I need the differences between various generations of da vinci robots used in robotic suregry and their images as well
da Vinci surgical robot generations comparison differences S Si Xi SP
da Vinci robot generations history 1999 2006 2009 2014 2018 2024 specifications
https://headneckroboticsurgery.com/2023/05/06/da-vinci-gener…
da Vinci 5 robot 2024 features specifications vs Xi differences
Da Vinci Surgical Robot Generations - Complete Guide

1st Generation - da Vinci Standard (1999/2000)
- 3-arm system (a 4th arm added in 2003)
- Four arms mounted on the sides of a central column; one fixed camera arm
- Stereoscopic 3D viewer built into the surgeon's console (binocular viewer, not a flat screen)
- Motorized wrist instruments (EndoWrist) with 7 degrees of freedom - mimicking human wrist motion
- Heavy camera arm with counterweights (the original dual-optic endoscopes were large)
- All computing housed in the surgeon's console
- No HD vision, no fluorescence imaging
2nd Generation - da Vinci S (2006)
- Introduced 3D high-definition (HD) vision - a major leap in image quality
- Lighter, more streamlined patient-side cart, though same basic 4-arm-on-column design
- Simplified setup with interactive touchscreen
- Improved software and hardware architecture
- Autofocus camera systems (the long central focus pedal was no longer required)
- Faster docking than the original
3rd Generation - da Vinci Si (2009)
- Dual console capability - a second surgeon console can connect, enabling proctored surgery and training side-by-side (transformative for surgical education)
- Brain of the system moved from the surgeon's console to the vision cart - simplified the console design and enabled future upgrades
- Communication between system components reduced to just two fiber optic cables
- Touchscreen interface added to the arm rest for system configuration
- TilePro software - allowed display of multiple video inputs simultaneously (e.g., ultrasound + endoscope view)
- Real-time fluorescence imaging (near-infrared) introduced
- Sleeker console appearance
4th Generation - da Vinci Xi (2014)
- Completely new patient-side cart with a boom-mounted overhead architecture - arms suspended above the surgical field from a horizontal boom, not a central column
- Any arm can hold the camera (numbered 1-4) - no dedicated fixed camera arm; all instruments and camera are 8mm
- Laser-guided port positioning system for precise setup
- Arms are thinner, smaller, with redesigned joints - greater range of motion and compacted spacing (one fist-width between arms vs. widely spaced)
- 360-degree rotation capability - can dock from any angle and work in any abdominal quadrant without re-docking
- Shorter docking time (~9.5 min vs ~19 min for Si in studies)
- Improved EndoWrist instruments with greater workspace
- Integrated table motion (patient positioning during surgery without undocking)
- Vessel Sealer Extend - seals and cuts vessels up to 7mm diameter
- Redesigned fully reusable stainless steel cannulas
- Firefly fluorescence imaging integrated
- Submillimetric accuracy (FLE ~0.97 mm vs 1.64 mm for Si)
Da Vinci X (2017) - The "Hybrid"
Da Vinci SP - Single Port (2018/2019)
- Single arm delivers three multi-jointed instruments plus a fully articulating 3D HD endoscope - all through one cannula
- Instruments first diverge inside the patient, then re-converge at the target
- Designed for single-incision or natural orifice surgery (e.g., through the mouth, vagina, or urethra)
- Ideal for confined anatomical spaces (neck, pelvis, retroauricular approaches)
- Smaller footprint
5th Generation - da Vinci 5 (2024)

- 10,000x more computing power than Xi - enables AI-driven features, advanced data analytics, and future capabilities
- Force Feedback technology - sensors measure pressure exerted on tissue during surgery; surgeon feels haptic resistance in their hands (can be toggled on/off). This is the biggest advance surgeons are most excited about.
- Redesigned hand controllers - ergonomic curved haptic arms with more volume for electronics; improved tremor and vibration filtration
- ~2x faster docking compared to Xi
- Over 150 design innovations
- Same boom architecture as Xi externally, but major internal redesign of arms (additional sensors, smarter electronics under the skin)
- Improved 3D imaging and vision
- Smaller OR footprint
- Integrated with My Intuitive+ app (case insights, surgical video review, personalized training), SimNow VR simulator, and Intuitive Hub (edge computing)
- Universal user interface across all three system components
- Guided tool changes and task automation reduce reliance on OR staff
- Note: Cleared for same indications as Xi, except cardiac and pediatric procedures (as of 2024)
Quick Comparison Summary Table
| Feature | Standard (1999) | S (2006) | Si (2009) | Xi (2014) | SP (2018) | da Vinci 5 (2024) |
|---|---|---|---|---|---|---|
| Arms | 3 (then 4) | 4 | 4 | 4 | 1 (3 instruments) | 4 |
| Camera | Fixed arm | Fixed arm | Fixed arm | Any arm | Integrated | Any arm |
| Vision | Standard 3D | HD 3D | HD 3D + TilePro | HD 3D + Firefly | 3D HD articulating | Next-gen 3D improved |
| Dual Console | No | No | Yes | Yes | No | Yes |
| Force Feedback | No | No | No | No | No | Yes |
| Docking | Slow | Moderate | Slow (~19 min) | Fast (~9.5 min) | N/A | ~2x faster than Xi |
| Table Motion | No | No | No | Yes | No | Yes (integrated) |
| Fluorescence | No | No | Yes (basic) | Yes (Firefly) | Yes | Yes (enhanced) |
| Computing | Basic | Basic | Moderate | Moderate | Moderate | 10,000x vs Xi |
| Single Port | No | No | No | No | Yes | No |
| Cart Design | Column | Column | Column | Overhead boom | Single arm | Overhead boom |
Create a PDF comparison guide of all da Vinci generations
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not found"
mkdir -p /home/daytona/workspace/davinci-guide && echo "Created"
~/davinci-guide/create_pdf.py
#!/usr/bin/env python3
"""
Da Vinci Surgical Robot Generations - PDF Comparison Guide
"""
import json
import subprocess
import base64
import os
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import cm, mm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
PageBreak, HRFlowable, Image, KeepTogether
)
from reportlab.platypus.flowables import Flowable
from reportlab.pdfgen import canvas
from io import BytesIO
# ── Color Palette ──────────────────────────────────────────────────────────────
DARK_BLUE = colors.HexColor("#0B2545") # header / title bg
MID_BLUE = colors.HexColor("#1B4F8A") # section heading bg
LIGHT_BLUE = colors.HexColor("#D6E4F0") # alternating table row
ACCENT = colors.HexColor("#2980B9") # thin rule / bullet accent
WHITE = colors.white
LIGHT_GREY = colors.HexColor("#F4F6F9")
TEXT_DARK = colors.HexColor("#1A1A2E")
GOLD = colors.HexColor("#F0A500")
OUTPUT_PATH = "/home/daytona/workspace/davinci-guide/DaVinci_Generations_Guide.pdf"
PAGE_W, PAGE_H = A4
# ── Image downloading helper ───────────────────────────────────────────────────
def fetch_images(urls):
try:
result = subprocess.check_output(
["node", "/home/daytona/skills/shared/scripts/fetch_images.js"] + urls,
timeout=30
)
return json.loads(result)
except Exception as e:
print(f"Image fetch error: {e}")
return [{"url": u, "base64": None, "error": str(e)} for u in urls]
def b64_to_image_flowable(b64_str, max_width, max_height):
"""Convert base64 image string to a ReportLab Image flowable."""
