Bilalary colic with images in easy to understand way
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I have excellent images and comprehensive content. Now I have everything needed to write a thorough, image-rich, easy-to-understand explanation of biliary colic.
Biliary Colic - A Complete, Easy-to-Understand Guide
What is Biliary Colic?
Biliary colic is the pain you get when a gallstone temporarily blocks the cystic duct (the outlet of the gallbladder). The gallbladder contracts to push bile out, hits the stone, and the resulting pressure buildup causes intense pain. When the stone shifts back into the gallbladder or passes through, the pain stops - that's why the attacks are episodic, not constant.
Despite the word "colic," the pain is usually steady, not wave-like.
The Gallbladder and Its Location
Think of the gallbladder as a small pear-shaped storage bag tucked under your liver on your right side. It stores bile (a digestive juice made by the liver) and squeezes it into your small intestine when you eat - especially fatty food.
LIVER
└── Gallbladder (sits underneath)
└── Cystic duct ──→ Common bile duct ──→ Small intestine
What Are Gallstones?
Gallstones are solid deposits that form when substances in bile (cholesterol or bilirubin salts) crystallize and clump together. About 10-20% of adults in Western countries have them, but 70-80% never get symptoms at all.
Two Main Types
| Cholesterol Stones | Pigment Stones | |
|---|---|---|
| How common | ~80% | ~20% |
| Color | Pale yellow to gray | Black or brown |
| X-ray | Usually invisible (radiolucent) | Usually visible (radiopaque) |
| Who gets them | Obese, female, elderly, pregnant | Chronic hemolysis (sickle cell), liver disease |
Real Gallstones - What They Look Like
Cholesterol gallstones (the most common type):

The photo above shows cholesterol gallstones (brown, faceted) packed inside a real gallbladder. The wall looks thickened because of chronic inflammation. - Robbins & Kumar Basic Pathology
Another example - fewer but larger stones:
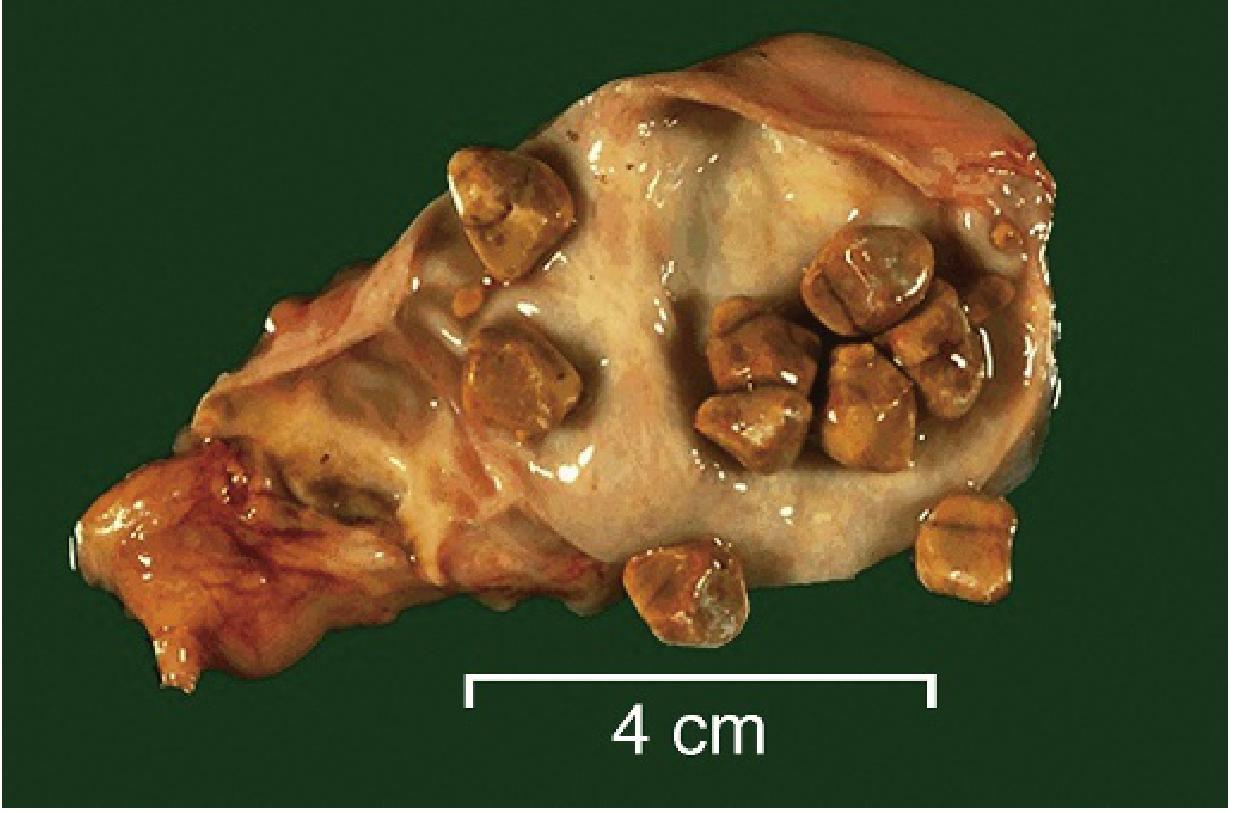
Yellow-tan cholesterol gallstones in the gallbladder. The wall is pale due to scarring. - Robbins & Kumar Basic Pathology
Pigment gallstones (black type - from chronic hemolysis):

Small black pigment stones in the gallbladder of a patient with a mechanical heart valve (causing chronic red blood cell destruction). - Robbins & Kumar Basic Pathology
Risk Factors - The "5 F's" and More
