Blood clotting condition in living body
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have rich, comprehensive content. Let me compile the full answer.
Thrombosis — Blood Clotting in a Living Body
Thrombosis is the formation of a blood clot (thrombus) within the vascular system of a living organism. Unlike normal hemostatic clotting (which stops bleeding after injury), thrombosis occurs pathologically within intact or mildly injured vessels and can obstruct blood flow, with potentially fatal consequences.
Virchow's Triad — The Three Core Causes
Three primary abnormalities predispose to thrombosis, collectively known as Virchow's Triad:
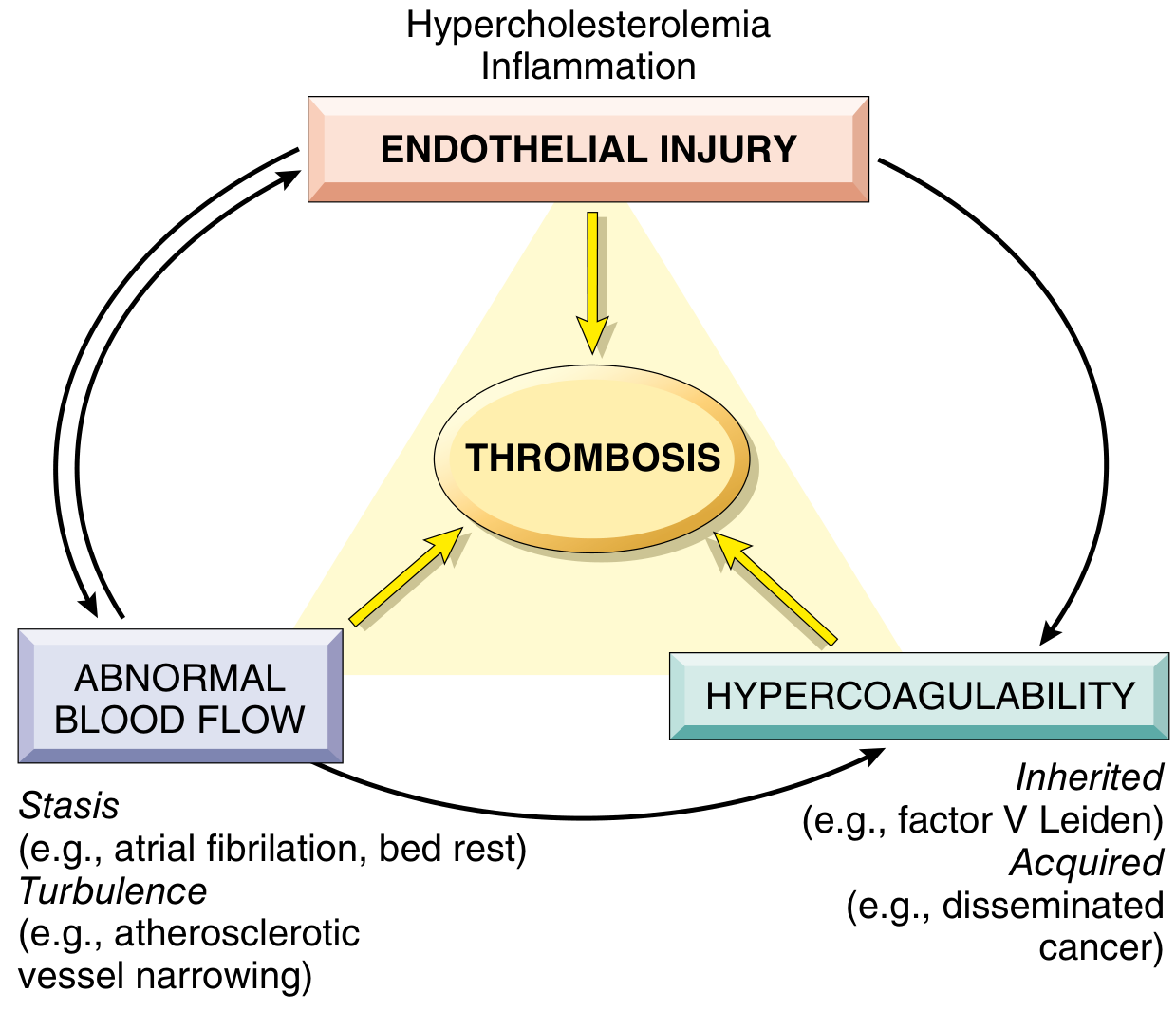
1. Endothelial Injury
- The most important factor, especially in the heart and arterial circulation where high blood flow rates otherwise prevent clotting.
