ECG changes
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Searching Images
ECG changes electrocardiogram ST elevation T wave inversion MI ischemia
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content and clear images. Let me compile the full answer.
ECG Changes: A Comprehensive Overview
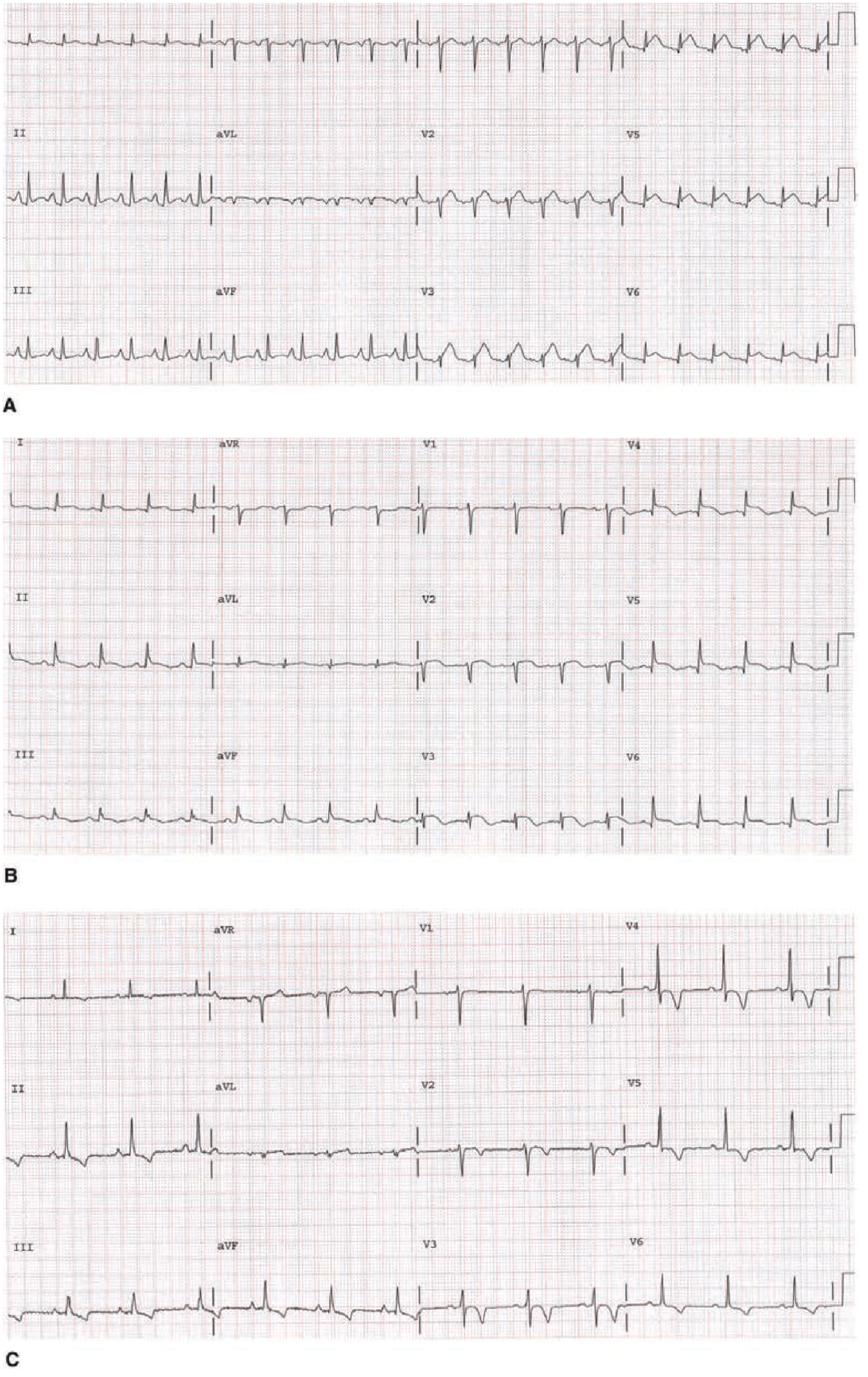
1. Acute Myocardial Infarction (STEMI)
The classic ECG evolution in acute ST-elevation MI passes through three overlapping phases:
Phase 1 — Early Acute (minutes to hours)
- Hyperacute T waves: tall, peaked, widened T waves are the earliest sign — can precede ST elevation
- ST elevation: ST segment evolves from concave → straightened → convex upward ("tombstone" appearance)
- Reciprocal ST depression in leads opposite the infarct zone; associated with larger infarcts and worse prognosis but greater benefit from reperfusion
Phase 2 — Evolved Acute (hours to days)
- ST elevation begins to regress
- T-wave inversion develops in leads with prior ST elevation
- Pathologic Q waves appear (diagnostic of transmural MI)
Phase 3 — Chronic/Stabilized
- Persistent Q waves (often permanent)
- ST segments return to baseline
- T-wave inversions may persist or resolve
"When typical ST-segment elevation persists for hours and is followed within hours to days by T-wave inversions and Q waves, the diagnosis of acute MI can be made with virtual certainty." — Goldman-Cecil Medicine
STEMI diagnostic thresholds:
| Lead | Criteria |
|---|---|