The classic mnemonic is the Five F's:
| Factor | Detail |
|---|---|
| Female | Women have 2x the rate of men |
| Fat (Obese) | Obesity increases cholesterol secretion |
| Forty (Age) | Risk rises with age; >25% after age 80 |
| Fertile (Pregnant) | Estrogen increases biliary cholesterol |
| Fair (Family history) | ~25% of risk is genetic |
Additional risk factors: oral contraceptives, rapid weight loss, diabetes, Crohn's disease, cirrhosis, sickle cell anemia.
How Biliary Colic Happens - Step by Step
- You eat a fatty meal → the gallbladder gets a signal (cholecystokinin) to contract
- A stone lodges in the cystic duct as bile tries to flow out
- Pressure builds inside the gallbladder → visceral pain signals fire (T8/T9 dermatomes)
- You feel severe right upper quadrant or epigastric pain, sometimes radiating to the right shoulder blade
- The stone shifts back into the gallbladder or passes through → pain stops within minutes to hours
- Next attack: could be days, weeks, or even years later
From Yamada's Textbook of Gastroenterology: "Pain is relieved if the stone returns into the gallbladder lumen or passes through the ampulla into the duodenum." - Yamada's Textbook of Gastroenterology, 7th ed.
Symptoms
| Symptom | Detail |
|---|---|
| Pain | Right upper quadrant or epigastric; steady (not wave-like); severe (reaches 9/10 on pain scale) |
| When it starts | Usually 30-60 minutes after eating, especially a heavy or fatty meal |
| Duration | 15 minutes to a few hours, then subsides |
| Radiation | Right shoulder or right shoulder blade (~60% of cases) |
| Nausea/vomiting | Very common |
| Fever | Absent - if fever is present, think cholecystitis or cholangitis |
| Jaundice | Absent - if present, think common bile duct stone (choledocholithiasis) |
| Peak timing | Often around midnight (circadian pattern) |
Key point: No fever + no jaundice + pain resolves within hours = biliary colic (uncomplicated).
Physical Examination
- Mild right upper quadrant tenderness on pressing
- No rebound tenderness, no rigidity (no peritoneal signs)
- Murphy's sign is NEGATIVE in biliary colic (positive Murphy's sign = acute cholecystitis)
- Patient may be distressed during an attack but looks well between attacks
How Is It Diagnosed?
Ultrasound - The Gold Standard
Ultrasound detects gallstones in ~95% of cases. It is cheap, safe, fast, and has no radiation. You must fast for 8 hours beforehand so the gallbladder is distended and full of bile (easier to see stones).