- Severe injury exposes von Willebrand factor (vWF) and tissue factor, triggering platelet adhesion and the coagulation cascade.
- Even without direct injury, endothelial activation/dysfunction (caused by infection, inflammation, hypercholesterolemia, homocystinemia, or cigarette toxins) shifts endothelial gene expression to a prothrombotic state:
- Downregulates thrombomodulin, protein C, and tissue factor pathway inhibitor (anticoagulants)
- Increases secretion of plasminogen activator inhibitors (PAI), which suppress fibrinolysis
- Arterial and cardiac thrombi are typically platelet-rich ("white thrombus") — hence aspirin and platelet inhibitors are used in CAD and MI.
2. Abnormal Blood Flow (Stasis or Turbulence)
- Turbulence contributes to arterial/cardiac thrombosis by damaging the endothelium and creating local pockets of stasis.
- Stasis is the major driver of venous thrombosis (DVT). Stasis:
- Promotes endothelial activation and procoagulant activity
- Allows platelets and leukocytes to contact the endothelium
- Prevents dilution of activated clotting factors by fresh blood and inhibits inflow of regulatory proteins (protein C, antithrombin)
Clinical examples of stasis/turbulence: atrial fibrillation, prolonged bed rest, atherosclerotic vessel narrowing, aortic/arterial aneurysms, mitral valve stenosis, hyperviscosity (polycythemia).
3. Hypercoagulability of the Blood
An increased tendency of blood to clot, divided into:
| Type | Examples |
|---|---|
| Inherited (primary) | Factor V Leiden mutation (most common), prothrombin G20210A mutation, antithrombin III deficiency, protein C or S deficiency |
| Acquired (secondary) | Prolonged bed rest/immobility, MI, atrial fibrillation, cancer (Trousseau syndrome), late pregnancy/OCP use, heparin-induced thrombocytopenia (HIT), antiphospholipid syndrome |
Morphology of Thrombi
| Feature | Arterial/Cardiac | Venous |
|---|---|---|
| Composition | Platelet-rich ("white") | RBC-rich ("red") |
| Location | Sites of turbulence/injury (e.g., atherosclerotic plaques) | Areas of stasis (deep veins of legs) |
| Attachment | Firmly attached, often occlusive or mural | Tend to be occlusive |
| Lines of Zahn | Present (alternating layers of platelets/fibrin + RBCs) — indicates formation in flowing blood | Absent |
Thrombi that form post-mortem have no lines of Zahn (gelatinous, not firmly attached) — this distinguishes them from antemortem thrombi at autopsy.
