describe the actions of hormones aldesterone
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive overview of the actions of aldosterone, drawn from Brenner and Rector's The Kidney and Costanzo Physiology:
Aldosterone: Actions
Overview & Origin
Aldosterone is a mineralocorticoid steroid hormone secreted by the zona glomerulosa of the adrenal cortex. It is the principal hormone regulating Na⁺ balance, extracellular fluid (ECF) volume, and K⁺ excretion. Its secretion is primarily stimulated by:
- Angiotensin II (via the renin–angiotensin–aldosterone system, RAAS)
- Elevated plasma K⁺
- ACTH (minor role)
Mechanism of Action
As a steroid hormone, aldosterone passively enters target cells, binds to the intracellular mineralocorticoid receptor (MR), and the hormone–receptor complex translocates to the nucleus to regulate gene transcription and new protein synthesis. This accounts for a lag period of 45–60 minutes before measurable changes in ion transport — the classic genomic mechanism.
Aldosterone's effects are divided into three temporal phases:
- Latent phase — no measurable effect for 15–20 min
- Early phase — MR-dependent induction of signaling kinases (mainly SGK1), increasing apical localization/opening probability of ENaC
- Late phase — transcription of effector genes encoding ion transport proteins (ENaC subunits, Na⁺-K⁺-ATPase subunits)
Primary Epithelial Actions (Kidney)
The main target is the aldosterone-sensitive distal nephron (ASDN) — the late distal convoluted tubule (DCT), connecting tubule (CNT), and collecting duct — which expresses both MR and the enzyme 11β-hydroxysteroid dehydrogenase type 2 (11β-HSD2).
1. ↑ Na⁺ Reabsorption
- Aldosterone increases expression and membrane trafficking of ENaC (epithelial Na⁺ channel) on the apical membrane of principal cells
- Transcriptionally induces α-ENaC via a glucocorticoid response element in the SCNN1A gene promoter
- Rapidly induces SGK1 (serum- and glucocorticoid-inducible kinase 1), which phosphorylates Nedd4-2 to prevent ENaC ubiquitination and degradation, stabilizing ENaC at the apical surface
- Increases Na⁺-K⁺-ATPase (α₁ and β₁ subunits) expression on the basolateral membrane, pumping Na⁺ into the blood
2. ↑ K⁺ Secretion
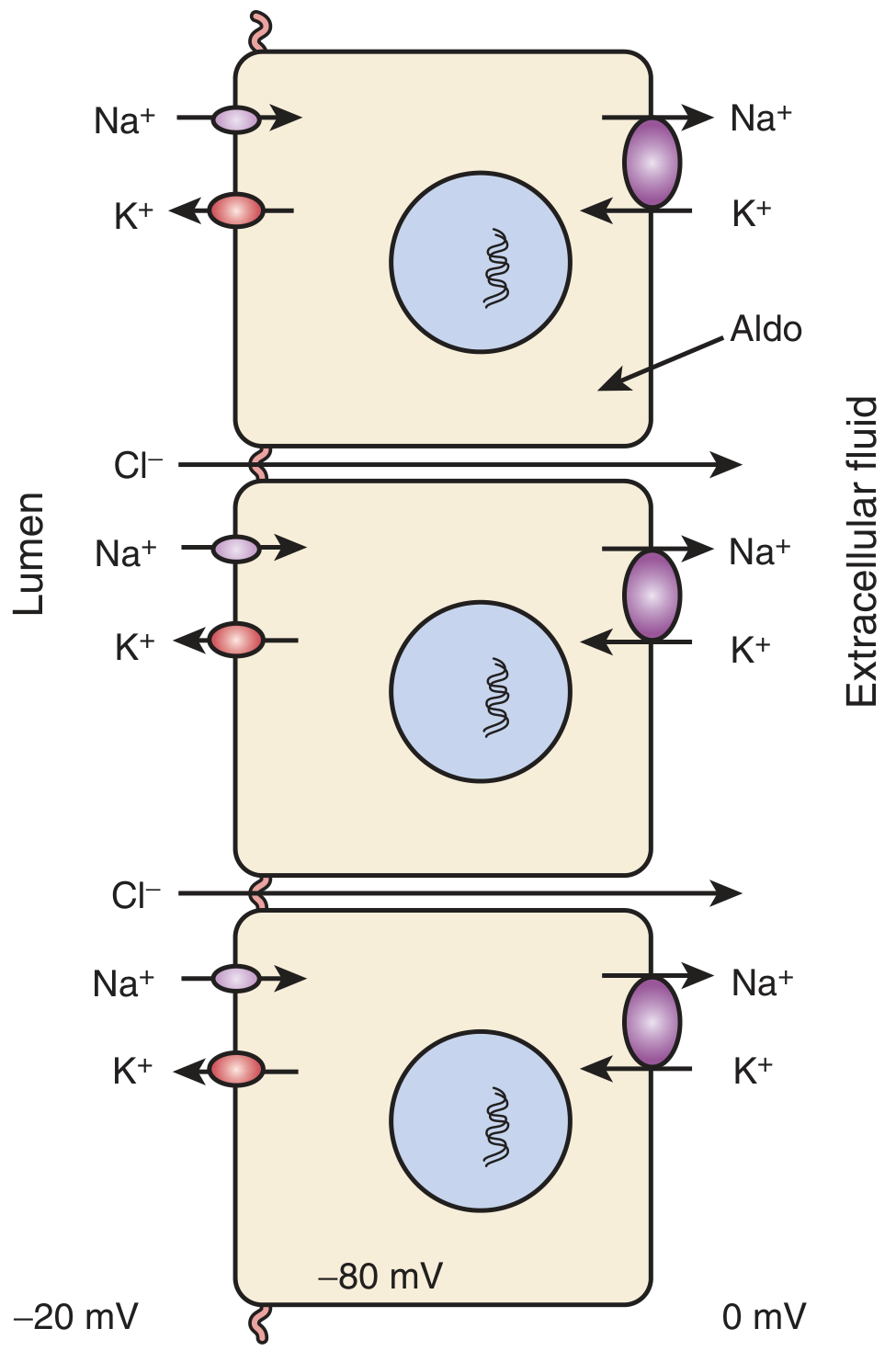
- Na⁺ entry via ENaC creates a lumen-negative electrical potential (−20 mV lumen, −80 mV intracellular, 0 mV extracellular) that drives K⁺ secretion through ROMK and BK channels into the tubular lumen
- Aldosterone acts on ENaC in ASDN to increase the driving force for K⁺ secretion
3. ↑ H⁺ Secretion
- Stimulates H⁺-ATPase in intercalated cells → urinary acid excretion
- Contributes to metabolic alkalosis in aldosterone excess states
4. Water Reabsorption
