Mitral regurgitation
Reading File
Finding Sources
Searching PubMed
"mitral regurgitation" management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Here is the full clinical review of mitral regurgitation.
Mitral Regurgitation (MR)
Overview
MR is (together with aortic stenosis) the most prevalent valvular heart disease in the general population, affecting roughly 9-10% of elderly patients in the United States. Prevalence is estimated at ~20% when mild MR is included, and it is predominantly a disease of the elderly - prevalence will likely double before 2050. Untreated significant MR carries a 1-year mortality or heart failure hospitalization rate of ~34%, with 5-year survival of 46% for secondary MR and 66% for primary MR.
- Braunwald's Heart Disease, p. 1456; Fuster and Hurst's The Heart 15e, p. 938
Classification
MR is divided into two fundamentally distinct categories:
| Feature | Primary (Organic) MR | Secondary (Functional) MR |
|---|---|---|
| Leaflet pathology | Intrinsic valve/apparatus disease | Leaflets structurally normal |
| Mechanism | Leaflet prolapse, flail, perforation, retraction | LV/LA dilatation displaces papillary muscles, impairing coaptation |
| Common causes | MVP, rheumatic disease, infective endocarditis, connective tissue disorders, degenerative | Dilated cardiomyopathy, ischemic LV dysfunction, atrial fibrillation with LA enlargement |
- Braunwald's Heart Disease, p. 1456
Mitral Valve Anatomy
The MV is a complex 3D structure. Coordinated interaction of the annulus, commissures, leaflets, chordae tendineae, papillary muscles, and left ventricle is required for functional integrity. Abnormalities of any of these components can cause MR.
- The annulus is saddle-shaped with anterior and posterior peaks
- The anterior leaflet (A1, A2, A3 scallops) is larger; the posterior leaflet (P1, P2, P3) is more restricted
- Chordae tendineae anchor leaflets to the posteromedial and anterolateral papillary muscles
Causes of MR (Braunwald Table 76.1)
Acute MR
- Papillary muscle rupture (MI)
- Infective endocarditis (leaflet perforation)
- Trauma (blunt chest injury, balloon valvotomy)
- Spontaneous chordae rupture
- Atrial myxoma
Chronic Primary MR
- Degenerative: Myxomatous disease (Barlow syndrome, fibro-elastic deficiency), Marfan syndrome, Ehlers-Danlos syndrome
- Inflammatory: Rheumatic heart disease, SLE (Libman-Sacks)
- Infective: Endocarditis
- Structural: Ruptured chordae, papillary muscle dysfunction (post-MI), annular calcification
- Congenital: Cleft mitral valve, parachute MV
Secondary MR
- Dilated cardiomyopathy
- Ischemic cardiomyopathy (apical PM displacement)
- Atrial functional MR (LA enlargement with annular dilatation)
Pathophysiology
Chronic Primary MR
In chronic MR, the LV initially compensates by eccentric hypertrophy - increased end-diastolic volume maintains forward stroke volume. Because part of each stroke volume is regurgitated into the low-pressure LA, afterload appears reduced, preserving an often supranormal ejection fraction. This compensation can mask true LV dysfunction for years.
A key clinical pearl: an EF of 55% in severe MR may represent substantial reduction in myocardial systolic function, as EF is artificially elevated by the low-resistance regurgitant pathway. LV end-systolic diameter ≥40 mm or LVEF ≤60% are guideline thresholds for intervention.
Over time, progressive volume overload leads to LV systolic dysfunction, LA enlargement, pulmonary hypertension, and atrial fibrillation.
Secondary MR
Pathophysiology involves apical displacement of the papillary muscles due to LV dilatation/remodeling, tethering the leaflets toward the apex and preventing adequate systolic coaptation. The result is functional (central or posterior-directed) regurgitation despite structurally normal leaflets. Secondary MR creates a vicious cycle: volume overload worsens LV dilatation, which worsens the tethering.
