Give me brief information about, brief information about the endometrial cancer.
Reading File
Finding Sources
Searching PubMed
"endometrial cancer"[MeSH Terms] AND diagnosis AND treatment
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive brief overview of endometrial cancer, drawn from authoritative medical textbooks.
Endometrial Cancer
Definition & Epidemiology
Endometrial cancer arises from the inner epithelial lining of the uterus (endometrium) and is the most common gynecologic cancer in women in the United States. It accounts for approximately 67,000 new cases and 13,000 deaths per year, making it the fourth most common cancer in women overall (after breast, lung, and colorectal cancers). Nearly 3% of U.S. women are expected to develop the disease in their lifetime. The average age at diagnosis is 60 years; it is rare before age 45. While it is more common in White women, Black women have a significantly higher mortality rate.
- Goldman-Cecil Medicine, p. 2094
Types
Endometrial cancers are broadly divided into two types:
| Feature | Type 1 | Type 2 |
|---|---|---|
| Estrogen | Dependent | Independent |
| Histology | Endometrioid adenocarcinoma | Clear cell or serous carcinoma |
| Patients | Younger, obese, perimenopausal | Older, thin, postmenopausal |
| Frequency | 80-85% | 15-20% |
| Prognosis | Lower grade, earlier stage | More aggressive, higher mortality |
| Molecular | ER/PR positive; MSI | TP53 mutations; ERBB2 overexpression |
Notably, serous and clear cell types make up less than 10% of cases yet account for more than half of all endometrial cancer deaths.
- Berek & Novak's Gynecology, p. 2141
Molecular Classification (TCGA)
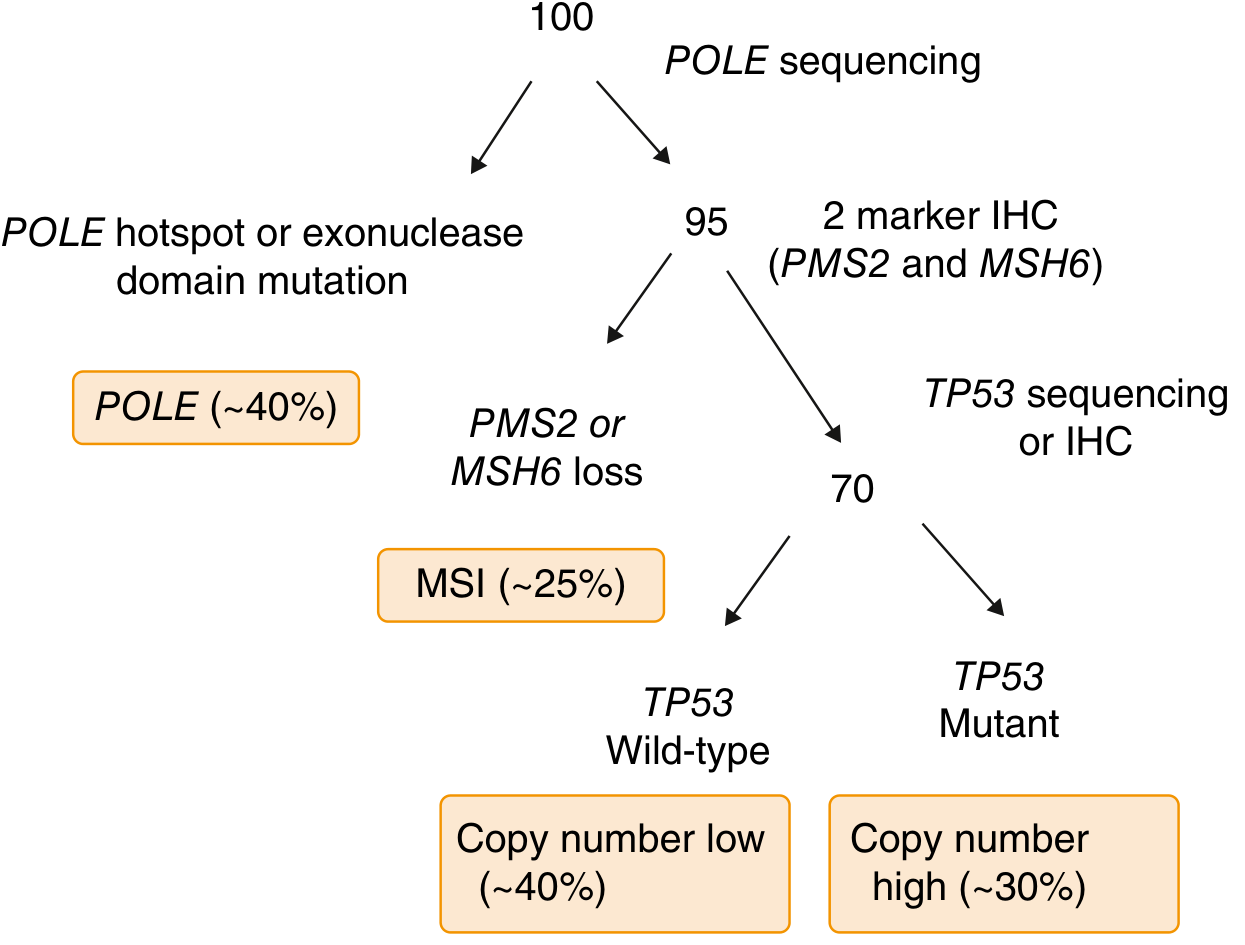
Modern molecular classification divides endometrial cancers into four subtypes based on POLE sequencing and immunohistochemistry:
-
POLE ultra-mutated (~5%) - best prognosis
-
MSI hypermutated (~25%) - intermediate prognosis; important for immunotherapy
-
Copy number low / TP53 wild-type (~40%) - intermediate prognosis
-
Copy number high / TP53 mutated (~30%) - worst prognosis
-
Goldman-Cecil Medicine, p. 2094-2095
Risk Factors
The most important risk factor is prolonged unopposed estrogen stimulation. Key risk factors include:
- Complex atypical hyperplasia (nearly 30-fold increased risk)
- Obesity (increased aromatase activity in adipose tissue converts androgens to estrogen)
- Nulliparity
- Diabetes mellitus
- Early menarche / late menopause
- Tamoxifen use
- Increasing age
- Lynch syndrome (up to 60% lifetime risk for endometrial cancer)
- Cowden syndrome (PTEN mutation; 13-20% lifetime risk)
- Family history of endometrial cancer (1.5-2x increased risk)