Fate of a Thrombus
Once formed, a thrombus can undergo:
- Propagation — enlarge and eventually occlude the vessel
- Embolization — detach and travel to distant sites (e.g., DVT → pulmonary embolism)
- Dissolution (fibrinolysis) — broken down by plasmin; most effective when thrombus is fresh (basis of tPA therapy in acute MI/stroke)
- Organization and recanalization — older thrombi are invaded by endothelial cells and smooth muscle, forming small channels that restore some blood flow
Key Complications
Deep Vein Thrombosis (DVT) → Pulmonary Embolism (PE)
- 70–80% of pulmonary emboli originate from leg DVT
- PE incidence: ~60–120 cases per 100,000/year in the US; causes 60,000–100,000 deaths/year
- A thrombus passing through the right heart lodges in the pulmonary arterial tree
- Small PE: often silent, organizes and incorporates into vessel wall
- Large PE (>60% obstruction): sudden death, acute cor pulmonale, or cardiovascular collapse
Systemic (Arterial) Thromboembolism
- 80% arise from intracardiac mural thrombi (left ventricular infarcts, left atrial dilation in AF)
- Most lodge in the lower extremities (75%) or brain (10%)
- Brain: stroke; intestine: ischemic colitis; kidneys: renal infarct
Disseminated Intravascular Coagulation (DIC)
- Widespread activation of coagulation throughout the microcirculation
- Paradoxically causes both microthrombi (organ ischemia) and consumption coagulopathy → bleeding
- Triggers: sepsis, severe trauma, obstetric complications, disseminated cancer
Summary
Thrombosis is the pathological activation of the same hemostatic mechanisms that normally protect against bleeding. The key insight is that endothelial integrity is the central safeguard — its disruption or dysfunction, combined with stasis or hypercoagulability, tips the balance irreversibly toward clot formation. The consequences — stroke, MI, PE, DVT — are among the leading causes of death worldwide.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease — pp. 126–131; Robbins & Kumar Basic Pathology — pp. 2493–2540
Blood clotting condition in heart attack
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive content for a thorough answer. Let me compile it.
Blood Clotting in a Heart Attack (Myocardial Infarction)
A heart attack (acute myocardial infarction, AMI) is fundamentally a thrombotic event — specifically, the sudden formation of a blood clot inside a coronary artery that cuts off blood supply to heart muscle. There are actually two distinct phases of clotting in the context of MI: the coronary thrombosis that causes the MI, and the mural (intracavitary) thrombus that forms after the MI.
