Anatomy
Asking for Preferences
Breast
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full anatomy of the breast.
Anatomy of the Breast
Position and Surface Anatomy
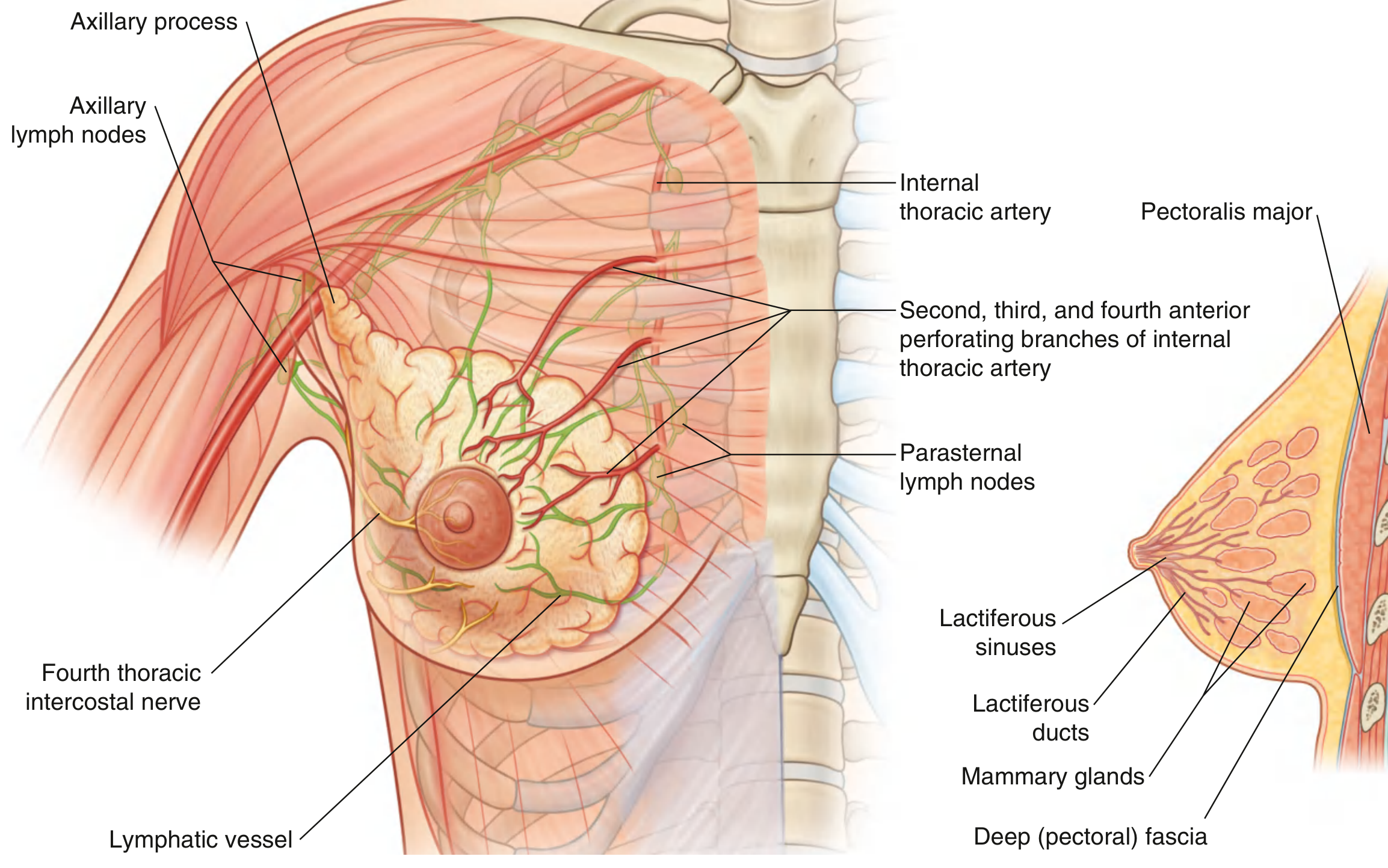
The breast lies on the anterior thoracic wall, between ribs II and VI, overlying the pectoralis major muscle (and partly serratus anterior and external oblique). Each breast extends superlaterally around the lower margin of pectoralis major into the axilla as the axillary tail (axillary process of Spence) - a clinically important extension since pathology here can mimic axillary lymphadenopathy.