- Harrison's Principles of Internal Medicine 22e, p. 1936; Braunwald's Heart Disease, p. 1465
Clinical Features
Symptoms
- Chronic MR: Often asymptomatic for many years; symptoms emerge with LV decompensation - exertional dyspnea, reduced exercise tolerance, fatigue, orthopnea, PND, palpitations (AF)
- Acute severe MR: Pulmonary edema, hemodynamic collapse (papillary muscle rupture post-STEMI is a surgical emergency)
Physical Examination
- Murmur: Holosystolic, high-pitched, blowing murmur, best heard at apex, radiating to axilla (or to base in posterior leaflet prolapse)
- In MVP: late-systolic murmur preceded by mid-systolic click
- In acute MR: murmur may be short and early-systolic (rapid LA pressure rise equalizes pressures)
- Apex beat: Hyperdynamic, displaced laterally (volume overloaded LV)
- S3 gallop: Indicates significant volume overload
- Loud P2 / right heart signs: In chronic severe MR with pulmonary hypertension
Echocardiography
Echo is the cornerstone of diagnosis and quantification. The key parameters are:
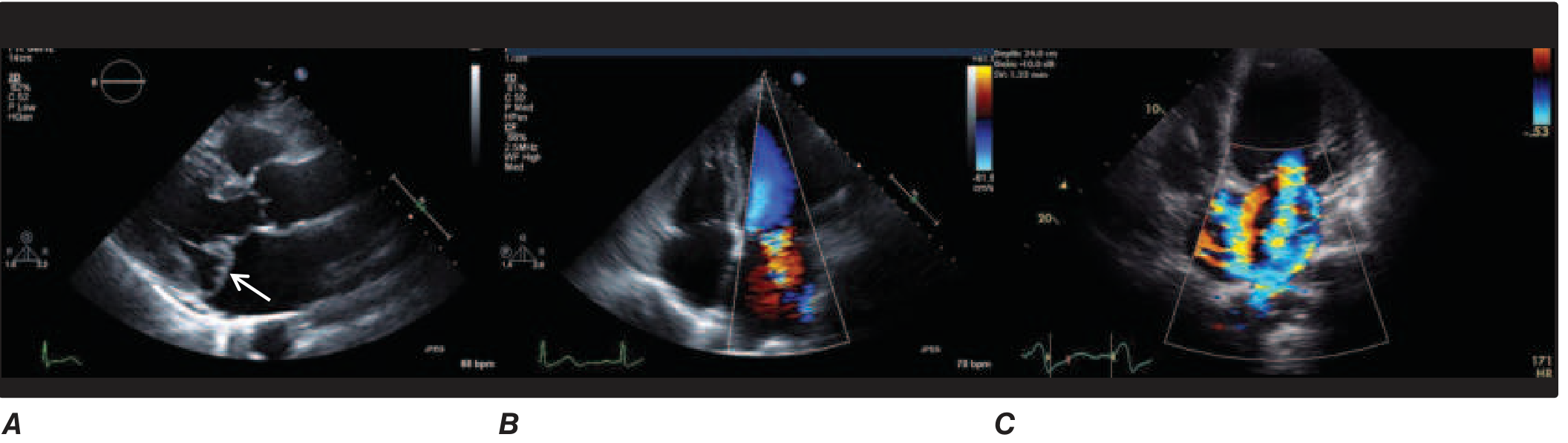
FIGURE 248-22 (Harrison's 22e) - A: MVP with posterior leaflet prolapse. B: Color Doppler MR jet in MVP. C: Severe functional (secondary) MR in a dilated LV.
Severity Grading (Quantitative Parameters)
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Vena contracta width | <3 mm | 3-6.9 mm | ≥7 mm |
| EROA (PISA) | <20 mm² | 20-39 mm² | ≥40 mm² |
| Regurgitant volume | <30 mL | 30-59 mL | ≥60 mL |
| Regurgitant fraction | <30% | 30-49% | ≥50% |
PISA method simplification: When aliasing velocity ~40 cm/sec, EROA ≈ r²/2 (where r = radius of convergence zone).
Important caveat: Color jet area alone is unreliable - affected by driving pressure, machine settings, and LA compliance. Quantitative methods (EROA, regurgitant volume, regurgitant fraction) are strongly preferred.
In secondary MR, a "disproportionate MR" concept has emerged: EROA that is disproportionately large relative to the degree of LV dilatation (EROA ≥30 mm² despite LVEF ≥30%) may predict greater benefit from intervention.
CMR is the reference technique when echo is inconclusive - it directly measures regurgitant volume and provides tissue characterization.
- Braunwald's Heart Disease, p. 779; Fuster and Hurst's The Heart 15e, p. 966
Natural History & Prognostic Markers
Primary MR
- Asymptomatic patients with preserved LV function: low mortality but progressive LV remodeling
- LVEF ≤60% or LVESD ≥40 mm: independent predictors of mortality
- New-onset AF: independently associated with adverse outcome (including sudden cardiac death in flail leaflet - RR 2.4)
- Pulmonary hypertension (PASP >50 mmHg): triggers consideration for surgery
- LA diameter ≥40 mm: associated with AF, thromboembolism, endocarditis
Secondary MR
- Worse prognosis than primary (5-year survival 46% vs 66%)
- Higher risk patients: LVEF <30%, significant LV dilatation, RV dysfunction, elevated BNP
- Global longitudinal strain <7%: independently associated with increased all-cause mortality
Management
Primary MR
Medical Therapy
No pharmacologic treatment improves outcomes in primary MR with preserved LV function. Vasodilators have shown only short-term hemodynamic benefits in small studies. Beta-blockers show no consistent benefit unless LVEF is depressed. Guidelines recommend heart failure-directed therapy (GDMT including ACEi/ARB, beta-blocker, MRA) only when LVEF is reduced.