Phase 1 — Coronary Thrombosis: The Cause of the Heart Attack
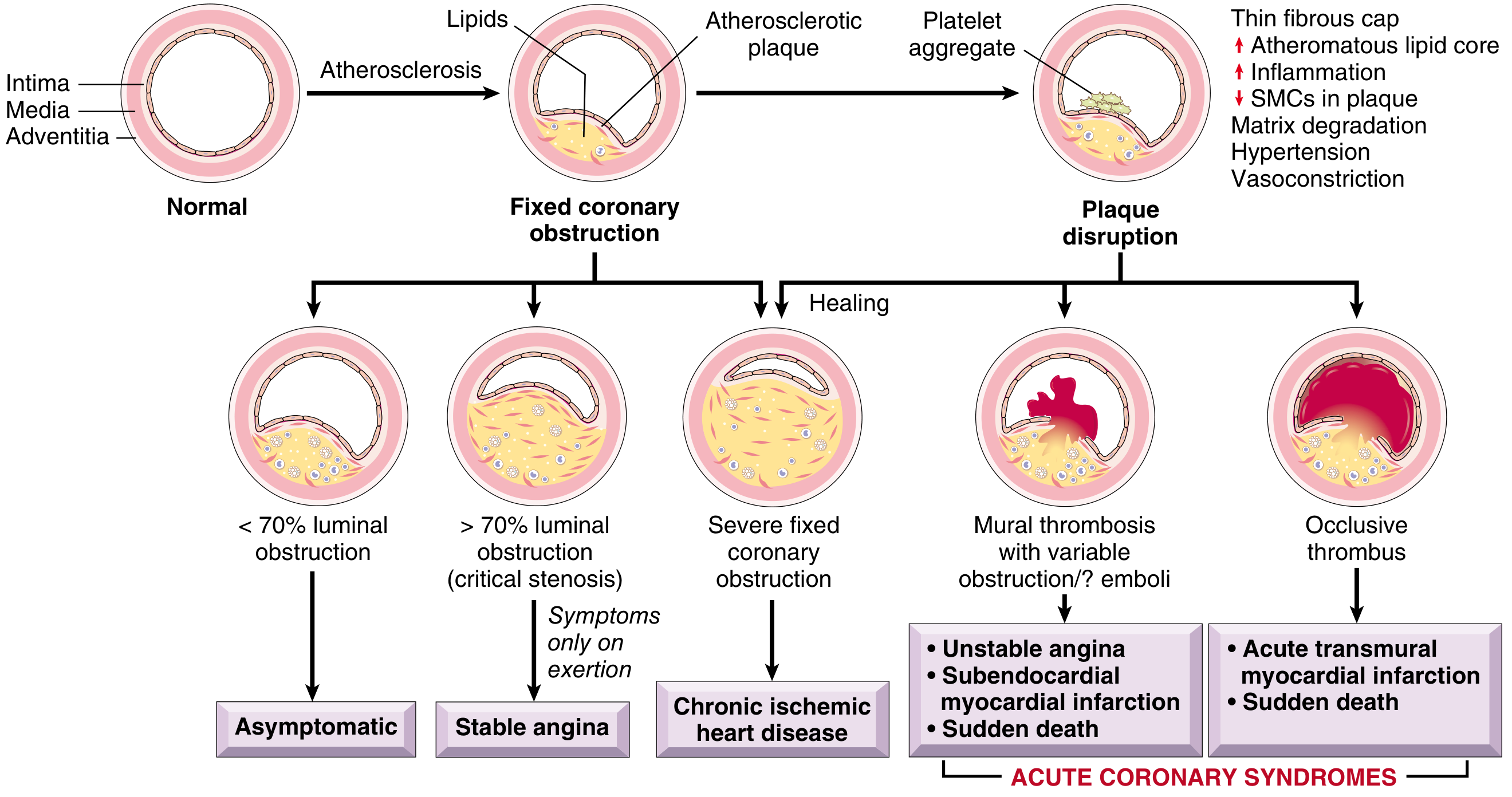
The Trigger: Atherosclerotic Plaque Disruption
Most MIs begin with a sudden disruption of a coronary artery atherosclerotic plaque — not necessarily a plaque that was severely narrowing the artery beforehand. The culprit lesion is often not critically stenotic or even symptomatic before rupture, making many asymptomatic adults at significant risk for a catastrophic event.
There are three forms of plaque disruption:
| Mechanism | Frequency | Details |
|---|---|---|
| Plaque rupture | ~65% of cases | Thin fibrous cap tears, exposing the lipid-rich necrotic core |
| Plaque erosion | ~30% of cases | Endothelial cell loss/apoptosis without full rupture |
| Calcified nodule | <5% of cases | Nodular calcification protrudes through the cap |
Why Plaques Rupture — The "Vulnerable Plaque"
A plaque is vulnerable to rupture when it has:
- A large lipid-rich atheromatous core
- A thin overlying fibrous cap (thin-cap fibroatheroma, TCFA)
- Heavy macrophage infiltration — macrophages secrete metalloproteinases that degrade the collagen maintaining cap integrity
- Few smooth muscle cells — SMCs are needed to synthesize new collagen
- Fissuring typically occurs at the junction of the fibrous cap and normal arterial wall where mechanical stress is greatest
Extrinsic factors also contribute: elevated blood pressure, platelet reactivity, adrenergic surges (e.g., early morning, physical exertion, emotional stress).
How the Clot Forms After Plaque Rupture
Once the plaque ruptures or erodes:
- Exposure of collagen, vWF, and tissue factor in the subendothelium
- Platelet adhesion → platelet activation → platelet aggregation (platelet plug = "white thrombus")
- Coagulation cascade activation via tissue factor → thrombin generation → fibrin cross-linking
- Rapid formation of a platelet-rich thrombus superimposed on the plaque
The degree of luminal obstruction determines the clinical outcome:
| Thrombus | Obstruction | Clinical Result |
|---|---|---|
| Partial/mural thrombus | Incomplete | Unstable angina / NSTEMI (subendocardial infarct) |
| Complete occlusion | Total | STEMI (transmural MI), sudden death |
"In most patients, unstable angina, infarction, and sudden cardiac death occur because of abrupt plaque change followed by thrombosis — hence the term acute coronary syndrome." — Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 510
Where in the Heart Does It Happen?