| V2–V3 (men) | ST elevation ≥2 mm at J point |
| V2–V3 (women) | ST elevation ≥1.5 mm |
| All other leads | ST elevation ≥1 mm in ≥2 contiguous leads |
Pathologic Q wave criteria:
- V2–V3: Q wave ≥0.02 s or QS complex
- Other leads: Q wave ≥0.03 s and ≥0.1 mV deep in ≥2 contiguous leads
2. Non-ST-Elevation ACS (NSTEMI / Unstable Angina)
- ST-segment depression (≥0.5 mm) — subendocardial ischemia
- T-wave inversion — may be symmetric and deep (Wellens' pattern in LAD territory = V1–V4)
- "Dynamic" ECG changes — new or worsening ST-T changes vs prior ECG strongly suggest ACS
- A normal ECG does not exclude ACS
3. Pericarditis
Classic four-stage ECG evolution:
| Stage | ECG Finding |
|---|---|
| I | Diffuse ST elevation (saddle-shaped/concave) + PR depression in I, II, III, aVF; PR elevation in aVR |
| II | ST returns to baseline; T waves flatten |
| III | Diffuse T-wave inversion |
| IV | Normalization |
Distinguishing pericarditis from STEMI:
- ST elevation in pericarditis is diffuse (not territory-specific) and concave
- PR depression is characteristic of pericarditis (not STEMI)
- No reciprocal ST depression (except aVR/V1)
- ST:T-wave ratio in V6 >0.25 favors pericarditis over early repolarization
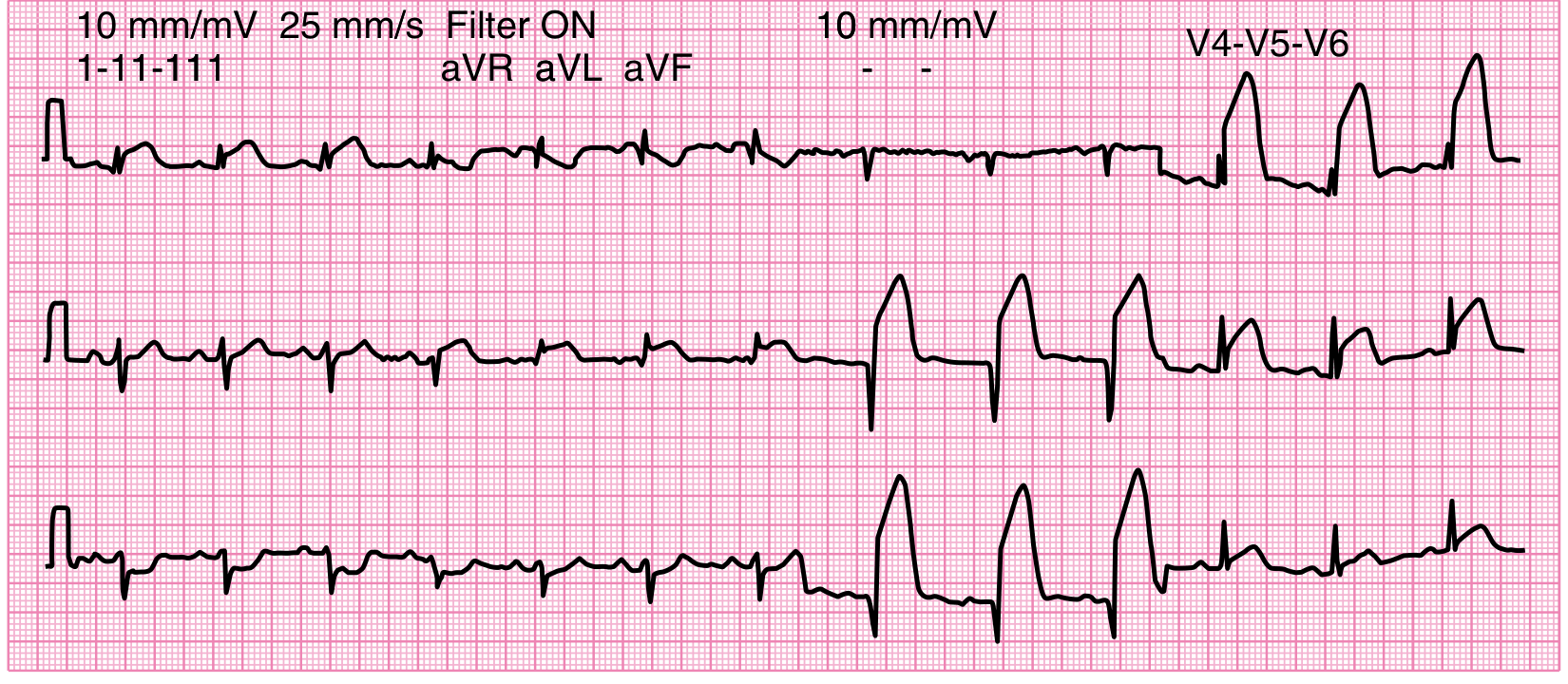
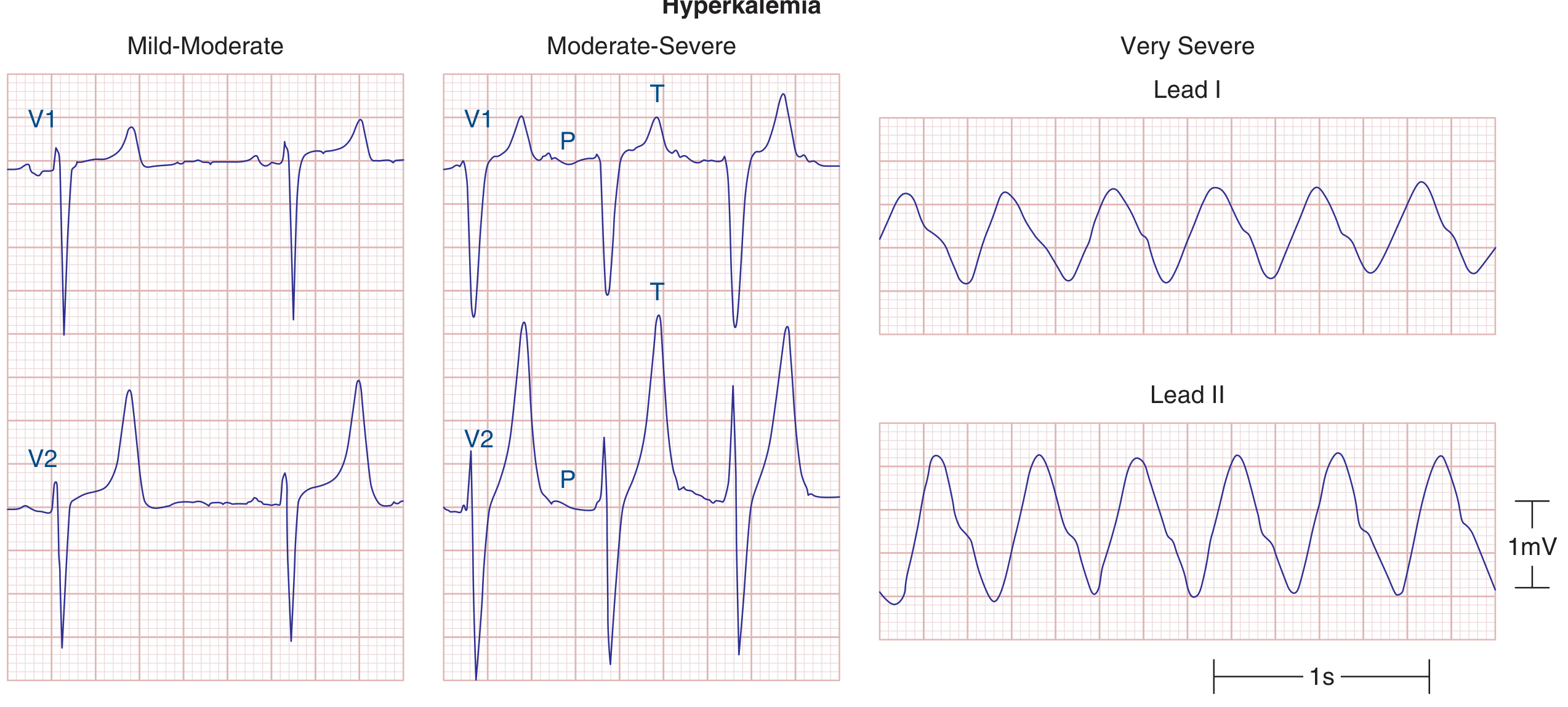
4. Electrolyte Abnormalities
Hyperkalemia (progressive sequence):
- Peaked (tented) T waves — narrow, tall, symmetric (earliest change)
- Prolonged PR interval, diminished P-wave amplitude
