluctuating mental status, subtle twitching, or unexplained confusion - NO overt convulsions
- Diagnosis requires EEG
- Treatment is the same staged approach but can be started more cautiously with lower initial doses since there is less urgency
- Prolonged postictal period or failure to wake after a convulsive seizure should prompt EEG to rule out NCSE
Key Pathophysiology Note
After 5-20 minutes of SE, GABA-A receptors are internalized (reducing the efficacy of benzodiazepines), while NMDA/glutamate receptors are upcharged. This explains why:
- Benzodiazepines lose effectiveness over time
- Ketamine (NMDA antagonist) becomes more rational in later stages
- The blood-brain barrier is compromised, allowing hyperexcitatory chemicals to flood the CNS
Intubation
Consider early in established SE. If intubating:
- Use a short-acting neuromuscular blocker (e.g., succinylcholine) to allow detection of ongoing seizure activity
- Choose induction agents with antiepileptic properties: propofol or ketamine
- Arrange continuous EEG monitoring after paralysis
Sources: Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Katzung's Basic & Clinical Pharmacology 16e; Goldman-Cecil Medicine; Katzung (Katzung's Basic and Clinical Pharmacology, 16th Edition, p. 677)
This is a shared conversation. Sign in to Orris to start your own chat.