try:
raw = base64.b64decode(b64_str.split(",")[1])
buf = BytesIO(raw)
img = Image(buf, width=max_width, height=max_height, kind='proportional')
return img
except Exception as e:
print(f"Image conversion error: {e}")
return None
# ── Canvas background for header pages ────────────────────────────────────────
class HeaderCanvas(canvas.Canvas):
def __init__(self, *args, **kwargs):
canvas.Canvas.__init__(self, *args, **kwargs)
self._saved_page_states = []
def showPage(self):
self._saved_page_states.append(dict(self.__dict__))
self._startPage()
def save(self):
num_pages = len(self._saved_page_states)
for state in self._saved_page_states:
self.__dict__.update(state)
self.draw_page_decorations(num_pages)
canvas.Canvas.showPage(self)
canvas.Canvas.save(self)
def draw_page_decorations(self, total_pages):
page_num = self._saved_page_states.index(dict(self.__dict__)) + 1 if dict(self.__dict__) in self._saved_page_states else 1
# Bottom footer bar
self.setFillColor(DARK_BLUE)
self.rect(0, 0, PAGE_W, 1.2*cm, fill=1, stroke=0)
self.setFillColor(WHITE)
self.setFont("Helvetica", 8)
self.drawString(2*cm, 0.4*cm, "Da Vinci Surgical Robot Generations | Intuitive Surgical")
self.drawRightString(PAGE_W - 2*cm, 0.4*cm, f"Page {self._pageNumber} of {total_pages}")
# Top thin accent line
self.setStrokeColor(ACCENT)
self.setLineWidth(2)
self.line(0, PAGE_H - 0.5*cm, PAGE_W, PAGE_H - 0.5*cm)
# ── Styles ─────────────────────────────────────────────────────────────────────
def make_styles():
base = getSampleStyleSheet()
styles = {}
styles['cover_title'] = ParagraphStyle(
'cover_title', fontName='Helvetica-Bold', fontSize=34,
textColor=WHITE, alignment=TA_CENTER, leading=42, spaceAfter=8
)
styles['cover_sub'] = ParagraphStyle(
'cover_sub', fontName='Helvetica', fontSize=14,
textColor=LIGHT_BLUE, alignment=TA_CENTER, leading=20, spaceAfter=4
)
styles['cover_year'] = ParagraphStyle(
'cover_year', fontName='Helvetica-Bold', fontSize=12,
textColor=GOLD, alignment=TA_CENTER, leading=16
)
styles['section_title'] = ParagraphStyle(
'section_title', fontName='Helvetica-Bold', fontSize=17,
textColor=WHITE, alignment=TA_LEFT, leading=22, leftIndent=0
)
styles['gen_header'] = ParagraphStyle(
'gen_header', fontName='Helvetica-Bold', fontSize=13,
textColor=WHITE, alignment=TA_LEFT, leading=18
)
styles['body'] = ParagraphStyle(
'body', fontName='Helvetica', fontSize=10,
textColor=TEXT_DARK, alignment=TA_JUSTIFY, leading=15, spaceAfter=4
)
styles['bullet'] = ParagraphStyle(
'bullet', fontName='Helvetica', fontSize=9.5,
textColor=TEXT_DARK, leftIndent=14, bulletIndent=4,
leading=14, spaceAfter=2
)
styles['bold_label'] = ParagraphStyle(
'bold_label', fontName='Helvetica-Bold', fontSize=10,
textColor=MID_BLUE, leading=14, spaceAfter=2
)
styles['table_header'] = ParagraphStyle(
'table_header', fontName='Helvetica-Bold', fontSize=9,
textColor=WHITE, alignment=TA_CENTER, leading=12
)
styles['table_cell'] = ParagraphStyle(
'table_cell', fontName='Helvetica', fontSize=8.5,
textColor=TEXT_DARK, alignment=TA_CENTER, leading=12
)
styles['table_cell_left'] = ParagraphStyle(
'table_cell_left', fontName='Helvetica', fontSize=8.5,
textColor=TEXT_DARK, alignment=TA_LEFT, leading=12
)
styles['caption'] = ParagraphStyle(
'caption', fontName='Helvetica-Oblique', fontSize=8,
textColor=colors.grey, alignment=TA_CENTER, leading=11
)
styles['toc_entry'] = ParagraphStyle(
'toc_entry', fontName='Helvetica', fontSize=11,
textColor=TEXT_DARK, leading=20, leftIndent=20
)
return styles
# ── Cover page ─────────────────────────────────────────────────────────────────
def build_cover(styles):
story = []
# Dark header band
cover_data = [[Paragraph("DA VINCI<br/>SURGICAL ROBOT", styles['cover_title'])]]
cover_table = Table(cover_data, colWidths=[PAGE_W - 4*cm])
cover_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), DARK_BLUE),
('TOPPADDING', (0,0), (-1,-1), 2*cm),
('BOTTOMPADDING', (0,0), (-1,-1), 1.5*cm),
('LEFTPADDING', (0,0), (-1,-1), 1*cm),
('RIGHTPADDING', (0,0), (-1,-1), 1*cm),
]))
story.append(cover_table)
story.append(Spacer(1, 0.5*cm))
# Subtitle band
sub_data = [[Paragraph("GENERATIONS COMPARISON GUIDE", styles['cover_sub'])]]
sub_table = Table(sub_data, colWidths=[PAGE_W - 4*cm])
sub_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), MID_BLUE),
('TOPPADDING', (0,0), (-1,-1), 0.7*cm),
('BOTTOMPADDING', (0,0), (-1,-1), 0.7*cm),
]))
story.append(sub_table)
story.append(Spacer(1, 0.8*cm))
# Year badge
story.append(Paragraph("1999 - 2024", styles['cover_year']))
story.append(Spacer(1, 0.4*cm))
# Timeline visual as table
timeline = [
["1999", "2006", "2009", "2014", "2017/18", "2024"],
["Standard", "S", "Si", "Xi", "X / SP", "5"],
["1st Gen", "2nd Gen", "3rd Gen", "4th Gen", "Variants", "5th Gen"],
]
col_w = (PAGE_W - 4*cm) / 6
tl_table = Table(timeline, colWidths=[col_w]*6, rowHeights=[1.0*cm, 0.9*cm, 0.7*cm])
tl_table.setStyle(TableStyle([
# Year row
('BACKGROUND', (0,0), (-1,0), MID_BLUE),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,0), 11),
('ALIGN', (0,0), (-1,0), 'CENTER'),
('VALIGN', (0,0), (-1,0), 'MIDDLE'),
# Name row
('BACKGROUND', (0,1), (-1,1), LIGHT_BLUE),
('TEXTCOLOR', (0,1), (-1,1), DARK_BLUE),
('FONTNAME', (0,1), (-1,1), 'Helvetica-Bold'),
('FONTSIZE', (0,1), (-1,1), 13),
('ALIGN', (0,1), (-1,1), 'CENTER'),
('VALIGN', (0,1), (-1,1), 'MIDDLE'),
# Gen row
('BACKGROUND', (0,2), (-1,2), LIGHT_GREY),
('TEXTCOLOR', (0,2), (-1,2), colors.grey),
('FONTNAME', (0,2), (-1,2), 'Helvetica-Oblique'),
('FONTSIZE', (0,2), (-1,2), 8),
('ALIGN', (0,2), (-1,2), 'CENTER'),
('VALIGN', (0,2), (-1,2), 'MIDDLE'),
('GRID', (0,0), (-1,-1), 0.5, WHITE),
('BOX', (0,0), (-1,-1), 1.5, ACCENT),
]))
story.append(tl_table)
story.append(Spacer(1, 1.0*cm))
# Cover summary paragraph
cover_text = (
"Since its FDA clearance in July 2000, the da Vinci Surgical System by Intuitive Surgical "
"has transformed minimally invasive surgery. Each generation has brought meaningful advances "
"in vision, instrumentation, arm design, ergonomics, and data integration. This guide "
"compares every platform - from the original da Vinci Standard to the latest da Vinci 5 - "
"covering key specifications, clinical improvements, and the most important differences "
"surgeons and hospitals need to know."