What ultrasound shows:
- Echogenic (bright) stones with "acoustic shadowing" behind them
- Possibly a thickened gallbladder wall if there is associated inflammation
CT Scan
CT is less sensitive for gallstones (~75%) because cholesterol stones are often isodense with bile (invisible). However, CT is excellent for showing complications like gallbladder perforation, emphysematous cholecystitis, or gallstone ileus.
CT scan showing acute cholecystitis (for comparison):

CT showing a stone at the gallbladder neck (arrow) and thickened wall (arrowheads) - this is cholecystitis; in simple biliary colic the wall would not be thickened. - Tintinalli's Emergency Medicine
Blood Tests
In uncomplicated biliary colic, labs are usually normal. If abnormal, consider a complication:
- Elevated WBC → cholecystitis
- Elevated bilirubin/ALP → choledocholithiasis
- Elevated lipase/amylase → gallstone pancreatitis
Biliary Colic vs. Acute Cholecystitis - Key Differences
| Feature | Biliary Colic | Acute Cholecystitis |
|---|---|---|
| Cause | Stone temporarily blocking cystic duct | Stone permanently blocking cystic duct → infection + inflammation |
| Pain duration | Minutes to a few hours | Persists >6 hours, worsening |
| Fever | Absent | Present (but only ~1/3 of cases) |
| Murphy's sign | Negative | Positive (65% sensitive, 87% specific) |
| WBC | Normal | Elevated |
| Ultrasound | Stones only | Stones + thickened wall + pericholecystic fluid |
| Treatment | Outpatient, elective cholecystectomy | Hospitalization, IV antibiotics, early surgery |
Simple rule: If the pain doesn't go away after a few hours - it's no longer just "colic."
Potential Complications if Left Untreated
Gallstones (asymptomatic)
↓ (minority progress)
Biliary Colic (temporary blockage)
↓ (if stone stays stuck)
Acute Cholecystitis (infection + inflammation)
↓ (can lead to)
┌─────────────────────────────────┐
│ Empyema (pus in gallbladder) │
│ Perforation │
│ Gangrene │
│ Cholangitis (bile duct infect.) │
│ Gallstone Pancreatitis │
│ Gallstone Ileus (bowel blockage)│
└─────────────────────────────────┘
Treatment
For Biliary Colic (Emergency Department)
- NSAIDs (first line) - e.g., ketorolac IV/IM. Works as well as opioids and may prevent progression to cholecystitis.
- Opioids - for severe pain when NSAIDs aren't enough. All opioids cause some sphincter of Oddi spasm, but no specific opioid is superior.
- Antiemetics - for nausea and vomiting.
- Anticholinergics (atropine, glycopyrrolate) - do NOT help; not recommended.
- Discharge home once pain is controlled, with outpatient surgical referral.
Definitive Treatment
Laparoscopic cholecystectomy (keyhole removal of the gallbladder) is the definitive cure. It is elective for biliary colic (done as an outpatient or next available slot). Advantages over open surgery:
- Less post-operative pain
- Shorter hospital stay
- Faster return to normal activity
When to operate urgently: If pain does not resolve and cholecystitis develops, early surgery (within 24-48 hours of diagnosis) is now the standard of care - proven by multiple trials to reduce total hospital stay by more than 4 days compared to delayed surgery.
Asymptomatic Gallstones
No treatment needed in most people. Prophylactic cholecystectomy is rarely recommended except in:
- Sickle cell disease
- Pre-organ transplant patients
- Ethnic groups with high gallbladder cancer risk (e.g., certain Native American populations)
Quick Summary Card
| What | Episodic RUQ pain from a gallstone blocking the cystic duct |
| Who | Female, obese, 40s, family history |
| Pain | Steady, severe, 30-60 min post-fatty meal, lasts <6 hours |
| Radiation | Right shoulder blade |
| No fever, no jaundice, no peritoneal signs | |
| Diagnosis | Abdominal ultrasound |
| Acute treatment | NSAIDs + antiemetics |
| Definitive treatment | Laparoscopic cholecystectomy |
Sources: Robbins & Kumar Basic Pathology; Fischer's Mastery of Surgery, 8th ed.; Tintinalli's Emergency Medicine; Yamada's Textbook of Gastroenterology, 7th ed.; Swanson's Family Medicine Review.
This is a shared conversation. Sign in to Orris to start your own chat.