The three major epicardial coronary arteries and their infarct territories:
| Artery | Frequency | Infarct Territory |
|---|---|---|
| Left Anterior Descending (LAD) | 40–50% | Anterior LV wall, anterior septum, apex |
| Right Coronary Artery (RCA) | 30–40% | Inferior/posterior LV wall, posterior septum |
| Left Circumflex (LCX) | 15–20% | Lateral LV wall |
Plaques tend to cluster in the first few centimeters of the LAD and LCX — these are the highest-risk segments.
Types of Myocardial Infarction Based on Clot
| Type | Mechanism | Morphology |
|---|---|---|
| STEMI (Transmural MI) | Complete coronary occlusion by thrombus | Full-thickness necrosis across LV wall |
| NSTEMI (Subendocardial MI) | Partial occlusion, or thrombus that lyses spontaneously/therapeutically | Necrosis limited to innermost zone of myocardium |
| Microinfarction | Small emboli from the thrombus, vasospasm, or vasculitis | Scattered focal necrosis in intramural vessels |
Phase 2 — Mural Thrombus: A Complication AFTER MI
Once the myocardium is infarcted (dead), a second clot can form inside the heart chamber itself:
- Large anterior MI with reduced left ventricular ejection fraction and apical wall-motion abnormality → blood pools and stagnates over the damaged, dyskinetic wall
- The inflamed, injured endocardium over the necrotic zone is prothrombotic
- A mural (intracavitary) thrombus forms on the inner wall of the left ventricle
- Within 4 weeks of acute MI, ~2.5% of patients suffer a stroke from embolization of this thrombus to the brain
Detection: Contrast-enhanced echocardiography; cardiac MRI (most sensitive)
Treatment: Anticoagulation for 3–6 months (warfarin or DOAC)
Complications of the Clotting Process
| Complication | Mechanism |
|---|---|
| Systemic embolism/stroke | Mural thrombus fragments embolize to brain, limbs, gut |
| Coronary re-thrombosis | Re-occlusion after spontaneous or therapeutic thrombolysis |
| Ventricular aneurysm | Thinned infarcted wall bulges → stagnation → thrombus |
| Pericarditis | Inflammation of pericardium over necrotic zone |
| Arrhythmia, cardiac rupture, CHF | Direct ischemic complications |
Treatment Targeting the Clot
| Drug Class | Examples | Target |
|---|---|---|
| Antiplatelet | Aspirin, clopidogrel, ticagrelor, prasugrel | Platelet aggregation (thromboxane A2, P2Y12 pathway) |
| Anticoagulants (acute) | Heparin (UFH/LMWH), fondaparinux, bivalirudin | Coagulation cascade (thrombin/Xa) |
| Fibrinolytics (thrombolytics) | tPA (alteplase), streptokinase | Dissolve existing fibrin clot |
| Statins | Atorvastatin, rosuvastatin | Stabilize plaques, reduce inflammation, lower LDL |
| Long-term anticoagulation | Warfarin, apixaban | Mural thrombus post-MI, AF |
| Mechanical | PCI (stenting), CABG | Physically restore lumen patency |
Key insight from statins: They may benefit not just by lowering cholesterol, but by reducing plaque inflammation and stabilizing the fibrous cap, making it less likely to rupture.
Summary
In a heart attack, clotting occurs in two dangerous ways:
- Coronary thrombosis — a plaque in the coronary artery ruptures, platelets and fibrin rapidly clot over the exposed core, and the artery occludes, starving the heart muscle of oxygen → causes the MI
- Mural thrombus — after the MI, blood stagnates over the dead, dyskinetic wall → clot forms inside the heart chamber → can embolize and cause a stroke
Both are driven by the same fundamental triad: endothelial injury + abnormal flow + hypercoagulability — but acting at different locations and timescales.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease — pp. 509–515; Fuster & Hurst's The Heart, 15th Ed. — Ch. 16, pp. 534–547; Robbins & Kumar Basic Pathology — pp. 430–434
TVD hart aatck CONDITION M SURGERY KERNA SAFE H YA NEHI
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Ab mere paas bahut comprehensive information hai. Poora jawab deta hoon — Urdu/Hindi mein aur medical detail ke saath.
