Insulin classes and indications
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-sourced answer.
Insulin Classes and Indications
Overview
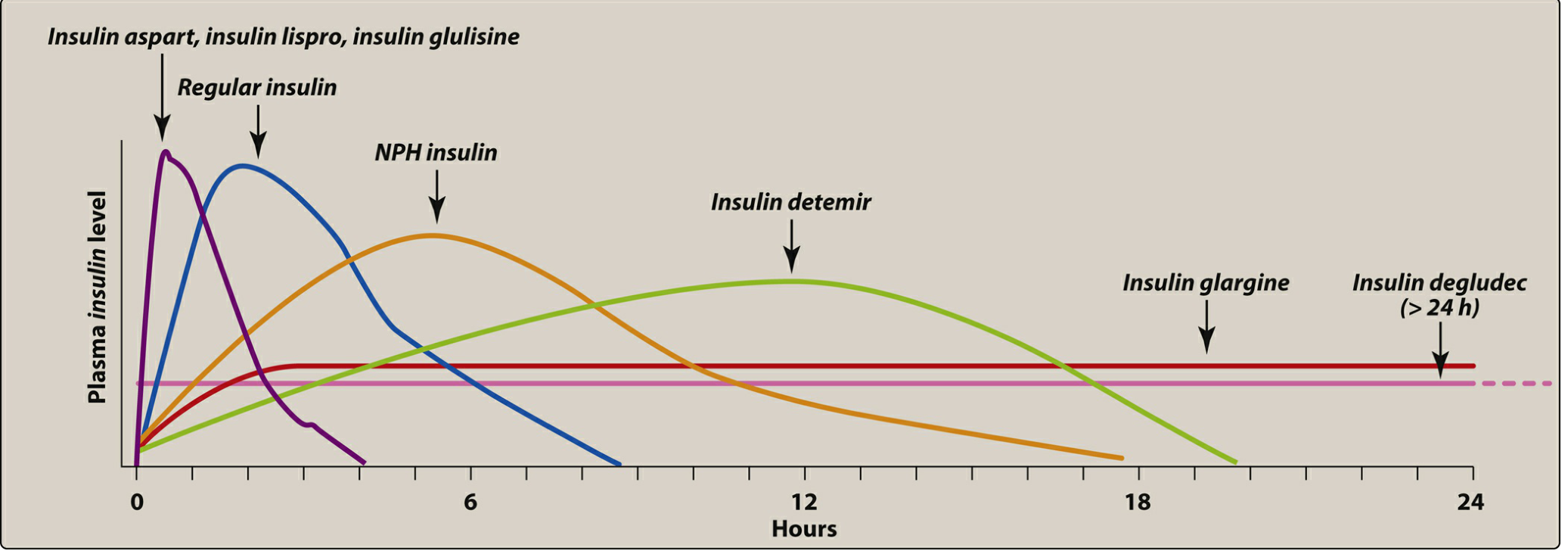
Insulin preparations are classified by their onset, peak, and duration of action into four main categories: rapid-acting, short-acting, intermediate-acting, and long-acting. Each class has distinct pharmacokinetic profiles and clinical uses.
Human insulin is produced by recombinant DNA technology. Modification of the amino acid sequence of human insulin creates analogs with improved pharmacokinetic properties. Currently, three rapid-acting analogs (lispro, aspart, glulisine) and three long-acting analogs (glargine, detemir, degludec) are available in the US, alongside human regular insulin and NPH.
Class 1: Rapid-Acting Insulins
| Agent | Brand(s) | Onset | Peak | Duration |
|---|---|---|---|---|
| Insulin lispro | Humalog, Admelog, Lyumjev | 5-15 min | 30-90 min | 3-4 h |
| Insulin aspart | Novolog, FIASP | 5-15 min | 1-1.5 h | 3-4 h |
| Insulin glulisine | Apidra | 5-15 min | 1-1.5 h | 3-4 h |
| Inhaled insulin | Afrezza | 5-15 min | ~10-20 min | ~3 h |
Mechanism: Amino acid substitutions in lispro, aspart, and glulisine reduce self-association of insulin molecules, resulting in faster subcutaneous absorption compared to regular insulin.
Indications:
- Prandial (mealtime) glucose control - administered 15 minutes before a meal (or within 15-20 min after starting a meal)
- Postprandial glucose correction
- Continuous subcutaneous insulin infusion (insulin pumps) - rapid-acting analogs are the standard pump insulin
- Can be given IV (though regular insulin is more commonly used IV)
- Inhaled insulin is contraindicated in asthma, COPD, and smokers due to bronchospasm risk
Class 2: Short-Acting Insulin
| Agent | Brand(s) | Onset | Peak | Duration |
|---|---|---|---|---|
| Regular insulin (soluble) | Humulin R, Novolin R | 30-60 min | ~2 h | 6-8 h |
| Regular U-500 | Humulin R U-500 | 30-60 min | 2-3 h | Up to 24 h |
Note: Regular insulin is a soluble, crystalline zinc insulin. U-500 (500 units/mL, 5x concentrated) behaves more like an intermediate-acting insulin.