- Gray's Anatomy for Students, p. 168
Structural Layers (Superficial to Deep)
| Layer | Details |
|---|---|
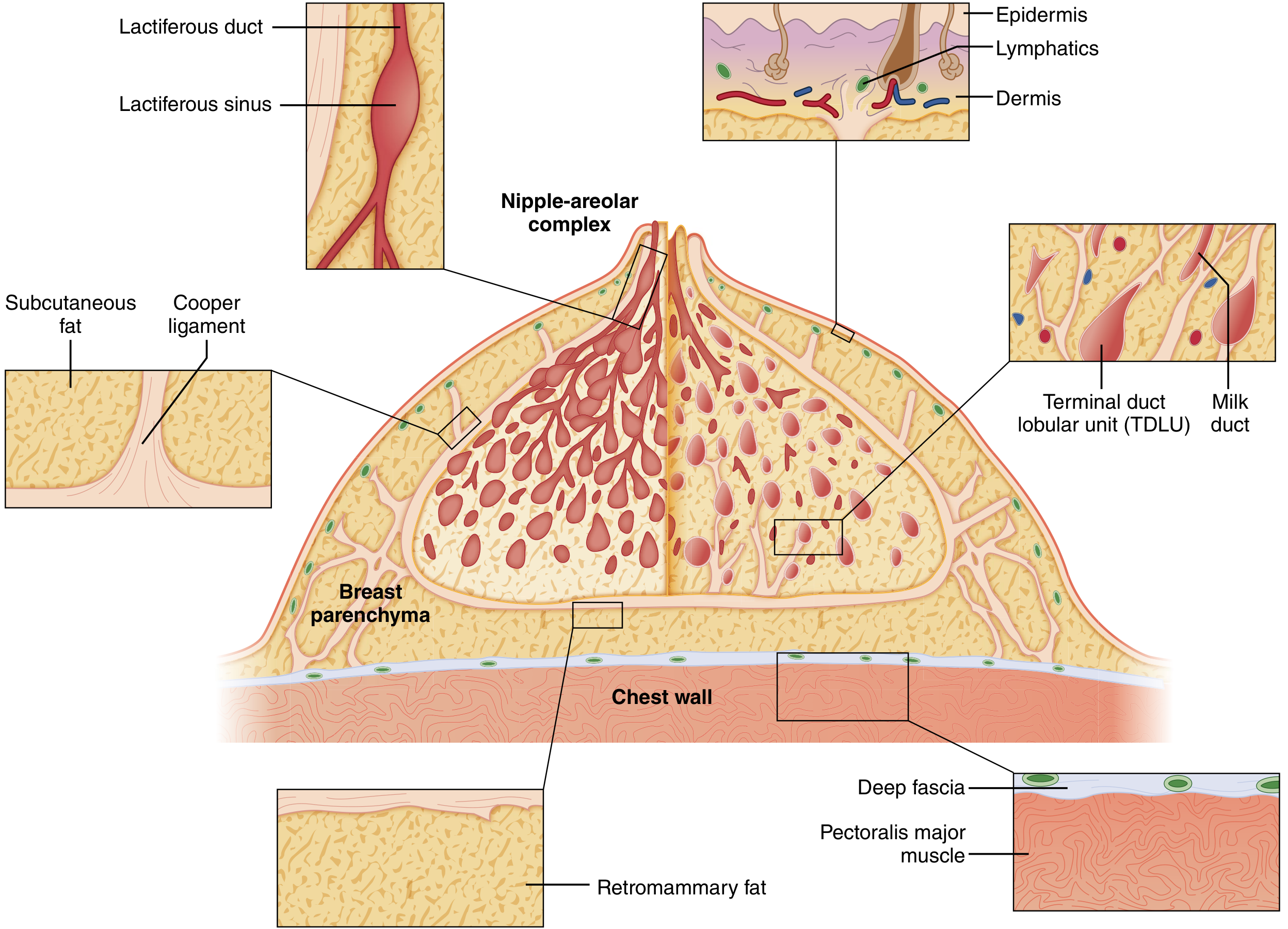
| Skin | Contains nipple-areolar complex (NAC) |
| Subcutaneous fat | Contains superficial fascial layers |
| Breast parenchyma | Glandular + fibrous + adipose tissue |
| Retromammary space | Loose areolar tissue - allows breast mobility |
| Deep (pectoral) fascia | Over pectoralis major |
The breast lies between the superficial fascia and the superficial layer of the deep (pectoral) fascia. The retromammary space - a potential space between the breast and the pectoral fascia - allows surgical separation.