Triple Vessel Disease (TVD) — Heart Attack ke Baad Surgery Safe Hai Ya Nahi?
⚠️ Zaroori baat: Yeh medical education ke liye information hai. Har patient ki condition alag hoti hai — final faisla sirf aapke cardiologist aur cardiac surgeon karenge.
TVD Kya Hota Hai?
Triple Vessel Disease (TVD) matlab dil ki teenon badi coronary arteries mein blockage:
- LAD — Left Anterior Descending (sabse important)
- LCX — Left Circumflex
- RCA — Right Coronary Artery
Jab teeno mein blockage ho aur upar se heart attack bhi aa jaye — yeh ek bahut serious condition hai.
Surgery (CABG) Ka Faisla Kab Aur Kaise Hota Hai?
✅ TVD Mein CABG (Bypass Surgery) Prefer Kyun Ki Jaati Hai?
Dunia ke sabse bade clinical trial SYNTAX Trial (1800 patients, TVD ya left main disease) ke mutabiq:
"Patients with the most extensive three-vessel coronary artery disease — CABG gives better long-term outcomes than PCI (stenting)." — Harrison's Internal Medicine 22E
| Factor | CABG (Bypass) | PCI (Stent) |
|---|---|---|
| TVD mein long-term survival | Behtar | Kamtar |
| Repeat procedure ki zaroorat | Kam | Zyada (13.5% vs 5.9%) |
| Diabetes + TVD | CABG clearly better | Inferior |
| Stroke risk (surgery ke waqt) | Thoda zyada | Kam |
Heart Attack (Acute MI) Ki Condition Mein Surgery — Timing Bahut Zaroori Hai
Yahan "kab surgery karo" bahut important sawal hai:
🚨 Situation 1: STEMI (Full Blockage) + TVD
Pehla qadam: Culprit artery (jo artery band hui) ko PCI se kholo
- Jis artery ne heart attack kiya — pehle usse stent se immediately khola jata hai (primary PCI)
- Baaki do arteries (non-culprit) ka baad mein plan banta hai
Sabiston Surgery Textbook ke mutabiq:
"In STEMI patients with complex multivessel CAD, elective CABG is a viable choice AFTER successful PCI of the culprit artery, provided patient is a CABG candidate."
🔴 Situation 2: Cardiogenic Shock (Heart Fail Ho Raha Ho)
- Agar dil ka pump bahut kamzor ho gaya (cardiogenic shock) → pehle culprit artery ki PCI
- Sabiston ke mutabiq: Shock mein immediate complete multivessel surgery potentially harmful ho sakti hai
- Pehle stabilize karo, phir CABG plan karo
🟡 Situation 3: NSTE-ACS (Partial Blockage) + TVD
- High-risk patients mein 24 ghante ke andar invasive strategy (angiography) karo
- Revascularization ka faisla angiography results aur GRACE score ke hisab se hota hai
Surgery Ke Risks — Honest Assessment
| Risk Factor | Surgery Ka Risk Badhata Hai |
|---|---|
| Acute/recent MI (fresh heart attack) | ✅ Haan — zyada risk |
| Cardiogenic shock | ✅ Bahut zyada risk |
| Low ejection fraction (<35%) | ✅ Zyada risk |
| Diabetes | Surgery still preferred over stent |
| Umar (budhaapa) | Risk badhta hai |
| Kidney disease | Risk badhta hai |
| Emergency surgery vs elective | Emergency mein zyada risk |
Safe Hai Ya Nahi — Direct Jawab
| Condition | Recommendation |
|---|---|
| Stable TVD, no active MI | ✅ CABG safe aur preferred — elective surgery |
| TVD + recent MI, stable | ✅ CABG after few days stabilization — safer |
| TVD + STEMI (active) | ⚡ Pehle culprit artery PCI → phir elective CABG |
| TVD + Cardiogenic Shock | 🔴 Emergency PCI of culprit first, CABG baad mein |
| TVD + Diabetes | ✅ CABG strongly preferred over stenting |
| TVD + Left Main disease | ✅ CABG strongly recommended |
Summary — Seedha Jawab
TVD mein bypass surgery (CABG) generally safe aur scientifically recommended hai — khaas kar jab:
- Teeno arteries mein severe disease ho
- Diabetes bhi ho
- Left main artery bhi involved ho
Lekin active heart attack ki condition mein surgery ka timing critical hai:
- Pehle emergency mein culprit artery ko stent se kholo
- Patient stable ho jaye
- Phir Heart Team (cardiologist + cardiac surgeon) milke CABG ka plan banao
"Elective CABG after acute MI stabilization = Safe aur better long-term outcomes"
"Emergency CABG in active cardiogenic shock = High risk"
📚 Sources: Sabiston Textbook of Surgery — Ch. 111; Harrison's Internal Medicine 22E — Ch. 284; Fuster & Hurst's The Heart 15th Ed.⚕️ Aapke ya aapke kisi apne ke case mein — cardiologist se milein, angiography report dikhayein, aur Heart Team se discuss karein. Yahi sabse sahi approach hai.
