45-year-old man with alcoholic cirrhosis is admitted to the intensive care unit for evaluation of hematemesis. On the morning of admission, he developed nausea and dizziness tollowed by a liquid, maroon stool. He subsequently vomited "a quart" of bright red blood. The patient's hemodynamic condition was stabilized. Upper gastrointestinal endoscopy shows large esophageal varices, one of which has adherent clot. No other bleeding site is seen. Sclerotherapy is administered to all visible varices. Twenty-four hours later he suddenly vomits a large volume of bright red blood. His pulse rate is 140/min, respiration rate is 36/min, and blood pressure is 70/40 mm Hg. Despite fluid resuscitation, he continues to behypotensive and vomit bright red blood. Which of the following is the most appropriate next step? A) Portosystemic shunt procedure B) Balloon-tamponade of the bleeding sarices. C) Intravenous vasopressm D) Iransiugular intraberatis pettesyst procedure Use source harrisons,scwartz,doherty
Answer: B) Balloon Tamponade of the Bleeding Varices
Clinical Scenario Analysis
- Active, massive, refractory variceal hemorrhage - continuing to vomit bright red blood despite initial sclerotherapy
- Hemodynamic collapse - BP 70/40 mmHg, HR 140, RR 36
- Persistent hypotension despite fluid resuscitation
- Sclerotherapy already failed (standard endoscopic therapy has been given)
Why B (Balloon Tamponade) is Correct
"Balloon tamponade (Sengstaken-Blakemore tube or Minnesota tube)... can be used in patients who need stabilization prior to endoscopic therapy or as a bridge to TIPS after endoscopic failure."
- Harrison's, Chapter 355 (Portal Hypertension / Variceal Hemorrhage)
"Up to 20% of variceal hemorrhage episodes may be refractory to standard therapy, and in these circumstances balloon tamponade can bridge to a definitive therapy such as TIPS... Although this method is highly effective in the initial control of bleeding, because of its transient effect it is only a temporizing bridge to a more definitive procedure (e.g., TIPS, surgical shunting, or transplantation) and is used only after endoscopic and pharmacologic therapies have failed."
- Mulholland/Greenfield, Chapter 59, p. 2917-2918
"When endoscopic therapy is either not available or is ineffective, hemorrhage may be temporarily halted by balloon tamponade using the Sengstaken-Blakemore or Minnesota tubes." - p. 456
"A TIPS shunt is the emergency procedure of choice in patients in whom endoscopic therapy has failed to control bleeding. Recent data confirm the utility and efficacy of TIPS stent as a salvage procedure for refractory variceal bleeding unresponsive to endoscopic and pharmacologic treatment."
Why the Other Options are Wrong in this Specific Clinical Context
| Option | Why Incorrect as the NEXT Step |
|---|---|
| A - Portosystemic shunt (surgical) | Emergency surgical shunting carries substantial operative mortality. Per Fischer's: it is restricted to patients who "failed endoscopic therapy and cannot be salvaged by TIPS for technical reasons." TIPS must be attempted before surgery. Not the immediate next step. |
| C - IV Vasopressin | Vasopressin is a pharmacologic adjunct used at the START of variceal bleeding management. At this point, the patient is exsanguinating and in hemodynamic collapse - vasopressin alone will not control massive hemorrhage that has already failed sclerotherapy. It is too little, too late. |
| D - TIPS (Transjugular Intrahepatic Portosystemic Shunt) | TIPS is the definitive next procedure after balloon tamponade stabilizes the patient. However, a patient with BP 70/40, HR 140, actively vomiting blood cannot undergo an IR procedure safely without first achieving temporary hemostasis. Balloon tamponade must bridge to TIPS - not the reverse. |
The Logical Treatment Cascade
Active variceal bleed
↓
1. Resuscitation + vasoactive drugs (octreotide/vasopressin) + antibiotics
↓
2. Endoscopic therapy (EVL or sclerotherapy) ← already done, FAILED
↓
3. ► BALLOON TAMPONADE ◄ (Sengstaken-Blakemore tube) ← CURRENT STEP
- Success rate: 70–80% in stopping acute bleed
- Duration: max 24 hours only
- Bridge to definitive therapy
↓
4. TIPS (definitive, >90% success in controlling refractory bleeding)
↓
5. Surgical shunt (if TIPS not feasible - last resort)
Key Teaching Point
The answer is B - Balloon Tamponade, as it is the only intervention that can immediately temporize massive, refractory variceal hemorrhage to allow the patient to be stabilized before undergoing TIPS.
Mallory weiss syndrome causes harrisons
Mallory-Weiss Syndrome - Causes (Harrison's, 22nd Ed)
Definition
"A Mallory-Weiss tear is a linear mucosal rent near or across the gastroesophageal junction that is often associated with retching or vomiting... When the tear disrupts a submucosal arteriole, brisk hemorrhage may result."
- Harrison's Principles of Internal Medicine, 22nd Ed, Chapter 333
Causes / Precipitating Factors
| Category | Specific Causes |
|---|---|
| Most common - Forceful expulsion | Vomiting, retching |
| Increased intra-abdominal pressure | Coughing, hiccupping, straining (e.g., lifting, defecation) |
| Alcohol-related | Heavy alcohol use - a classically associated history (leads to repeated retching/vomiting) |
| Predisposing anatomical factor | Hiatal hernia - present in the majority of patients; the disruption of the normal gastroesophageal anatomy makes the junction more vulnerable |
| Pregnancy | Hyperemesis gravidarum - persistent severe vomiting |
| Iatrogenic/procedural | Upper endoscopy, CPR, seizures |
| Portal hypertension / Cirrhosis | Worsens severity of bleeding once a tear occurs (increased venous pressure) |
"Violent vomiting can produce severe bleeding through a Mallory-Weiss lesion, a longitudinal tear in the mucosa at the gastroesophageal junction."