Internal Structure
The mature breast has three principal tissue types:
- Glandular epithelium - the functional secretory component
- Fibrous stroma - provides structural support
- Adipose tissue - predominates after menopause as glandular tissue involutes
Duct System
- 15-20 lobes, each draining via a lactiferous duct that opens at the nipple
- Each duct has a dilated segment just below the NAC - the lactiferous sinus
- Ducts branch progressively outward in a radial pattern, terminating in terminal duct lobular units (TDLUs)
- TDLUs = the acini + terminal ductules - the milk-forming units of the lactating breast, and the site where most breast cancers originate
The entire ductal system is lined by epithelial cells surrounded by myoepithelial cells (contractile, propel milk toward the nipple). Outside both layers lies a continuous basement membrane - its integrity is the boundary between in-situ (DCIS) and invasive cancer.
- Sabiston Textbook of Surgery, p. 1369-1370
- THIEME Atlas of Anatomy, p. 229
Cooper's (Suspensory) Ligaments
Fibrous bands running from the chest wall deep fascia to the skin dermis, providing shape and support. When infiltrated by cancer, they tether and shorten, causing skin dimpling - the classic "peau d'orange" sign.
Blood Supply
| Source | Branches | Region Supplied |
|---|---|---|
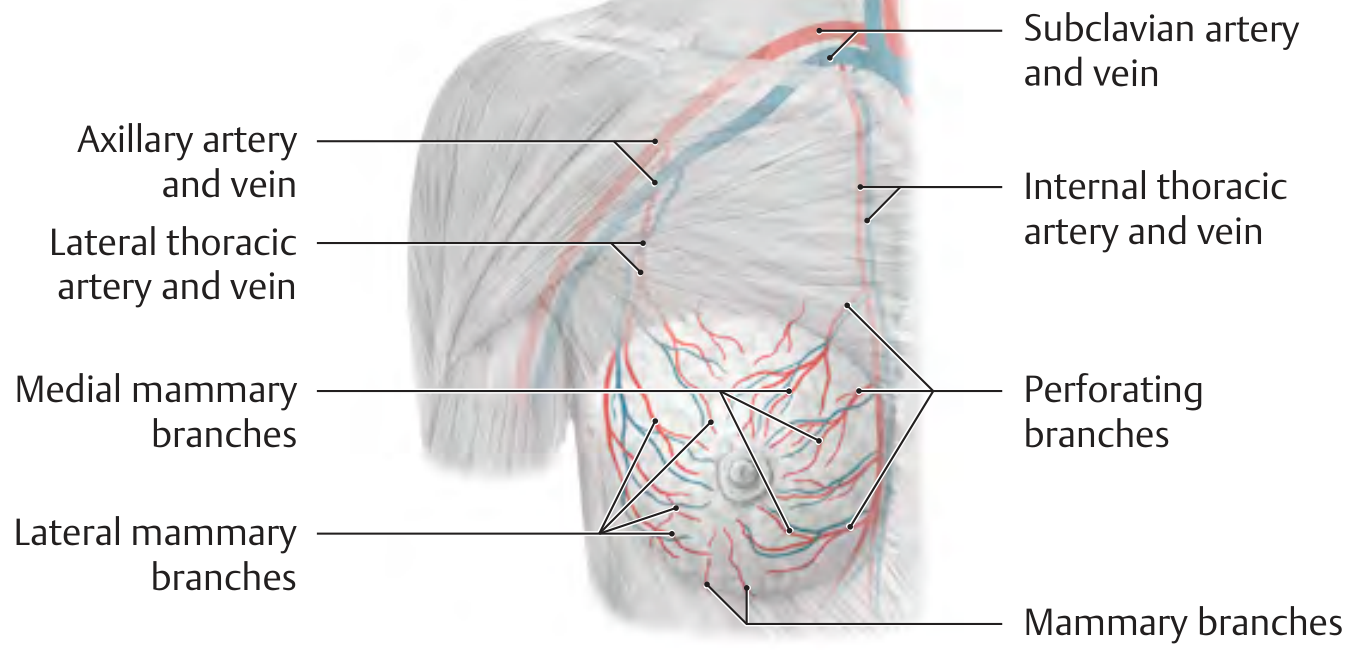
| Internal thoracic artery | Perforating branches (2nd-4th intercostal spaces) | Anteromedial breast |
| Lateral thoracic artery (from axillary) | Lateral mammary branches | Lateral breast |
| Intercostal arteries (2nd-5th) | Direct mammary branches | Peripheral breast |
Venous drainage mirrors arterial supply - internal and lateral thoracic veins.
