Tonsil surgery steps by steps with proper instrument name and use
Reading File
Finding Sources
Finding Sources
Searching the Web
tonsillectomy surgical steps instruments dissection technique
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK536942
I now have comprehensive information from multiple authoritative sources. Let me compile the full, detailed answer.
Tonsillectomy - Step-by-Step Surgical Guide with Instruments
Tonsillectomy is one of the most commonly performed ENT operations. It can be done by cold steel dissection (most traditional), hot/diathermy technique (most common in the US), or newer methods like Coblation. Below is the full procedure for the standard cold steel dissection and snare technique, followed by the hot/diathermy variant.
Pre-operative Setup
Patient Position: Supine, with a shoulder roll placed to extend the neck and bring the oropharynx into view. The operating table is rotated 45-180° so the surgeon sits or stands at the head of the bed.
Anesthesia: General anaesthesia with oral intubation. An oral RAE (Ring-Adair-Elwyn) endotracheal tube is preferred - it curves away from the mouth, keeping the surgical field clear. The tube is taped at the midline.
Instruments List (Cold Steel Tonsillectomy)
| Instrument | Purpose |
|---|---|
| Crowe-Davis or McIvor mouth gag | Opens and maintains the mouth in the open position; has a tongue blade that depresses the tongue and holds the ETT groove |
| Boyle-Davis mouth gag | Alternative gag with integrated tongue depressor |
| Wieder tongue depressor/retractor | Retracts the tongue; improves visualization of the oropharynx |
| Allis clamp | Grasps and medializes the tonsil during dissection |
| White tonsil clamp | Curved Allis-type clamp for grasping tonsil tissue |
| No. 7 knife handle + No. 12 blade | Makes the initial mucosal incision along the anterior pillar |
| Fisher tonsil knife and dissector | Dissects the tonsil from its capsule in the avascular plane |
| Hurd dissector and pillar retractor | Blunt dissection of the peritonsillar space + retracts the anterior pillar out of the way |
| Curved Metzenbaum scissors | Identifies and extends the avascular plane between capsule and pharyngeal muscles |
| Tonsil wire snare (Tyding snare) | Loop placed around the inferior pole to amputate the tonsil pedicle |
| Schmidt tonsil forceps | Holds and passes ligatures for hemostasis |
| Foerster-Ballenger sponge-holding forceps | Holds tonsil swabs/pledgets for pressure on the tonsillar fossa |
| Baum tonsil needle holder | Curved needle holder for suture ligation of bleeding vessels deep in the tonsillar fossa |
| DeBakey forceps | Tissue handling/fine dissection |
| Negus artery forceps / straight artery forceps | Clamping bleeding vessels |
| Bipolar diathermy forceps | Coagulation of bleeding points |
| Tonsil sponge/swab | Tamponade of the tonsillar fossa after removal |
| Backhaus towel clamps | Securing drapes |
| Suction tip (Yankauer) | Clearing blood and secretions from the field |
Step-by-Step Operative Technique (Cold Steel Dissection)
Step 1 - Position and Exposure
- The patient is placed supine with a shoulder roll under the shoulders.
- The surgeon sits at the patient's head.
- A Crowe-Davis or McIvor mouth gag is gently inserted, fitting the endotracheal tube into the groove of the blade. The gag is opened to expose the oropharynx and suspended from a rack or held by an assistant.
- A Wieder tongue depressor depresses the tongue base further if needed.
- Bilateral tonsils are inspected and the procedure is usually started on the right side.