)
story.append(Paragraph(cover_text, styles['body']))
story.append(Spacer(1, 0.8*cm))
# Published by
pub_data = [[
Paragraph("Compiled from Intuitive Surgical data, peer-reviewed literature, and clinical sources.", styles['caption']),
]]
pub_table = Table(pub_data, colWidths=[PAGE_W - 4*cm])
pub_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), LIGHT_GREY),
('TOPPADDING', (0,0), (-1,-1), 0.5*cm),
('BOTTOMPADDING', (0,0), (-1,-1), 0.5*cm),
('BOX', (0,0), (-1,-1), 1, ACCENT),
]))
story.append(pub_table)
story.append(PageBreak())
return story
# ── TOC ────────────────────────────────────────────────────────────────────────
def build_toc(styles):
story = []
toc_header = [[Paragraph("TABLE OF CONTENTS", styles['section_title'])]]
toc_table = Table(toc_header, colWidths=[PAGE_W - 4*cm])
toc_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), DARK_BLUE),
('TOPPADDING', (0,0), (-1,-1), 0.6*cm),
('BOTTOMPADDING', (0,0), (-1,-1), 0.6*cm),
('LEFTPADDING', (0,0), (-1,-1), 0.8*cm),
]))
story.append(toc_table)
story.append(Spacer(1, 0.6*cm))
entries = [
("1.", "Da Vinci Standard (1999) - 1st Generation"),
("2.", "Da Vinci S (2006) - 2nd Generation"),
("3.", "Da Vinci Si (2009) - 3rd Generation"),
("4.", "Da Vinci Xi (2014) - 4th Generation"),
("5.", "Da Vinci X (2017) - Budget Hybrid"),
("6.", "Da Vinci SP (2018) - Single Port"),
("7.", "Da Vinci 5 (2024) - 5th Generation"),
("8.", "Full Comparison Table - All Generations"),
("9.", "Summary & Key Takeaways"),
]
for num, title in entries:
row = [[
Paragraph(f"<b>{num}</b>", styles['bold_label']),
Paragraph(title, styles['toc_entry']),
]]
row_table = Table(row, colWidths=[1.2*cm, PAGE_W - 5.2*cm])
row_table.setStyle(TableStyle([
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('LINEBELOW', (0,0), (-1,-1), 0.3, colors.HexColor("#CCCCCC")),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
]))
story.append(row_table)
story.append(PageBreak())
return story
# ── Section header band ────────────────────────────────────────────────────────
def section_header(title, year, gen_label, styles):
"""Returns a styled generation header table."""
header_data = [[
Paragraph(f"{title}", styles['section_title']),
Paragraph(f"<b>{year}</b><br/><font size='9'>{gen_label}</font>", ParagraphStyle(
'year_label', fontName='Helvetica-Bold', fontSize=13,
textColor=GOLD, alignment=TA_CENTER, leading=16
)),
]]
ht = Table(header_data, colWidths=[PAGE_W - 8*cm, 4*cm])
ht.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), DARK_BLUE),
('LEFTPADDING', (0,0), (0,-1), 0.8*cm),
('RIGHTPADDING', (-1,0), (-1,-1), 0.6*cm),
('TOPPADDING', (0,0), (-1,-1), 0.6*cm),
('BOTTOMPADDING', (0,0), (-1,-1), 0.6*cm),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
]))
return ht
def specs_table(rows, styles):
"""Build a two-column spec table (Label | Value)."""
table_data = []
for label, value in rows:
table_data.append([
Paragraph(f"<b>{label}</b>", styles['bold_label']),
Paragraph(value, styles['body']),
])
t = Table(table_data, colWidths=[5.5*cm, PAGE_W - 9.5*cm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), WHITE),
('ROWBACKGROUNDS', (0,0), (-1,-1), [WHITE, LIGHT_GREY]),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 8),
('RIGHTPADDING', (0,0), (-1,-1), 8),
('LINEBELOW', (0,0), (-1,-1), 0.3, colors.HexColor("#DDDDDD")),
('BOX', (0,0), (-1,-1), 0.8, ACCENT),
]))
return t
def bullet_list(items, styles):
out = []
for item in items:
out.append(Paragraph(f"<bullet color='#{ACCENT.hexval()[2:]}'>●</bullet> {item}", styles['bullet']))
return out
# ── Generation pages ───────────────────────────────────────────────────────────
def gen_standard(styles):
story = []
story.append(section_header("DA VINCI STANDARD", "1999 / 2000", "1st Generation", styles))
story.append(Spacer(1, 0.5*cm))
story.append(Paragraph(
"The original da Vinci Surgical System received FDA clearance in July 2000, marking the "
"beginning of commercial robotic surgery. It was the first system to translate a surgeon's "
"hand movements into precise micro-movements of instruments inside the patient, through a "
"stereoscopic 3D viewer at the surgeon's console.",
styles['body']
))
story.append(Spacer(1, 0.4*cm))
story.append(specs_table([
("FDA Clearance", "July 2000"),
("Arms", "3 (4th instrument arm added 2003)"),
("Camera", "Fixed dedicated camera arm"),
("Vision", "Standard 3D stereoscopic (non-HD)"),
("Degrees of Freedom", "7 DoF + 2 axial rotation per instrument"),
("Console", "Binocular viewer; computing housed in console"),
("Dual Console", "No"),
("Force Feedback", "No"),
("Fluorescence Imaging", "No"),
("HD Vision", "No"),
("Table Motion", "No"),
("Docking", "Slow; complex setup"),
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Key Features & Innovations:</b>", styles['bold_label']))
story.extend(bullet_list([
"First commercially available robotic surgery platform (Intuitive Surgical)",
"EndoWrist instruments with 7 degrees of freedom - mimicking human wrist motion and eliminating tremor",
"Immersive stereoscopic 3D binocular viewer at surgeon console (not a flat monitor)",
"All robotic arms originating from a single patient cart (no per-arm table mounting)",
"Surgeon seated at console, fully decoupled from the patient",
"Heavy camera arm requiring counterweights due to large dual-optic endoscopes",
"Long central pedal on foot board for manual camera focus",
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Limitations:</b>", styles['bold_label']))
story.extend(bullet_list([
"No high-definition imaging",
"Bulky footprint and long OR setup times",
"Limited arm flexibility; arms required wide spacing",
"No dual-console capability (no teaching/proctoring setup)",
"Single console only; all computing in console",
"No fluorescence or near-infrared imaging",
], styles))
story.append(PageBreak())
return story
def gen_s(styles):
story = []
story.append(section_header("DA VINCI S", "2006", "2nd Generation", styles))
story.append(Spacer(1, 0.5*cm))
story.append(Paragraph(
"Launched in 2006, the da Vinci S was a significant hardware and software upgrade. "
"The most impactful improvement was the introduction of 3D high-definition vision, which "
"dramatically improved the surgeon's ability to see fine tissue planes and structures. "
"The patient-side cart was redesigned to be lighter and more streamlined.",
styles['body']
))
story.append(Spacer(1, 0.4*cm))
story.append(specs_table([
("FDA Clearance", "2006"),
("Arms", "4 (column-mounted)"),
("Camera", "Fixed dedicated camera arm"),
("Vision", "3D High-Definition (HD) - major upgrade"),
("Console", "Binocular viewer; similar pedal board to Standard"),
("Dual Console", "No"),
("Force Feedback", "No"),
("Fluorescence Imaging", "No"),
("Table Motion", "No"),
("Docking Time", "Moderate; improved over Standard"),
("Setup", "Interactive touchscreen added"),
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Key Improvements over Standard:</b>", styles['bold_label']))
story.extend(bullet_list([
"3D High-Definition (HD) camera - the single most important visual leap in the platform's early history",
"Lighter, more streamlined patient-side cart with improved aesthetics",
"Updated software architecture with faster processing",
"Autofocus camera system introduced (eliminating the manual focus pedal)",
"Simplified system setup with interactive touchscreen interface",
"Improved instrument compatibility and EndoWrist range",
"da Vinci S HD variant later released with further image quality improvements",
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Remaining Limitations:</b>", styles['bold_label']))
story.extend(bullet_list([
"Still uses column-based arm design; arms must be widely spaced",
"No dual-console capability",
"No fluorescence or near-infrared imaging",
"Operation times significantly longer than Xi (studies show ~85 min longer)",
"Docking time still ~16 min vs later generations",
], styles))
story.append(PageBreak())
return story
def gen_si(styles):
story = []
story.append(section_header("DA VINCI Si", "2009", "3rd Generation", styles))
story.append(Spacer(1, 0.5*cm))
story.append(Paragraph(
"The da Vinci Si (2009) became the most widely disseminated robotic surgery platform globally. "
"It introduced the transformative dual-console capability, enabling proctored surgery and "
"resident/fellow training. The computing brain was moved from the surgeon's console to the "
"vision cart - a strategic architecture shift that enabled all future improvements.",
styles['body']
))
story.append(Spacer(1, 0.4*cm))
story.append(specs_table([
("FDA Clearance", "2009"),
("Arms", "4 (column-mounted)"),