TVD hart aatck CONDITION and second heart attack SURGERY KERNA SAFE H YA NEHI
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Ab mere paas bahut comprehensive aur specific information hai. Poora detailed jawab deta hoon.
TVD + Pehla Heart Attack + Doosra Heart Attack — Surgery (CABG) Safe Hai Ya Nahi?
⚠️ Zaroori disclaimer: Yeh medical education information hai. Har patient alag hota hai — asli faisla sirf qualified cardiologist + cardiac surgeon ki team karti hai jo patient ko personally dekhe, tests kare, aur sab factors weigh kare.
Samajhna Zaroori Hai: "Doosre Heart Attack" Mein Situation
Jab TVD ke patient ko doosra heart attack aata hai, to condition mein kai cheezein hoti hain:
| Factor | Matlab |
|---|---|
| Pehle MI se dil ka kuch hissa pehle se damage hai | LV function kamzor hoga |
| Doosre MI se aur heart muscle mar gayi | EF (ejection fraction) aur neeche gir sakti hai |
| Teeno arteries mein blockage (TVD) | Bachti hui zindagi heart muscle bhi khatre mein |
| Doosra MI fresh/active hai | Inflammation, unstable plaque, clot abhi bhi active |
Seedha Jawab — Safe Hai Ya Nahi?
🔴 Active (Fresh) Doosre Heart Attack Ke Dauraan — Surgery HIGH RISK Hai
Jab doosra heart attack abhi ho raha ho (acute STEMI/NSTEMI):
- Emergency mein turant surgery (CABG) nahi karte — yeh bahut khatra hai
- Sabse pehle PCI (stent) se culprit artery (jo doosra attack la rahi hai) kholi jaati hai
- Sabiston Surgery ke mutabiq:
"In STEMI patients with multivessel disease and cardiogenic shock — prompt PCI of the culprit vessel is the recommended strategy. Immediate complete multivessel surgery shows no benefit and potential HARM."