- Harrison's, Chapter on the Gastrointestinal System in Pregnancy
"A history of heavy alcohol use is commonly described, as is the presence of a hiatal hernia. Patients characteristically have an episode of nonbloody emesis, retching or coughing followed by hematemesis."
Classic Clinical Presentation
- Initial episode of non-bloody vomiting or retching
- Followed by hematemesis (bright red blood)
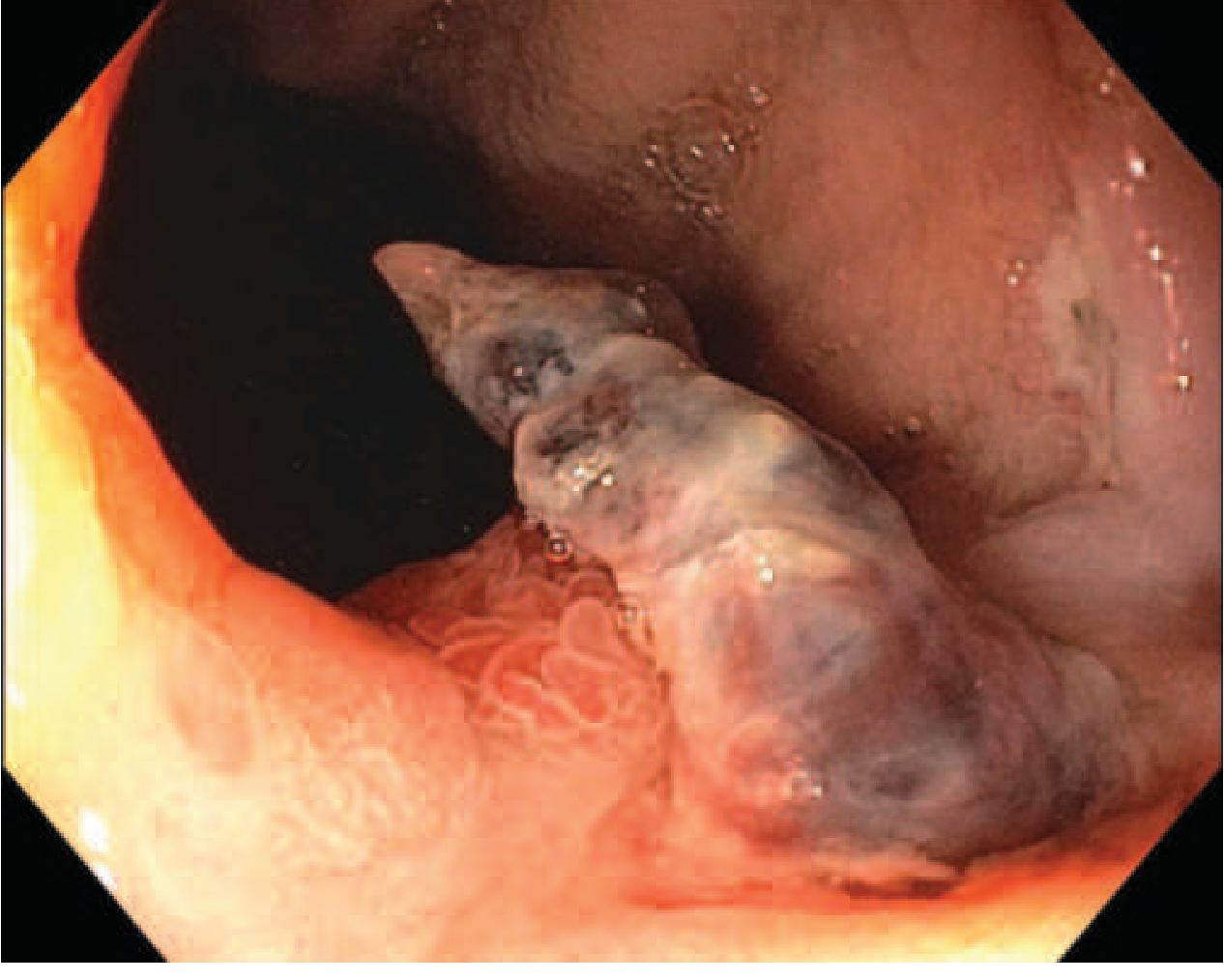
Endoscopic Image (Harrison's Fig. 333-40)
Key Points to Remember
- Location: Near or across the gastroesophageal junction (distal esophagus / proximal stomach)
- Mechanism: Sudden forceful increase in intra-abdominal/intragastric pressure → longitudinal mucosal tear → disruption of submucosal arteriole → hemorrhage
- Most common predisposing factors: Retching/vomiting + alcohol use + hiatal hernia
- Mortality: ~5% overall; higher with cirrhosis/portal hypertension, advanced age, or active bleeding at endoscopy
- Diagnosis: Upper endoscopy (gold standard)
- Treatment: Endoscopic hemostasis (coaptive coagulation, band ligation, or clip placement ± epinephrine injection); a nonbleeding sentinel clot rarely rebleeds and does NOT require endoscopic therapy
Did you finish
- Forceful vomiting / retching (most common trigger)
- Heavy alcohol use (classic associated history)
- Hiatal hernia (present in majority of patients - predisposing anatomical factor)
- Coughing, straining, hiccupping
- Hyperemesis gravidarum (pregnancy)
- Iatrogenic causes (endoscopy, CPR, seizures)
- Cirrhosis/portal hypertension (worsens bleeding severity)