("Camera", "Fixed dedicated camera arm"),
("Vision", "HD 3D + TilePro multi-input display"),
("Dual Console", "YES - first dual-console system"),
("Force Feedback", "No"),
("Fluorescence Imaging", "YES - real-time near-infrared"),
("Table Motion", "No"),
("Docking Time", "~19 min (longer than Xi)"),
("Computing", "Moved to vision cart (architectural shift)"),
("Communication", "Two fiber-optic cables between components"),
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Key Improvements over S:</b>", styles['bold_label']))
story.extend(bullet_list([
"Dual-console surgery: a second surgeon console connects to the same patient cart - enabling proctored training and hand-off during complex procedures",
"System computing moved from surgeon's console to the vision cart - sleeker console design and modular future upgrades",
"Communication simplified to just two optic fiber cables between system components",
"TilePro software: multiple video inputs (e.g., ultrasound + endoscope) displayed simultaneously on console",
"Real-time fluorescence/near-infrared imaging (e.g., for sentinel node mapping, blood flow assessment)",
"Touchscreen added to arm rest for intraoperative system configuration",
"Assistant touchscreen on vision cart for parallel setup",
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Remaining Limitations:</b>", styles['bold_label']))
story.extend(bullet_list([
"Patient cart design unchanged from S - arms still on central column",
"Longer docking time (~19 min) vs Xi (~9.5 min)",
"No overhead boom architecture; limited multi-quadrant repositioning",
"Accuracy: FLE ~1.64 mm vs ~0.97 mm for Xi",
], styles))
story.append(PageBreak())
return story
def gen_xi(styles):
story = []
story.append(section_header("DA VINCI Xi", "2014", "4th Generation", styles))
story.append(Spacer(1, 0.5*cm))
story.append(Paragraph(
"The da Vinci Xi (2014) was the most radical redesign in the platform's history. "
"The entire patient-side cart was rebuilt from scratch with an overhead boom architecture "
"that suspended the arms above the patient. This unlocked multi-quadrant surgery without "
"re-docking and made the Xi the gold standard for complex minimally invasive procedures. "
"It remains the most widely used multiport robotic system in the world.",
styles['body']
))
story.append(Spacer(1, 0.4*cm))
story.append(specs_table([
("FDA Clearance", "2014"),
("Arms", "4 (overhead boom-mounted; any arm = camera)"),
("Instrument Size", "All instruments and camera: 8 mm"),
("Camera", "Any of the 4 arms can hold the camera"),
("Vision", "HD 3D + Firefly fluorescence imaging integrated"),
("Dual Console", "YES"),
("Force Feedback", "No"),
("Table Motion", "YES - integrated table motion (patient repositioning without undocking)"),
("Docking Time", "~9.5 min (vs ~19 min for Si)"),
("Accuracy (FLE)", "0.97 mm (vs 1.64 mm for Si)"),
("Port Setup", "Laser-guided port positioning system"),
("Instrument Reach", "Expanded workspace vs Si"),
("Vessel Sealer", "Vessel Sealer Extend: seals/cuts up to 7 mm"),
("Cannulas", "Fully reusable stainless steel; bladeless/blunt tip options"),
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Landmark Improvements over Si:</b>", styles['bold_label']))
story.extend(bullet_list([
"Overhead boom architecture: arms suspended from horizontal boom above surgical field - no central column",
"Arms numbered 1-4; ANY arm can hold the camera (no fixed camera arm)",
"360-degree approach: dock from any angle, access any abdominal quadrant without re-docking",
"Smaller arm spacing (one fist-width vs widely spaced) reduces external collisions",
"Thinner arms with redesigned joints: greater internal range of motion and improved patient clearance",
"Laser-guided port positioning for optimal trocar placement",
"Integrated table motion: patient repositioning intraoperatively without breaking the sterile field",
"Submillimetric accuracy: FLE 0.97 mm vs 1.64 mm on Si",
"Shorter docking time: ~9.5 min (50% faster than Si)",
"Firefly near-infrared fluorescence imaging fully integrated",
"Second-generation Vessel Sealer Extend (up to 7 mm vessels)",
"Improved robotic stapling with articulation and intelligent feedback",
], styles))
story.append(PageBreak())
return story
def gen_x(styles):
story = []
story.append(section_header("DA VINCI X", "2017", "Budget Hybrid (3rd/4th Gen Bridge)", styles))
story.append(Spacer(1, 0.5*cm))
story.append(Paragraph(
"The da Vinci X is not a true new generation - it is a cost-optimized hybrid designed to "
"give hospitals access to Xi-generation instruments at a lower acquisition price. It uses "
"the Si platform's patient-side cart, modified to accept Xi EndoWrist instruments.",
styles['body']
))
story.append(Spacer(1, 0.4*cm))
story.append(specs_table([
("Released", "2017"),
("Patient Cart", "Si-based cart (column design) modified for Xi instruments"),
("Instruments", "Xi-generation EndoWrist instruments (8 mm)"),
("Camera", "Fixed camera arm (Si-style)"),
("Vision", "HD 3D"),
("Dual Console", "YES (limited)"),
("Force Feedback", "No"),
("Table Motion", "No"),
("Purpose", "Cost reduction vs full Xi system"),
("Overhead Boom", "No - retains Si column design"),
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Positioning:</b>", styles['bold_label']))
story.extend(bullet_list([
"Entry-level option for hospitals unable to afford the full Xi platform",
"Bridges instrument compatibility between 3rd and 4th generation platforms",
"Shares Xi-generation instrument inventory, useful for multi-robot institutions",
"Not recommended for complex multi-quadrant cases requiring full Xi flexibility",
"Has since been phased out in favor of Xi and da Vinci 5",
], styles))
story.append(Spacer(1, 0.6*cm))
story.append(section_header("DA VINCI SP", "2018 / 2019", "Single-Port Variant (Xi Platform)", styles))
story.append(Spacer(1, 0.5*cm))
story.append(Paragraph(
"The da Vinci SP was originally designed on the Si platform but that version never reached "
"the market. The released system is built on the Xi platform. It is uniquely designed for "
"single-incision and natural orifice surgery, delivering all instruments and the camera "
"through a single cannula.",
styles['body']
))
story.append(Spacer(1, 0.4*cm))
story.append(specs_table([
("FDA Clearance", "2018 (urology); expanded 2019+"),
("Base Platform", "Xi"),
("Arms", "1 outer arm; 3 articulating instruments + camera inside"),
("Entry", "Single cannula (all instruments through one port)"),
("Camera", "Fully articulating 3D HD endoscope"),
("Vision", "3D HD articulating endoscope"),
("Access Route", "Single incision OR natural orifice (transoral, transvaginal, transanal)"),
("Instrument Behavior", "Instruments diverge inside patient, then converge at target"),
("Footprint", "Smaller than Xi"),
("Dual Console", "No"),
("Force Feedback", "No"),
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Clinical Advantages of SP:</b>", styles['bold_label']))
story.extend(bullet_list([
"Ideal for confined anatomical spaces: retroauricular neck surgery, pelvis, urethra, vagina",
"Only one skin incision required (or natural orifice entry)",
"Fully articulating camera provides improved visualization in narrow spaces",
"Enables procedures previously impossible with standard multiport robotic systems",
"Used in transoral robotic surgery (TORS) for oropharynx and larynx",
], styles))
story.append(PageBreak())
return story
def gen_dv5(styles):
story = []
story.append(section_header("DA VINCI 5", "2024", "5th Generation", styles))
story.append(Spacer(1, 0.5*cm))
story.append(Paragraph(
"The da Vinci 5 received FDA clearance in March 2024 and represents the most significant "
"leap in the platform since the Xi in 2014. While it shares the Xi's proven boom architecture "
"externally, nearly everything under the skin has been redesigned. It brings over 150 design "
"innovations, 10,000x the computing power of the Xi, and introduces the first force feedback "
"technology in the platform's history.",
styles['body']
))
story.append(Spacer(1, 0.4*cm))
story.append(specs_table([
("FDA Clearance", "March 2024"),
("Arms", "4 (overhead boom - same architecture as Xi)"),
("Camera", "Any arm (same as Xi)"),
("Vision", "Next-generation 3D imaging (improved over Xi)"),
("Computing Power", "10,000x more than da Vinci Xi"),
("Force Feedback", "YES - first in da Vinci history"),
("Tremor/Vibration", "Best-ever filtration (improved input + output)"),
("Hand Controllers", "Redesigned curved haptic arms (more ergonomic)"),
("Docking Speed", "~2x faster than Xi"),