Sporadic cases account for the majority; only 3-5% are attributed to genetic predisposition.
- Goldman-Cecil Medicine, p. 2094
Clinical Features
- Abnormal uterine bleeding is the hallmark presenting symptom, occurring in about 90% of cases
- Postmenopausal bleeding should always raise suspicion
- Pelvic pain, palpable uterine mass, or weight loss may be present in advanced disease
- Most women present at an early, curable stage due to the prominent bleeding symptom
Diagnosis
- Office endometrial aspiration biopsy - the accepted first step in evaluating abnormal uterine bleeding or suspected endometrial pathology
- Transvaginal ultrasound - endometrial thickness >4 mm in postmenopausal women warrants further evaluation
- Hysteroscopy with directed biopsy - if aspiration biopsy is insufficient or non-diagnostic
- No effective screening test exists for the general population
- Berek & Novak's Gynecology, p. 2141
Staging (FIGO Surgical Staging)
Staging is surgical and includes hysterectomy, bilateral salpingo-oophorectomy, and peritoneal cytology. Lymph node assessment is required for most patients.
| Stage | Description |
|---|---|
| I | Confined to the uterine corpus |
| II | Cervical stromal invasion |
| III | Local/regional spread (adnexa, serosa, vagina, lymph nodes) |
| IV | Bladder/bowel involvement or distant metastasis |
Prognostic Variables
The most important adverse prognostic factors are:
- Advancing age
- Non-endometrioid or grade 3 histology
- Deep myometrial invasion
- Lymph-vascular space invasion
- Large tumor size
- Cervical extension
- Lymph node metastasis
- Intraperitoneal spread
Treatment
Surgery is the primary treatment for most patients:
- Total hysterectomy + bilateral salpingo-oophorectomy + surgical staging
Adjuvant therapy based on risk:
- Vaginal vault brachytherapy - for low-to-intermediate risk (reduces vaginal recurrence)
- External pelvic radiation - for intermediate to high-risk disease
- Chemotherapy (carboplatin + paclitaxel) - for high-risk, advanced, or recurrent disease
- Hormonal therapy (progestins) - for low-grade recurrent or metastatic disease
- Immunotherapy (pembrolizumab) - particularly effective in MSI-high or mismatch repair-deficient tumors
Radiation alone may be used as primary treatment for patients who are not surgical candidates.
- Berek & Novak's Gynecology, pp. 2141-2142
Prognosis
Overall prognosis is generally favorable because most patients (about 75%) present with Stage I disease, which carries a 5-year survival rate exceeding 90%. Advanced-stage and high-grade histologies have significantly worse outcomes.
Sources: Goldman-Cecil Medicine (International Edition) | Berek & Novak's Gynecology
This is a shared conversation. Sign in to Orris to start your own chat.