Surgical Indications (ACC/AHA 2020 / ESC 2021)
- Class I: Surgery when LVEF ≤60% or LVESD ≥40 mm (even if asymptomatic), or in symptomatic patients with LVEF >30%
- Class I: Surgery in asymptomatic patients with preserved LVEF when new-onset AF or resting PASP >50 mmHg is present
- Class IIa: Asymptomatic patients with progressive severe MR, normal LV function, and high likelihood of durable repair (>95% repair rate at an experienced center)
Repair vs. Replacement: Mitral valve repair is strongly preferred over replacement when feasible - it preserves LV function, avoids prosthesis-related complications, and carries lower operative mortality. Repair rates of >95% are achievable for posterior leaflet prolapse at experienced centers.
Secondary MR
Medical/Device Therapy (First-Line)
Optimizing GDMT for underlying heart failure is mandatory first:
- ACE inhibitors/ARBs, beta-blockers, MRA, SGLT2i
- Cardiac resynchronization therapy (CRT): significantly reduces secondary MR in appropriate candidates (LBBB, LVEF <35%, QRS >150 ms)
Surgical Therapy
- Ring annuloplasty (undersized): most common repair - reduces annular circumference to improve leaflet coaptation
- Chordal sparing mitral valve replacement (MVR): may be preferred over annuloplasty repair when durable repair is unlikely; the CTSN trial showed similar LV remodeling at 1-2 years but higher MR recurrence after repair (59% vs 3.8% at 2 years)
- Combined CABG + MV surgery in ischemic MR with suitable anatomy and viable myocardium
- Surgical mortality in secondary MR with LV dysfunction: 4-5% in contemporary series (previously 10-20%)
Transcatheter Therapy (MitraClip - Edge-to-Edge Repair)
The MitraClip device (PASCAL is a newer alternative) replicates the Alfieri stitch - grasping the A2 and P2 scallops to create a double-orifice valve.
Primary MR: FDA-approved for prohibitive surgical risk patients. EVEREST II demonstrated non-inferiority to surgery in safety but lower efficacy (greater residual MR).
Secondary MR: The COAPT trial (Stone et al., NEJM 2018) demonstrated that MitraClip significantly reduced heart failure hospitalization and all-cause mortality compared to medical therapy in carefully selected patients (LVEF 20-50%, EROA ≥30 mm², symptoms despite GDMT). The MITRA-FR trial was negative - differences attributed to patient selection (MITRA-FR enrolled patients with less "disproportionate" MR relative to LV size).
2025 Meta-analysis update: A systematic review (PMID 40851316, 2025) comparing MitraClip to surgery for secondary MR confirms MitraClip offers comparable short-term outcomes with lower procedural risk in suitable patients.
Current guidelines recommend MitraClip for secondary MR in patients with:
-
LVEF 20-50%
-
EROA ≥30 mm² (disproportionate MR)
-
Persistent symptoms despite optimal GDMT (including CRT if indicated)
-
Favorable anatomy (no severe mitral stenosis, adequate leaflet mobility)
-
Braunwald's Heart Disease, p. 1463-1470; Fuster and Hurst's The Heart 15e, p. 966
Acute Mitral Regurgitation
Acute severe MR is a hemodynamic emergency. The LV and LA have no time to compensate - sudden volume overload causes rapid rise in LA pressure with flash pulmonary edema.
Causes: Papillary muscle rupture (posteromedial PM, supplied by single coronary artery - more vulnerable), infective endocarditis with leaflet destruction, chordae rupture, blunt trauma.
Management:
- Stabilization: IV nitroprusside (afterload reduction) ± IABP (intra-aortic balloon pump) to reduce regurgitant fraction
- Definitive: Emergency surgery - delay worsens outcomes dramatically; surgery even in cardiogenic shock carries better outcomes than medical management
Summary Table: Key Decision Points
| Clinical Scenario | Recommendation |
|---|---|
| Asymptomatic primary MR, LVEF >60%, LVESD <40 mm | Active surveillance; surgery if repair likely at experienced center |
| Symptomatic primary MR, LVEF >30% | Surgery (repair preferred) |
| Primary MR + LVEF ≤60% or LVESD ≥40 mm | Surgery regardless of symptoms |
| Secondary MR - asymptomatic | Optimize GDMT + CRT if indicated |
| Secondary MR - symptomatic despite GDMT, LVEF 20-50%, EROA ≥30 mm² | MitraClip or surgery (MitraClip preferred if high surgical risk) |
| Acute severe MR | Emergency surgery ± nitroprusside/IABP bridge |
Recent Evidence (2025)
- PMID 40851316: MitraClip vs surgery for secondary MR meta-analysis (2025) - comparable outcomes with lower procedural risk for MitraClip
- PMID 40793956: Treatment strategies for ischemic MR - systematic review and meta-analysis (2025) - coronary revascularization alone is insufficient for severe ischemic MR; combined MV surgery + CABG yields better outcomes
- PMID 40849614: Antithrombotic therapy post mitral valve repair (network meta-analysis 2025) - addresses optimal anticoagulation strategies post-repair
Sources: Braunwald's Heart Disease, 2 Vol Set, Fuster and Hurst's The Heart 15e, Harrison's Principles of Internal Medicine 22e, Textbook of Clinical Echocardiography
This is a shared conversation. Sign in to Orris to start your own chat.