("Table Motion", "YES (integrated, same as Xi)"),
("Fluorescence", "YES (enhanced)"),
("OR Footprint", "Smaller than Xi"),
("Data Integration", "My Intuitive+, SimNow VR, Case Insights, Intuitive Hub"),
("Dual Console", "YES"),
("Indications", "Same as Xi EXCEPT cardiac and pediatric (as of 2024)"),
("Force Feedback Contraindication", "Hysterectomy and myomectomy for Force Feedback needle driver"),
], styles))
story.append(Spacer(1, 0.4*cm))
story.append(Paragraph("<b>Landmark Advances over Xi:</b>", styles['bold_label']))
story.extend(bullet_list([
"Force Feedback: sensors measure tissue interaction forces; haptic resistance felt in surgeon's hands - toggleable on/off. Most significant sensory advance in the platform's 25-year history",
"10,000x computing power: enables AI-driven features, real-time analytics, and future autonomous capabilities",
"Redesigned hand controllers with curved haptic arms; thicker for more electronics and better tremor filtration",
"Additional arm sensors for improved precision and sub-millimetric accuracy",
"~2x faster docking workflow with guided, task-automated setup",
"Surgeons make fewer staff requests for settings changes (streamlined intraoperative workflow)",
"Universal user interface across all three system components (cart, console, vision system)",
"Integration with My Intuitive+ for objective surgical performance review and personalized training",
"SimNow VR simulator tightly integrated for training and credentialing",
"Case Insights: AI-driven computational observer flags key surgical events from recorded video",
"Smaller OR footprint than Xi",
"Cost: ~15% higher than full Xi stack (inclusive of table motion, hub, simulation items bundled)",
], styles))
story.append(PageBreak())
return story
# ── Comparison table ───────────────────────────────────────────────────────────
def build_comparison_table(styles):
story = []
header_data = [[Paragraph("FULL COMPARISON TABLE", styles['section_title'])]]
ht = Table(header_data, colWidths=[PAGE_W - 4*cm])
ht.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), DARK_BLUE),
('TOPPADDING', (0,0), (-1,-1), 0.6*cm),
('BOTTOMPADDING', (0,0), (-1,-1), 0.6*cm),
('LEFTPADDING', (0,0), (-1,-1), 0.8*cm),
]))
story.append(ht)
story.append(Spacer(1, 0.5*cm))
def H(text): return Paragraph(f"<b>{text}</b>", styles['table_header'])
def C(text, bold=False):
st = ParagraphStyle('tc', fontName='Helvetica-Bold' if bold else 'Helvetica',
fontSize=8, textColor=TEXT_DARK, alignment=TA_CENTER, leading=11)
return Paragraph(text, st)
def CL(text):
st = ParagraphStyle('tcl', fontName='Helvetica-Bold', fontSize=8,
textColor=TEXT_DARK, alignment=TA_LEFT, leading=11)
return Paragraph(text, st)
YES = lambda: Paragraph("<b><font color='#27AE60'>YES</font></b>", ParagraphStyle('y', fontName='Helvetica-Bold', fontSize=8, alignment=TA_CENTER))
NO = lambda: Paragraph("<font color='#C0392B'>No</font>", ParagraphStyle('n', fontName='Helvetica', fontSize=8, alignment=TA_CENTER))
PART = lambda t: Paragraph(f"<font color='#E67E22'>{t}</font>", ParagraphStyle('p', fontName='Helvetica', fontSize=8, alignment=TA_CENTER))
col_w = [3.8*cm, 2.2*cm, 2.2*cm, 2.2*cm, 2.5*cm, 2.0*cm, 2.0*cm, 2.5*cm]
table_data = [
# Header
[H("Feature"), H("Standard\n1999"), H("S\n2006"), H("Si\n2009"), H("Xi\n2014"), H("X\n2017"), H("SP\n2018"), H("DV5\n2024")],
# Rows
[CL("Arms"), C("3→4"), C("4"), C("4"), C("4"), C("4"), C("1 (3 inst)"), C("4")],
[CL("Fixed Camera Arm"), YES(), YES(), YES(), NO(), YES(), C("Integrated"), NO()],
[CL("HD Vision"), NO(), YES(), YES(), YES(), YES(), YES(), C("Enhanced")],
[CL("3D Vision"), YES(), YES(), YES(), YES(), YES(), YES(), YES()],
[CL("Dual Console"), NO(), NO(), YES(), YES(), PART("Limited"), NO(), YES()],
[CL("Fluorescence (NIR)"), NO(), NO(), YES(), YES(), YES(), YES(), C("Enhanced")],
[CL("Force Feedback"), NO(), NO(), NO(), NO(), NO(), NO(), YES()],
[CL("Table Motion"), NO(), NO(), NO(), YES(), NO(), NO(), YES()],
[CL("Overhead Boom"), NO(), NO(), NO(), YES(), NO(), NO(), YES()],
[CL("Single Port"), NO(), NO(), NO(), NO(), NO(), YES(), NO()],
[CL("Docking Time"), C("Slow"), C("~16 min"), C("~19 min"), C("~9.5 min"), C("Moderate"), C("N/A"), C("~2x faster\nthan Xi")],
[CL("Accuracy (FLE mm)"), C("~1.31"), C("~1.31"), C("~1.64"), C("0.97"), C("~1.0"), C("N/A"), C("<0.97")],
[CL("AI / Data Integration"), NO(), NO(), NO(), PART("Basic"), NO(), NO(), YES()],
[CL("Computing Power"), C("Basic"), C("Basic"), C("Moderate"), C("Moderate"), C("Moderate"), C("Moderate"), C("10,000x vs Xi")],
[CL("Laser Port Guide"), NO(), NO(), NO(), YES(), NO(), NO(), YES()],
[CL("OR Footprint"), C("Large"), C("Large"), C("Large"), C("Moderate"), C("Moderate"), C("Compact"), C("Smaller than Xi")],
]
ct = Table(table_data, colWidths=col_w, repeatRows=1)
ct.setStyle(TableStyle([
# Header row
('BACKGROUND', (0,0), (-1,0), DARK_BLUE),
('TEXTCOLOR', (0,0), (-1,0), WHITE),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
# Alternating rows
('ROWBACKGROUNDS', (0,1), (-1,-1), [WHITE, LIGHT_GREY]),
# Feature column left-align
('ALIGN', (0,1), (0,-1), 'LEFT'),
('LEFTPADDING', (0,0), (0,-1), 6),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
('FONTSIZE', (0,0), (-1,-1), 8),
('GRID', (0,0), (-1,-1), 0.4, colors.HexColor("#CCCCCC")),
('BOX', (0,0), (-1,-1), 1, ACCENT),
# Highlight DV5 column
('BACKGROUND', (7,1), (7,-1), colors.HexColor("#EAF4FB")),
]))
story.append(ct)
story.append(PageBreak())
return story
# ── Summary / Takeaways ────────────────────────────────────────────────────────
def build_summary(styles):
story = []
header_data = [[Paragraph("SUMMARY & KEY TAKEAWAYS", styles['section_title'])]]
ht = Table(header_data, colWidths=[PAGE_W - 4*cm])
ht.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), DARK_BLUE),
('TOPPADDING', (0,0), (-1,-1), 0.6*cm),
('BOTTOMPADDING', (0,0), (-1,-1), 0.6*cm),
('LEFTPADDING', (0,0), (-1,-1), 0.8*cm),
]))
story.append(ht)
story.append(Spacer(1, 0.5*cm))
milestones = [
("1999/2000 - Standard", "First commercial platform. Proved robotic surgery was viable. EndoWrist instruments and immersive 3D console established the template all successors follow."),
("2006 - da Vinci S", "HD vision transformed surgical detail. Autofocus and lighter cart improved usability. Established the platform in broader clinical use."),
("2009 - da Vinci Si", "Dual-console surgery changed surgical education. Moving the system brain to the vision cart was the architectural foundation for all future generations."),
("2014 - da Vinci Xi", "The most radical redesign. Overhead boom, any-arm camera, 360-degree access, laser port guidance, integrated table motion, and sub-mm accuracy. Set the global standard."),
("2017 - da Vinci X", "Cost-access bridge. Not a clinical leap but made Xi-generation instruments available at lower cost. Now largely superseded."),
("2018 - da Vinci SP", "Enabled single-port and natural orifice procedures previously impossible robotically. Key for urology, ENT, and colorectal."),
("2024 - da Vinci 5", "First force feedback in 25 years. 10,000x computing power unlocks AI features. Fastest docking, best ergonomics, and most data-rich platform ever built."),
]
for name, desc in milestones:
row_data = [[
Paragraph(f"<b>{name}</b>", ParagraphStyle('ml', fontName='Helvetica-Bold', fontSize=10, textColor=WHITE, leading=14)),
Paragraph(desc, styles['body']),
]]
row_table = Table(row_data, colWidths=[4.5*cm, PAGE_W - 8.5*cm])
row_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,-1), MID_BLUE),
('BACKGROUND', (1,0), (1,-1), LIGHT_GREY),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 8),
('BOTTOMPADDING', (0,0), (-1,-1), 8),
('LEFTPADDING', (0,0), (0,-1), 8),
('LEFTPADDING', (1,0), (1,-1), 10),
('LINEBELOW', (0,0), (-1,-1), 0.5, WHITE),
]))
story.append(row_table)
story.append(Spacer(1, 0.8*cm))
advice_data = [[
Paragraph("<b>Choosing a Platform</b>", ParagraphStyle('adv', fontName='Helvetica-Bold', fontSize=11, textColor=WHITE, leading=16)),
]]
adv_header = Table(advice_data, colWidths=[PAGE_W - 4*cm])
adv_header.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), ACCENT),
('TOPPADDING', (0,0), (-1,-1), 0.4*cm),
('BOTTOMPADDING', (0,0), (-1,-1), 0.4*cm),
('LEFTPADDING', (0,0), (-1,-1), 0.8*cm),
]))
story.append(adv_header)
story.append(Spacer(1, 0.3*cm))
advice = [
"For highest capability multiport surgery: da Vinci 5 (2024) is the top choice with force feedback and AI integration",
"For most widely-deployed proven multiport platform: da Vinci Xi (2014) with 7+ million procedures recorded",
"For single-incision or natural orifice approaches: da Vinci SP",