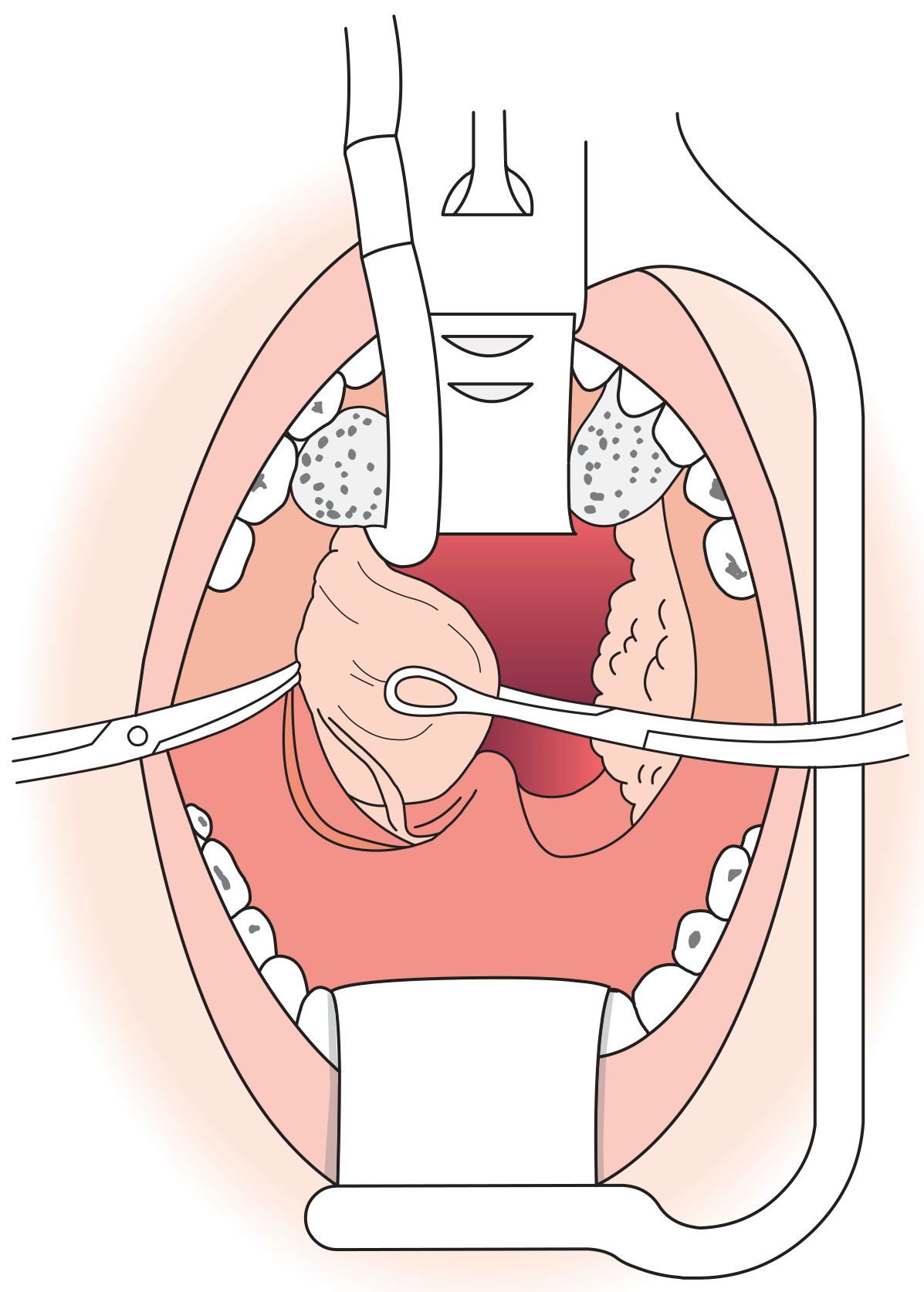
Step 2 - Grasping and Medialization of the Tonsil
- The Allis clamp (or White tonsil clamp) is applied to the superior pole of the tonsil.
- The tonsil is pulled medially (toward the midline), which stretches and tautens the overlying mucosa, making the anterior pillar and tonsillar capsule border visible.
Step 3 - Mucosal Incision
- Using a No. 7 knife handle fitted with a No. 12 blade, an incision is made through the mucosa of the anterior faucial pillar at the medial edge of the tonsil, running from the superior pole downward.
- The incision stays just outside the tonsillar capsule to avoid entering tonsillar tissue and causing bleeding.
Step 4 - Identifying the Capsule Plane
- The Hurd dissector is used to retract the anterior pillar laterally and begin blunt dissection.
- The Fisher tonsil knife/dissector or curved Metzenbaum scissors is then used to identify the avascular plane of loose areolar tissue between the tonsillar capsule and the underlying superior constrictor and palatoglossus muscles.
- Dissection proceeds in this plane - staying outside the capsule avoids inadvertent entry into tonsillar tissue and minimizes bleeding.
Step 5 - Dissection from Superior to Inferior Pole
- Using the Fisher tonsil dissector (and supplemented by gauze-on-forceps blunt dissection), the tonsil is progressively freed from its bed:
- Start at the superior pole
- Work around the lateral surface
- Continue to the inferior pole (where the attachment to the lingual tonsil remains)
- The Hurd dissector retracts the posterior pillar and helps expose deeper tissue planes.