🟡 Doosra Heart Attack Ke Baad Stabilize Hone Par — CABG Plan Banta Hai
Jab emergency guzar jaaye, marz stable ho — tab CABG ka assessment hota hai:
CABG strongly recommended hota hai jab:
| Condition | Guideline Recommendation |
|---|---|
| TVD (3 artery blockage) + low EF ≤35% | COR 1 (Strongly Recommended) — CABG |
| TVD + Diabetes | CABG preferred over PCI |
| TVD + proximal LAD involvement | CABG strongly preferred |
| Arrhythmia (VF/VT) bhi ho | CABG recommended for survival |
| Doosre MI ke baad viable (zinda) heart muscle ho | CABG se significant benefit |
"CABG is associated with improved odds of survival in multivessel disease patients with severe LV dysfunction (EF ≤35%)" — Sabiston Textbook of Surgery (2021 ACC/AHA Guidelines)
🔑 Sabse Important Factor: Heart Muscle Zinda Hai Ya Nahi (Viability)
Do baar heart attack aane ke baad yeh test sabse zaroori hai:
Myocardial Viability Testing (MRI ya Nuclear scan)
| Result | Matlab | CABG Ka Fayda |
|---|---|---|
| Viable (hibernating) muscle | Dil ki muscle dormant hai, mari nahi | ✅ CABG se bahut fayda — function wapas aa sakta hai |
| Non-viable (scarred/dead) | Muscle puri tarah mar gayi (scar tissue) | ❌ CABG se koi fayda nahi |
Schwartz Surgery Textbook ke mutabiq:
"An 80% reduction in mortality in patients who underwent revascularization WITH viable myocardium vs. medical therapy alone (3.2% vs. 16%)." "CABG had NO benefit over medical therapy for patients WITHOUT viable myocardium."
Yani: Agar viability test positive aaye — surgery life-saving hai. Agar sab kuch scar hai — surgery ka koi fayda nahi, balki risk badhta hai.
Doosre MI Ke Baad CABG Ke Risks Jo Badhte Hain
| Risk Factor | Kya Hota Hai |
|---|---|
| Kam EF (Ejection Fraction) | Dil ka pump kamzor → surgery se dil aur thak sakta hai |
| LV bada ho gaya (dilated) | EDD >100 mL/m² → 5-year survival drastically girta hai |
| LV dyssynchrony | Dil ki deewarein ek saath nahi chalti → 30-day mortality 27% tak |
| Coronary vessels ki quality kharab | Poor distal vessels → CABG ka koi fayda nahi, mortality 100% |
| Cardiogenic shock | Blood pressure bahut gir gaya → surgery almost impossible safely |
| Umar, kidney disease, diabetes complications | Har cheez risk badhati hai |
STICH Trial — Scientific Proof (Doosra MI + Low EF Mein CABG)
STICH Trial — specifically ischemic heart disease + low EF (≤35%) mein CABG ka study:
- Short term: CABG vs medicines mein koi difference nahi tha
- 10 saal baad: CABG group mein cardiovascular deaths kum + hospitalizations kum
- Natija: Long term mein CABG clearly better — lekin patient selection zaroori hai
Practical Summary — Step by Step Kya Hota Hai
DOOSRA HEART ATTACK AA GAYA
↓
EMERGENCY: Culprit artery ka PCI (stent) → blood flow restore karo
↓
Patient stabilize ho — 24-72 ghante observe karo
↓
Echocardiography → EF check karo
↓
Angiography → teeno arteries ki anatomy dekho
↓
VIABILITY TEST (MRI/Nuclear) → kita dil zinda hai?
↓
Heart Team discussion (Cardiologist + Cardiac Surgeon)
↓
[Viable muscle + TVD] [No viable muscle]
CABG — Life saving Medical therapy only
Elective in stable patient CABG se koi fayda nahi
Final Summary — 3 Points Mein
-
Doosre active heart attack mein turant surgery nahi — pehle stent se emergency manage karo, phir stabilize karo
-
Stabilize hone ke baad TVD mein CABG scientifically best option hai — especially agar EF low ho, diabetes ho, ya teeno arteries mein severe blockage ho
-
Viability test zaroori hai — agar dil ki muscle zinda hai, CABG se survival dramatically behtar hoti hai; agar sab scar hai, surgery ka koi fayda nahi
📚 Sources: Sabiston Textbook of Surgery — Ch. 111 (2021 ACC/AHA Guidelines); Schwartz's Principles of Surgery 11E — CABG for Ischemic Cardiomyopathy; Harrison's Internal Medicine 22E — Surgical Therapy in Heart Failure; STICH Trial data🏥 Aap ya aapka koi relative is situation mein hai to — foran cardiologist se milein. Echocardiography aur viability testing karwayein. Yeh faisla Heart Team kare — akele koi ek doctor nahi karta.
This is a shared conversation. Sign in to Orris to start your own chat.