"For cost-sensitive entry: da Vinci X (though Xi is strongly preferred for clinical versatility)",
"The S and Si are largely phased out of new installations; Si may still be in active use at some centers",
"The Standard (Classic) has been fully retired",
]
story.extend(bullet_list(advice, styles))
story.append(Spacer(1, 0.8*cm))
story.append(HRFlowable(width="100%", thickness=1, color=ACCENT))
story.append(Spacer(1, 0.3*cm))
story.append(Paragraph(
"Sources: Intuitive Surgical product data, PMC10683436 (History of Robotic Surgery), "
"PMC8155181 (S/Si/Xi outcomes comparison), PMC9540612 (Xi vs Si accuracy), "
"FDA 510(k) clearance records, and peer-reviewed surgical literature.",
styles['caption']
))
return story
# ── Main ───────────────────────────────────────────────────────────────────────
def main():
styles = make_styles()
doc = SimpleDocTemplate(
OUTPUT_PATH,
pagesize=A4,
rightMargin=2*cm, leftMargin=2*cm,
topMargin=1.8*cm, bottomMargin=2.0*cm,
title="Da Vinci Surgical Robot Generations Comparison Guide",
author="Orris Medical AI",
subject="Robotic Surgery Platform Comparison",
)
story = []
story += build_cover(styles)
story += build_toc(styles)
story += gen_standard(styles)
story += gen_s(styles)
story += gen_si(styles)
story += gen_xi(styles)
story += gen_x(styles)
story += gen_dv5(styles)
story += build_comparison_table(styles)
story += build_summary(styles)
doc.build(story, canvasmaker=HeaderCanvas)
print(f"PDF saved to: {OUTPUT_PATH}")
if __name__ == "__main__":
main()
cd /home/daytona/workspace/davinci-guide && python3 create_pdf.py 2>&1
ls -lh /home/daytona/workspace/davinci-guide/DaVinci_Generations_Guide.pdf
DaVinci Generations Guide
PDF Document · PDF
- Title banner, generation timeline strip (1999 - 2024), and executive summary paragraph
- Numbered entries for all 9 sections
- Da Vinci Standard (1999) - 1st Gen
- Da Vinci S (2006) - 2nd Gen
- Da Vinci Si (2009) - 3rd Gen
- Da Vinci Xi (2014) - 4th Gen
- Da Vinci X (2017) + SP (2018) - hybrid/single-port
- Da Vinci 5 (2024) - 5th Gen
- All 7 platforms side-by-side across 16 features (HD vision, dual console, force feedback, docking time, accuracy, AI integration, etc.)
- Milestone timeline, platform selection guide, and source citations
What was the actual use of puma650 robotic surgery
PUMA 560 650 robotic surgery first use 1985 neurosurgery history
PUMA robot surgical use history neurosurgery
https://pmc.ncbi.nlm.nih.gov/articles/PMC4677089
PUMA 560/200 in Robotic Surgery - The Pioneer
What Was the PUMA?
The Landmark First Use - 1985
What Actually Happened:
- A patient needed a cerebral biopsy - a needle had to be inserted into the brain at a precise target identified on CT imaging
- Human hands are subject to tremor, which can be catastrophic when placing a needle millimeters from critical brain structures
- Dr. Kwoh's team programmed the PUMA 560 to hold and guide the biopsy cannula/needle based on CT scan coordinates
- The robot was used purely as a stable positioning and holding platform - it was not autonomous and did not "perform" surgery independently
- The surgeon still controlled the procedure; the robot eliminated tremor and provided geometric precision that human hands could not match
- The procedure was successful
Why Neurosurgery First?
- Brain targets are often only a few millimeters in size
- Human hand tremor of even 1-2 mm could mean hitting eloquent cortex or major vessels
- Open skull surgery (craniotomy) was the only alternative to a robotic needle guide
- The PUMA offered a way to reach deep brain targets through a small burr hole with millimeter precision guided by CT coordinates
Follow-on Surgical Uses of the PUMA Platform
| Year | Procedure | Key Detail |
|---|---|---|
| 1985 | CT-guided brain biopsy | First ever robot in surgery; needle placement only |
| 1988 | Transurethral resection of the prostate (TURP) | PUMA used to position resectoscope; significant because it required robotic manipulation inside a body cavity |
| 1988+ | Further neurosurgical frameless stereotaxy | Continued use for needle-based deep brain targets |
What the PUMA Was NOT
- It was not autonomous - it did not decide where to go; surgeons programmed coordinates from CT/imaging
- It had no force feedback or tissue sensing
- It did not replace the surgeon - it was a tool holder/guide
- It had no vision system of its own
- It was an off-the-shelf industrial arm repurposed without surgical-specific design (no sterility features, no safety interlocks designed for human tissue)
What the PUMA Led To
- ROBODOC (1992) - Integrated Surgical Systems; designed for milling precise femoral cavities in hip replacement
- PROBOT (1992) - Imperial College London; first robot to perform surgery entirely autonomously (prostatectomy), derived from PUMA experience
- NeuroMate (1987 development, FDA approved 1997) - First commercially available neurosurgical robot; used in 1,000+ cases
- Minerva (1991) - University of Lausanne; first neurosurgery robot not requiring a stereotactic frame
- AESOP (1994, FDA approved) - Computer Motion; voice-controlled robotic laparoscope arm
- ZEUS (1998) - Computer Motion; full robotic surgery system
- da Vinci (2000) - Intuitive Surgical; the direct evolutionary descendant of everything the PUMA proved possible
Summary
Compare early surgical robots (PUMA, AESOP, ZEUS) vs da Vinci
AESOP ZEUS robotic surgery specifications history Computer Motion vs da Vinci comparison
ZEUS AESOP robotic surgery history comparison da Vinci
https://pmc.ncbi.nlm.nih.gov/articles/PMC10445506
ZEUS robotic surgical system patient table arms image PUMA 560 surgical robot operating room photo
Early Surgical Robots vs. Da Vinci - A Complete Comparison
Visual Gallery



1. PUMA 560 (1985)
| Attribute | Detail |
|---|---|
| Type | Passive/semi-active positioning arm |
| Arms | 1 (single industrial arm) |
| Degrees of Freedom | 6 (industrial spec) |
| Vision | None (relied on external CT) |
| Control | Pre-programmed coordinates from CT imaging; no real-time surgeon control |
| Surgeon Interface | None - preprogrammed before procedure |
| Tremor Filtering | Yes (inherent to mechanical rigidity) |
| Motion Scaling | No |
| Telepresence | No |
| Autonomous | Partially - held position autonomously, not surgeon-controlled in real time |
| Sterility | Not designed for OR environment |
| Force Feedback | No |
- CT-guided stereotactic brain biopsy (1985)
- Transurethral resection of prostate (TURP) positioning (1988)
2. AESOP - Automated Endoscopic System for Optimal Positioning (1992/1994)
| Attribute | Detail |
|---|---|
| Type | Camera/endoscope positioning arm (single purpose) |
| Arms | 1 (endoscope holder only) |
| Degrees of Freedom | 6 |
| Vision | Controlled the laparoscope/endoscope; no independent vision |
| Control | Voice commands from surgeon ("AESOP, move up / move right / zoom in") |
| Surgeon Interface | Voice recognition system + optional foot pedal |
| Tremor Filtering | Yes - stable camera platform |
| Motion Scaling | No |
| Telepresence | No |
| Instrument Arms | None - camera only |
| Force Feedback | No |
| Cost | Lower than ZEUS/da Vinci |
3. ZEUS Robotic Surgical System (1998/2001)
| Attribute | Detail |
|---|---|
| Type | Full master-slave telemanipulator |
| Arms | 3 (table-mounted independently) |
| Arm Mounting | Each arm independently clamped to the operating table |
| Camera Arm | AESOP arm (voice-controlled endoscope) |
| Instrument Arms | 2 arms; each with 4 degrees of freedom |
| Vision | 2D standard OR optional 3D; 2D flat-screen monitor at console |
| Surgeon Console | Seated; flat video monitor; two hand-control handles |
| Tremor Filtering | Yes |
| Motion Scaling | Yes - 2:1 to 10:1 (surgeon's large movement scaled to tiny instrument movement) |
| Telepresence | YES - first system to demonstrate transatlantic remote surgery |
| Force Feedback | No (visual feedback only) |
| Autonomy | None - fully surgeon-controlled |
| Instrument Count | Up to 28 different surgical instruments by 2000 |
- 1998 - First clinical use: uterine tube anastomosis (Cleveland Clinic)
- September 24, 1999 - World's first robotically-assisted closed-chest beating-heart bypass surgery (London Health Sciences Centre; Dr. Douglas Boyd)
- September 7, 2001 - "Operation Lindbergh" - The most famous moment in ZEUS history: Surgeons in New York performed a laparoscopic cholecystectomy (gallbladder removal) on a patient in Strasbourg, France via a high-speed fiber optic connection with 150ms latency. 54-minute procedure; no complications. First ever transatlantic robotic surgery.