Indications:
- Prandial coverage - given 30 minutes before a meal (slower onset than analogs)
- Intravenous infusion in hyperglycemic emergencies (DKA, HHS, perioperative/ICU glucose management) - regular insulin is the standard for IV use
- Sliding scale correction protocols in hospitalized patients
- U-500 for highly insulin-resistant type 2 DM patients requiring large doses
Class 3: Intermediate-Acting Insulin
| Agent | Brand(s) | Onset | Peak | Duration |
|---|---|---|---|---|
| NPH (Neutral Protamine Hagedorn) | Humulin N, Novolin N | 2-4 h | 6-7 h | 10-20 h |
Mechanism: Zinc and protamine are added to regular insulin, forming a less-soluble complex that delays absorption. Also called insulin isophane.
Indications:
- Basal insulin coverage in type 1 or type 2 DM - typically given twice daily
- Combined with rapid- or short-acting insulin for mealtime + basal control
- Available as premixed formulations (e.g., 70% NPH/30% regular; 75% NPL/25% lispro)
- Never given IV - only subcutaneous
- Not appropriate when rapid glucose lowering is needed (e.g., DKA)
Class 4: Long-Acting Insulins (Basal Analogs)
| Agent | Brand(s) | Onset | Peak | Duration |
|---|---|---|---|---|
| Insulin glargine | Lantus, Basaglar, Semglee, Toujeo (U-300) | 0.5-1 h | Flat (peakless) | ~24 h |
| Insulin detemir | Levemir | 0.5-1 h | Flat | ~17 h |
| Insulin degludec | Tresiba (U-100 & U-200) | 0.5-1.5 h | Flat | >42 h |
Mechanism: Each agent achieves prolonged, peakless action through different strategies:
- Glargine - isoelectric point shift causes microprecipitation at the SC injection site
- Detemir - reversibly binds to albumin via a fatty acid chain, extending duration
- Degludec - forms multi-hexamer complexes that slowly dissociate; ultra-long action >42 hours enables flexible dosing
Indications:
- Basal glucose control (primarily fasting and between-meal glucose) in type 1 and type 2 DM
- Type 1 DM: combined with rapid-acting insulin for a basal-bolus regimen (the standard intensive approach)
- Type 2 DM: added to oral agents when fasting glucose is not at target; titrated to fasting blood glucose
- Degludec's ultra-long duration allows for flexible (not daily-fixed-time) dosing - an advantage for patients with irregular schedules
- Never given IV - subcutaneous only
Summary Table: Pharmacokinetics at a Glance
| Class | Examples | Onset | Peak | Duration | Key Use |
|---|---|---|---|---|---|
| Rapid-acting | Lispro, Aspart, Glulisine, Inhaled | 5-15 min | 30-90 min | 3-4 h | Mealtime bolus, insulin pumps |
| Short-acting | Regular (R) | 30-60 min | ~2 h | 6-8 h | Pre-meal, IV use, DKA/HHS |
| Intermediate | NPH | 2-4 h | 6-7 h | 10-20 h | Basal (BID), premixed combos |
| Long-acting | Glargine, Detemir, Degludec | 0.5-1.5 h | Flat/peakless | 17 - >42 h | Once-daily basal |
Clinical Indications Summary
| Indication | Preferred Insulin(s) |
|---|---|
| Type 1 DM (standard) | Basal-bolus: long-acting (glargine/detemir/degludec) + rapid-acting (lispro/aspart/glulisine) |
| Type 2 DM - initial insulin | Long-acting basal (add to oral agents); titrate to fasting glucose |
| Type 2 DM - intensification | Add rapid-acting prandial insulin if HbA1c not at goal |
| DKA / HHS (emergency) | IV regular insulin infusion |
| Hospitalized (non-ICU) | SC long-acting basal + rapid-acting for prandial/correction ("basal-bolus") |
| Insulin pump (CSII) | Rapid-acting analog only (lispro, aspart, or glulisine) |
| Gestational DM | Regular insulin and NPH (most evidence); analogs increasingly used |
| Cystic fibrosis-related DM | Rapid-acting pre-meal ± basal if fasting hyperglycemia present |
Key Clinical Pearls
- Sulfonylureas should be stopped when short-acting prandial insulins are added - combined use increases hypoglycemia risk.
- Sliding-scale insulin alone (short-acting reactive dosing) is inferior to basal-bolus regimens in hospitalized patients.
- Rotation of injection sites is essential to prevent lipohypertrophy, which impairs absorption.
- Long-acting analogs (glargine, detemir, degludec) cannot be mixed with other insulins in the same syringe.
- Regular insulin is the only formulation suitable for IV administration in practice (rapid-acting analogs can be used IV but regular is standard).
- Renal insufficiency decreases insulin clearance - dose reduction is often required.
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Edition (Tables 41-5, 41-6)
- Lippincott Illustrated Reviews: Pharmacology (Chapter 24, Figure 24.7)
- Harrison's Principles of Internal Medicine 22E (Chapter 416)
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Edition (Table 12-9)
This is a shared conversation. Sign in to Orris to start your own chat.