- Na⁺ reabsorption is accompanied by Cl⁻ reabsorption (paracellular and via pendrin/Cl⁻–HCO₃⁻ exchange) and water follows osmotically → expanded ECF and blood volume
Regulation of Sodium and Potassium Balance
| Stimulus | Aldosterone Response | Net Effect |
|---|---|---|
| Low dietary Na⁺ / low blood pressure | ↑ Aldosterone | ↑ Na⁺ reabsorption → restores ECF volume |
| High plasma K⁺ | ↑ Aldosterone | ↑ K⁺ secretion → normalizes plasma K⁺ |
| Angiotensin II | ↑ Aldosterone | Both of the above |
Extra-Renal / Non-Epithelial Actions
Aldosterone acts beyond the kidney:
- Colon: increases Na⁺ absorption and K⁺ secretion in the distal colon (important when renal function is impaired)
- Salivary & sweat glands: reduces Na⁺ concentration in secretions
- Vascular wall: aldosterone causes rapid rise in intracellular pH via nongenomic mechanisms; at nanomolar concentrations it has vascular effects including vasoconstriction and modulation of vascular tone
- Heart & vasculature (pathophysiologic): excess aldosterone promotes myocardial and vascular fibrosis, atrial fibrillation, and increased risk of myocardial infarction/stroke — effects seen in primary aldosteronism beyond what blood pressure elevation alone would explain
Nongenomic Actions
In addition to the classical genomic mechanism, aldosterone also has rapid nongenomic effects (onset 5–10 min, not blocked by transcription inhibitors):
- Mediated primarily via classical MR in a non-transcriptional fashion (and possibly via non-MR membrane receptors on endothelial cells)
- Include rapid vascular effects (e.g., in response to orthostasis or acute blood volume depletion)
- Blocked by MR antagonist RU 28318
Summary Table of Actions
| Action | Location | Net Effect |
|---|---|---|
| ↑ Na⁺ reabsorption (ENaC ↑, Na⁺-K⁺-ATPase ↑) | Kidney ASDN | ↑ ECF volume, ↑ BP |
| ↑ K⁺ secretion (ROMK, BK channels) | Kidney ASDN | ↓ Plasma K⁺ |
| ↑ H⁺ secretion | Kidney collecting duct | Metabolic alkalosis |
| ↑ Na⁺ absorption | Colon, salivary/sweat glands | ↓ Na⁺ loss in secretions |
| Vascular & cardiac fibrosis | Heart, vessels | Hypertension complications |
| Rapid nongenomic vascular effects | Vascular endothelium | ↑ Vascular tone |
Clinical Correlates
- Primary aldosteronism (Conn syndrome): adenoma or bilateral hyperplasia → hypertension, hypokalemia, metabolic alkalosis, suppressed renin
- Hypoaldosteronism (Addison's disease): salt wasting, hyperkalemia, hypotension
- Aldosterone antagonists (spironolactone, eplerenone): K⁺-sparing diuretics; also used in heart failure to reduce cardiac fibrosis
Sources: Brenner and Rector's The Kidney, 2-Volume Set, Chapter 12; Costanzo Physiology 7th Edition, Chapters 6 & 9.
This is a shared conversation. Sign in to Orris to start your own chat.