- Arms mounted to the operating table individually - not from a unified cart; this caused arm collision problems and complex positioning
- Only 4 degrees of freedom per instrument arm (vs. 7 in da Vinci's EndoWrist)
- 2D visualization at the console (flat monitor) vs. da Vinci's immersive stereoscopic 3D binocular viewer
- No wrist articulation at the instrument tip (instruments moved rigidly like laparoscopic tools)
- Console ergonomics were poor for long cases
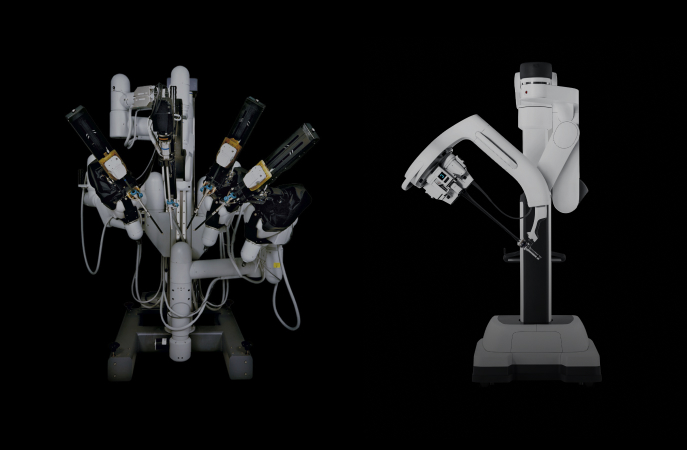
4. Da Vinci Surgical System (1999/2000)
| Attribute | Detail |
|---|---|
| Type | Full master-slave telemanipulator |
| Arms | 3 (Standard) then 4 |
| Arm Mounting | All arms from a single unified patient cart |
| Camera | Dedicated camera arm (fixed) - later any arm in Xi |
| Instrument Arms | 2-3; EndoWrist instruments |
| Vision | Immersive stereoscopic 3D binocular viewer at surgeon's console |
| Degrees of Freedom | 7 DoF + 2 axial rotation per instrument (wrist articulation) |
| Surgeon Console | Fully immersive; head-mounted binocular 3D viewer; finger-loop controls; foot pedals |
| Tremor Filtering | Yes |
| Motion Scaling | Yes |
| Telepresence | Yes |
| Force Feedback | No (added in da Vinci 5, 2024) |
| EndoWrist | YES - instruments articulate at the tip like a human wrist |
Head-to-Head Comparison: The Four Systems
| Feature | PUMA 560 | AESOP | ZEUS | Da Vinci |
|---|---|---|---|---|
| Year | 1985 | 1992/1994 | 1998/2001 | 1999/2000 |
| Manufacturer | Unimation | Computer Motion | Computer Motion | Intuitive Surgical |
| Purpose | Needle positioning | Camera holding | Full telemanipulation | Full telemanipulation |
| No. of Arms | 1 | 1 | 3 | 3-4 |
| Arm Mounting | Floor-standing | Table/cart | Table (each arm separate) | Unified patient cart |
| Surgeon Console | None | Voice commands | Flat screen + hand controls | Immersive 3D binocular viewer |
| Vision | External CT only | Controlled laparoscope | 2D flat monitor (opt. 3D) | Stereoscopic 3D (HD from S gen) |
| Degrees of Freedom | 6 (industrial) | 6 | 4 per instrument arm | 7 + 2 axial per instrument |
| Wrist Articulation (EndoWrist) | No | No | No | YES |
| Tremor Filtering | Yes (passive) | Yes | Yes | Yes |
| Motion Scaling | No | No | Yes (2:1 to 10:1) | Yes |
| Telepresence/Telesurgery | No | No | Yes | Yes |
| Transatlantic Surgery | No | No | Yes (Lindbergh, 2001) | No (at that time) |
| Instrument Arms | 0 | 0 | 2 | 2-3 |
| Instrument Library | 0 (held biopsy needle) | 0 | 28 instruments | 100+ instruments |
| Force Feedback | No | No | No | No (until 2024) |
| FDA Cleared for Surgery | No (experimental) | Yes (1994) | Yes (2001) | Yes (2000) |
| Dual Console | No | No | No | From Si (2009) |
| Dedicated OR Design | No (industrial robot) | Yes | Yes | Yes |
| Status | Retired | Discontinued 2003 | Discontinued 2003 | Active (da Vinci 5 current) |
| Approx. Cost | N/A (industrial) | ~$100K | $975,000 | $1,000,000+ |
The Critical Differences Explained
1. Why da Vinci Won Over ZEUS
2. The Merger That Ended the Competition
3. What Each Contributed to the Lineage
PUMA 560 (1985)
→ proved robots could work in the human body
AESOP (1994)
→ proved voice-controlled camera positioning was practical
ZEUS (1998)
→ proved full master-slave telemanipulation and telesurgery
Da Vinci (2000)
→ combined all lessons + added 3D vision + wrist articulation
→ set the standard for the next 25 years
Summary
Give me a detailed history of evolution of robotic suregry
complete history evolution robotic surgery 1970s to 2024 timeline milestones
history robotic surgery evolution milestones
https://pmc.ncbi.nlm.nih.gov/articles/PMC10683436
robotic surgery future 2020s AI autonomous surgery new competitors Hugo Versius Senhance
The Complete History of Robotic Surgery: 1960s to 2026
ERA 1: The Conceptual Origins (1960s - 1970s)
The Word "Robot" and Early Concepts
NASA and DARPA - The Real Instigators
- NASA began funding research in the 1970s into how surgeons could treat astronauts in space or inaccessible locations without being physically present - the concept of telepresence surgery
- DARPA (Defense Advanced Research Projects Agency) simultaneously explored how surgeons could operate on wounded soldiers at the front lines without being there - a robotic surgical system mounted in an armored vehicle that could "virtually" bring the surgeon to the battlefield
- Researchers Phil Green, Richard Satava and the Stanford Research Institute (SRI) developed early telepresence prototypes under these DARPA contracts - prototypes that would eventually become the direct ancestors of the da Vinci system
ERA 2: First Robots in the OR (1985 - 1991)
1985 - PUMA 560: The First Robot in Surgery
1988 - PROBOT (Imperial College London)
1988 - Onward - PUMA for TURP
ERA 3: Purpose-Built Surgical Robots (1992 - 1997)
1992 - ROBODOC (Integrated Surgical Systems + IBM)
- First used in human subjects 1992
- Remains to this day the only active robotic system cleared by the FDA for orthopedic surgery
- Demonstrated that "active" robots (robots that perform tissue manipulation autonomously, not just hold tools) were safe and valuable
1992 - AESOP 1st Generation (Computer Motion Inc.)