- Widened QRS
- Sine-wave pattern → asystole
Hypokalemia:
- Prolonged ventricular repolarization
- Prominent U waves (most characteristic)
- Flattened or inverted T waves
- Prolonged QU interval (often mistaken for QT prolongation)
Hypocalcemia:
- Prolonged QT interval (prolonged ST segment specifically)
Hypercalcemia:
- Shortened QT interval
5. Drug-Induced ECG Changes
| Drug/Class | ECG Effect |
|---|---|
| Digoxin | "Scooping" of ST-T complex; shortened QT; PR prolongation |
| Class IA (quinidine, procainamide) | QT prolongation; wide QRS |
| Class III (amiodarone, sotalol) | QT prolongation |
| TCAs, phenothiazines | QT prolongation; wide QRS |
| Cocaine | ST elevation (vasospasm) |
6. Pulmonary Embolism
Classic (but insensitive/non-specific) pattern:
- S1Q3T3: deep S in I, Q wave + T inversion in III
- Right heart strain: sinus tachycardia, RBBB, T inversion in V1–V4
- Right axis deviation
- Most common finding is simply sinus tachycardia or a non-specific change
7. Left Ventricular Hypertrophy (LVH)
- High-voltage QRS (tall R in V5–V6, deep S in V1–V2)
- "Strain" pattern: ST depression + T inversion in lateral leads (I, aVL, V5–V6)
- Can mimic ischemia
8. Bundle Branch Blocks
| Block | QRS | Key Features |
|---|---|---|
| LBBB | ≥120 ms | Broad notched R in V5–V6, I, aVL; deep S in V1 |
| RBBB | ≥120 ms | RSR' ("rabbit ears") in V1–V2; broad S in I, V5–V6 |
New LBBB in the setting of chest pain may represent STEMI equivalent; use Sgarbossa criteria:
- ST elevation ≥1 mm concordant with QRS → 5 pts
- ST depression ≥1 mm in V1–V3 → 3 pts
- ST elevation ≥5 mm discordant with QRS → 2 pts (≥3 pts = STEMI likely)
9. Other Notable Changes
| Condition | ECG Finding |
|---|---|
| Hypothermia | Osborn (J) waves (convex hump at J point); bradycardia; prolonged intervals |
| Subarachnoid hemorrhage | Deeply inverted, wide T waves ("CVA T waves"); prolonged QT |
| Brugada syndrome | Coved ST elevation in V1–V2; RBBB morphology |
| Cardiac tamponade | Electrical alternans (P-QRS-T beat-to-beat alternation) + sinus tachycardia + low voltage |
| Pericardial/pleural effusion | Low QRS voltage |
| Posterior MI | Tall R + ST depression in V1–V2; confirmed with posterior leads V7–V9 |
Differential Diagnosis of ST Elevation (Non-STEMI Causes)
| Cardiac | Other |
|---|---|
| Prior MI with aneurysm | Pulmonary embolism |
| Pericarditis/myocarditis | Hyperkalemia |
| LVH/aortic stenosis (strain) | |
| Hypertrophic cardiomyopathy | |
| Coronary vasospasm / Prinzmetal | |
| Early repolarization (normal variant) | |
| Brugada syndrome |
(Washington Manual of Medical Therapeutics; Goldman-Cecil Medicine)
Sources: Goldman-Cecil Medicine (9780323930345) | Harrison's Principles of Internal Medicine 22E (9781265977061) | Tintinalli's Emergency Medicine (9781260019933) | Washington Manual of Medical Therapeutics (9781975190620) | Swanson's Family Medicine Review (9780323698115)
This is a shared conversation. Sign in to Orris to start your own chat.