- A small inferior pedicle remains at the end of this dissection.
Step 6 - Removal of the Tonsil (Snaring)
- The Tyding tonsil wire snare is passed around the inferior pedicle of the tonsil.
- The wire is tightened and the tonsil is amputated at the inferior pole, severing its attachment to the lingual tonsil.
- The snare wire must pass freely through the shaft - any resistance can cause tearing and bleeding.
- The tonsil is removed and sent for histopathology if indicated.
Step 7 - Haemostasis
- A tonsil sponge (held in Foerster-Ballenger sponge forceps) is packed into the tonsillar fossa and firm pressure is applied for 2-3 minutes.
- The sponge is removed and the fossa inspected for bleeding.
- Bleeding vessels are controlled by:
- Ligature (suture ties) using the Baum tonsil needle holder and absorbable suture (e.g., Vicryl or silk)
- Negus artery forceps to clamp vessels before tying
- Bipolar diathermy forceps for coagulation of small bleeding points
- The same procedure is then performed on the contralateral (left) tonsil.
Step 8 - Final Check and Closure
- Both tonsillar fossae are inspected thoroughly for residual bleeding.
- The mouth gag is carefully released and removed.
- The pharynx is suctioned with a Yankauer sucker.
- The patient is turned to the lateral (recovery) position before extubation to prevent aspiration of blood.
Hot/Diathermy Technique (Most Common in the US)
Instead of cold steel, a monopolar electrocautery (set at ~20 Watts with a traditional tip) is used:
- The Allis clamp grasps and medializes the superior pole.
- The lateral tonsil edge is identified submucosal.
- The cautery incises the superior pole, and the avascular plane is developed using the cautery tip.
- The entire tonsil is removed from superior to inferior pole.
- Haemostasis is maintained continuously with the cautery throughout the dissection.
Note: The NPTA audit data showed that cold steel + ties has lower secondary haemorrhage rates (1.0%) compared to monopolar (5.5%) or bipolar diathermy forceps (4.3%) alone, as noted in Scott-Brown's Otorhinolaryngology, Vol 2.
Coblation Technique
- Uses an Arthrocare Evac plasma wand (Coblation device) with saline irrigation.
- Creates a plasma field of ionized particles that dissociates tissue at low temperature (40-70°C), minimizing heat damage to surrounding tissue.
- Two variants: extracapsular (total removal) or intracapsular (partial - leaves a thin capsule layer).
- Particularly popular for paediatric cases given lower post-operative pain.
Post-operative Care
- Patient placed in the lateral/tonsil position on recovery to allow blood/secretions to drain from the mouth.
- Closely observed for reactionary (primary) haemorrhage in the first few hours.
- Oral fluids encouraged early; a normal diet is resumed as soon as tolerated.
- Secondary haemorrhage (5-10 days post-op, due to sloughing of membrane) is the main late complication.
Summary Table of Key Instruments and Their Role
| Step | Instrument | Role |
|---|---|---|
| Exposure | McIvor/Crowe-Davis gag | Opens mouth, holds ETT |
| Retraction | Wieder tongue depressor | Depresses tongue |
| Grasping | Allis clamp | Medializes tonsil |
| Incision | No. 12 blade + No. 7 handle | Cuts anterior pillar mucosa |
| Dissection | Fisher tonsil knife/dissector | Frees tonsil from capsule plane |
| Dissection | Hurd dissector | Blunt dissection + pillar retraction |
| Dissection | Metzenbaum scissors | Identifies avascular plane |
| Removal | Tyding snare | Amputates inferior pedicle |
| Haemostasis | Foerster-Ballenger forceps | Holds tonsil sponge for pressure |
| Haemostasis | Negus artery forceps | Clamps bleeding vessels |
| Haemostasis | Baum needle holder | Suture ligation |
| Haemostasis | Bipolar diathermy | Coagulates small bleeders |
| Suction | Yankauer sucker | Clears blood/secretions |
Sources: Bailey & Love's Short Practice of Surgery 28th Ed., Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2, Cummings Otolaryngology Head and Neck Surgery, and StatPearls Tonsillectomy (NCBI).
This is a shared conversation. Sign in to Orris to start your own chat.