- AESOP 1000 (1992/1994): foot-pedal controlled; FDA cleared 1994 - first FDA-cleared robot to assist in surgery
- AESOP 2000 (1996): replaced pedal with voice control ("AESOP, move up / zoom in") - surgeon controlled the camera hands-free while operating
- AESOP 3000: more degrees of freedom
- AESOP HR (HERMES Ready): integrated OR-wide voice control of lights, table, and instruments
1991 - Minerva (University of Lausanne)
1992 - NeuroMate (Integrated Surgical Systems)
ERA 4: The Race to Full Telemanipulation (1998 - 2003)
1997-1998 - SRI / Intuitive Surgical Prototype Becomes da Vinci
- First clinical use: 1997-1998 at Cleveland Clinic
- FDA clearance for general laparoscopy: July 11, 2000
- Key innovation: EndoWrist instruments with 7 degrees of freedom + 2 axial rotations - the instrument tip articulated like a human wrist inside the body; immersive stereoscopic 3D binocular viewer
1998 - ZEUS (Computer Motion)
- 3 arms independently table-mounted; 4 degrees of freedom per instrument arm
- Surgeon console: flat video monitor + two hand controls
- First clinical use 1998 (Cleveland Clinic - uterine tube anastomosis)
- 1999 - First robotically-assisted closed-chest beating-heart bypass (CABG) surgery (Dr. Douglas Boyd, London)
- FDA clearance: October 2001
September 7, 2001 - "Operation Lindbergh" - The Transatlantic Surgery
- Total procedure time: 54 minutes
- Communication latency: 155 milliseconds
- No technical complications
- Cost of telecommunications: over $1 million
- First ever transatlantic robotic surgery; proved telesurgery across intercontinental distances was physically possible
2000-2003 - The Patent War
March 2003 - The Merger That Ended the War
ERA 5: The Da Vinci Monopoly and Specialty Expansion (2003 - 2014)
Key Procedures Established in This Era:
| Year | Milestone |
|---|---|
| 2000 | FDA clearance for general laparoscopy |
| 2001 | First robotic prostatectomy (radical prostatectomy) - became the killer app |
| 2002 | First robotic cardiac valve repair |
| 2003 | ZEUS discontinued; Intuitive dominant |
| 2004-2006 | Robotic hysterectomy, myomectomy, sacrocolpopexy in gynecology |
| 2005 | da Vinci S launched - HD 3D vision |
| 2006-2008 | Robotic partial nephrectomy, pyeloplasty established in urology |
| 2009 | da Vinci Si launched - dual console, fluorescence imaging, TilePro |
| 2010s | Robotic colorectal surgery, esophagectomy, pancreatectomy, gastrectomy |
Robotic Prostatectomy - The Defining Procedure
ERA 6: Fourth Generation and Design Revolution (2014 - 2019)
2014 - Da Vinci Xi: The Most Radical Redesign
- 360-degree docking from any angle
- Multi-quadrant surgery without re-docking
- Any arm could hold the camera
- Laser-guided port placement
- Integrated table motion
- Sub-millimetric accuracy (FLE 0.97mm)
- Docking time cut in half vs. Si
2018-2019 - Da Vinci SP: Single Port
2017-2019: The First Challengers Emerge
- CMR Surgical (UK, founded 2014): developing Versius - a modular, portable robotic system with small individual arm units that could be positioned anywhere around the table
- TransEnterix/Asensus Surgical: Senhance system - haptic feedback (first in soft tissue robotics), eye-tracking camera control, reusable instruments
- Medtronic: announced intent to build Hugo RAS - a modular, AI-integrated system
ERA 7: The AI Era and Market Opening (2020 - 2026)
2020 - Versius (CMR Surgical) - Modular Architecture
- Modular design: each arm is an independent unit on a small wheeled cart - any number can be positioned around the patient in any configuration
- Small footprint, easy OR integration
- Used in 30,000+ procedures in 30+ countries as of 2024
- Second most widely deployed soft-tissue robotic system globally
- Strong adoption in Europe, India, Latin America
2021 - January: First Fully Autonomous Laparoscopic Procedure
2022 - ChatGPT and AI in Surgery
- Real-time phase recognition: AI identifies which step of an operation is occurring
- Instrument tracking: AI tracks every instrument tip in the surgical field
- Complication prediction: AI flags anatomical danger zones
- Automated documentation: AI generates operative notes from video
- Caresyntax, Activ Surgical, Theator emerged as AI surgical analytics companies
2024 - Da Vinci 5: Force Feedback at Last
- Force feedback sensors - surgeons feel tissue resistance in their hands for the first time
- 10,000x the computing power of Xi
- 150+ design innovations
- Redesigned ergonomic hand controllers
- ~2x faster docking
- Integration with AI analytics (My Intuitive+, Case Insights)
December 2025 - The Monopoly Officially Ends
- Medtronic Hugo RAS - FDA cleared December 2025. Modular AI-integrated system with machine learning camera tracking, cloud-connected performance dashboards, lower cost footprint
- CMR Surgical Versius Plus - FDA cleared December 2025. Entered US market after 4+ years of international clinical use
ERA 8: Where It's Heading (2026 and Beyond)
Fully Autonomous Surgery
- Task-specific autonomy first (suturing, stapling, vessel sealing with no surgeon input)
- Supervised autonomy (surgeon monitors, intervenes only if needed)
- Full procedural autonomy (theorized for 2030s+)
AI Integration
- Real-time anatomical overlays from preoperative CT/MRI projected onto the live surgical field
- AI-assisted dissection planes: the robot knows where the ureter is before the surgeon sees it
- Personalized training: AI reviews every procedure and gives surgeons objective performance scores
New Market Entrants (2025-2026)
| Platform | Company | Notable Feature |
|---|---|---|
| Hugo RAS | Medtronic | Modular, AI-integrated, FDA cleared Dec 2025 |
| Versius Plus | CMR Surgical (UK) | Most portable soft-tissue robot; FDA cleared Dec 2025 |
| Dexter | Distalmotion (Switzerland) | Works with existing laparoscopic infrastructure |
| Ottava | J&J/Ethicon | Under development; J&J re-entered the space |
| neuroArm | University of Calgary | MRI-compatible neurosurgical robot |
| Ion / Monarch | Intuitive / Auris Health | Robotic bronchoscopy and lung biopsy |
| Mako Smart Robotics | Stryker | Orthopedic joint replacement (hip/knee) |
| VELYS | J&J | Robotic knee replacement |
Miniaturization
Telesurgery Revival
The 40-Year Arc: A Summary
1970s → NASA/DARPA: Concept (treat soldiers/astronauts remotely)
1985 → PUMA 560: First robot touches a human patient
1988 → PROBOT: First purpose-built surgical robot
1992 → ROBODOC: First active robot; AESOP: Camera control
1994 → AESOP FDA cleared: First cleared surgical robot
1998 → ZEUS: First full telemanipulator in clinical use
1999 → Da Vinci: First 3D + wrist articulation + immersive console
2000 → Da Vinci FDA cleared: Modern robotic surgery begins
2001 → Operation Lindbergh: Transatlantic surgery proved possible
2003 → Merger: Intuitive monopoly begins
2005-14 → Da Vinci S → Si → Xi: HD vision, dual console, boom architecture
2014 → Xi: Overhead boom, any-arm camera, 9.5-min docking
2018 → SP: Single-port surgery
2021 → STAR: First autonomous bowel anastomosis (animal model)
2024 → Da Vinci 5: Force feedback after 25 years
2025 → Hugo + Versius Plus FDA cleared: Monopoly ends
2026+ → AI integration, autonomous task surgery, global competition
Create a detailed PDF on robotic surgery history from 1960s to 2026
mkdir -p /home/daytona/workspace/robotic-surgery-history && echo "ready"