- THIEME Atlas of Anatomy, p. 229
Nerve Supply
Sensory innervation is segmental from the 2nd-6th intercostal nerves (lateral and medial mammary branches). The upper breast also receives branches from the supraclavicular nerves (cervical plexus, C3-C4).
- The 4th intercostal nerve carries sensation to the nipple-areolar complex - relevant in surgical planning.
Lymphatic Drainage
This is the most clinically important aspect for breast cancer staging and surgery.
| Drainage Route | % of Lymph | Destination |
|---|---|---|
| Axillary nodes | 70-80% | Primary route |
| Internal mammary nodes | ~20% (combined); 2-3% primary | Along internal thoracic vessels |
| Supraclavicular nodes | After axillary level III | "Outside" the axilla proper |
Lymph flows from parenchyma → subareolar plexus (Sappey's plexus, under the nipple) → interlobular lymphatics → axillary or internal mammary nodes.
Axillary Lymph Node Levels (defined by relation to pectoralis minor)
| Level | Location | Notes |
|---|---|---|
| Level I | Lateral to lateral border of pectoralis minor | Lowest (most accessible) |
| Level II | Posterior to pectoralis minor + Rotter's/interpectoral nodes | Between pec minor/major |
| Level III | Medial to pectoralis minor (infraclavicular) | Highest; at Halsted's ligament |
The apex of the axilla is the costoclavicular (Halsted's) ligament, where the axillary vein becomes the subclavian vein. Drainage continues to supraclavicular nodes (N3 disease in staging).
- Sabiston Textbook of Surgery, p. 1370
Key Surgical Nerves in the Axilla
These must be identified and preserved during axillary lymph node dissection (ALND):
| Nerve | Origin | Muscle Innervated | Injury Consequence |
|---|---|---|---|
| Long thoracic nerve | Cervical plexus (C5-C7) | Serratus anterior | Winged scapula |
| Thoracodorsal nerve | Posterior cord, brachial plexus | Latissimus dorsi | Weak arm adduction/extension |
| Medial pectoral nerve | Medial cord, brachial plexus | Pectoralis major | Atrophy of pec major |
| Intercostobrachial nerves (sensory) | Intercostal nerves (T2) | Skin of medial upper arm | Cutaneous numbness/pain |
Development & Physiological Changes
- The breast is a modified sweat (sudoriferous) gland, derived from ectoderm along the "milk line" (axilla to groin)
- At puberty, estrogen drives ductal elongation and branching; progesterone and prolactin develop lobules
- In adolescence: predominantly epithelium + stroma
- In postmenopausal women: glandular tissue involutes and is replaced by adipose tissue (explains why mammography sensitivity improves with age)
Summary of Key Clinical Correlations
- Peau d'orange = invasion of Cooper's ligaments by cancer → skin tethering
- Nipple retraction = fibrosis/cancer tethering a major duct
- Sentinel lymph node biopsy exploits the concept that Sappey's plexus drains predictably to the first (sentinel) axillary node
- Winged scapula post-mastectomy = injury to the long thoracic nerve
- DCIS vs invasive cancer = determined by whether the basement membrane of the TDLU has been breached
Sources: Gray's Anatomy for Students | Sabiston Textbook of Surgery | THIEME Atlas of Anatomy (General Anatomy and Musculoskeletal System)
This is a shared conversation. Sign in to Orris to start your own chat.