Introduction of Dialysis.
introduction to dialysis principles types hemodialysis peritoneal dialysis
"dialysis" AND "hemodialysis"
Introduction to Dialysis
1. Definition and Overview
"Dialysis may be required for the treatment of either acute or chronic kidney disease."
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
2. When Is Dialysis Needed?
Indications for Starting Dialysis
| Indication | Detail |
|---|---|
| Uremic encephalopathy or neuropathy | CNS/PNS manifestations of uremia |
| Pericarditis or pleuritis | Uremic serositis |
| Uremic bleeding | Platelet dysfunction |
| Fluid overload refractory to diuretics | Volume overload |
| Uncontrolled hypertension | Refractory to medications |
| Persistent hyperkalemia | Life-threatening arrhythmia risk |
| Metabolic acidosis | Refractory to bicarbonate therapy |
| Malnutrition / weight loss | Uremic anorexia |
| Persistent nausea and vomiting | Uremic gastropathy |
3. Epidemiology
- In the United States, over 800,000 patients have treated ESKD (end-stage kidney disease), the vast majority requiring dialysis.
- Since 2000, prevalence of treated ESKD in the US has risen 65%, mostly reflecting improved dialysis survival.
- The crude incidence is approximately 363 cases per million population per year in the US.
- Leading cause of ESKD: diabetes mellitus (~45%), followed by hypertension (~30%), glomerulonephritis, polycystic kidney disease.
- Globally, prevalence is highest in Taiwan (3170 pmp), Japan (2620 pmp), and the United States (2080 pmp).
- Deaths on dialysis are mainly from cardiovascular disease and infections.
4. Physiological Principles of Dialysis
A. Diffusion
- Urea, creatinine, uric acid (uremic toxins)
- Excess potassium, phosphate
- Corrects metabolic acidosis (via bicarbonate in dialysate)
B. Convection (Ultrafiltration)
- In hemodialysis: driven by hydrostatic pressure applied across the artificial membrane
- In peritoneal dialysis: driven by an oncotic gradient using high-dextrose or large carbohydrate polymers in dialysate
Dialysate Composition
- Potassium: ~2 mEq/L (lower than plasma) to remove excess K⁺
- Bicarbonate: ~35 mEq/L (higher than plasma) to correct acidosis
- Prepared by reverse osmosis + deionization to remove trace minerals, bacteria, and endotoxins
5. Types of Dialysis
A. Hemodialysis (HD)
| Type | Setting | Frequency | Duration |
|---|---|---|---|
| Conventional in-center HD | Dialysis unit / hospital | 3×/week | 3-4 hours/session |
| Home HD | Patient's home | 3-6×/week | Variable |
| Nocturnal HD | Home / center | 6×/week (overnight) | 6-8 hours |
| CRRT (Continuous RRT) | ICU only | Continuous | 24 hrs/day |
| PIRRT / SLED (Slow Low-Efficiency Dialysis) | ICU | Daily or alternating | 6-12 hrs/session |
- Arteriovenous Fistula (AVF) - preferred; native vein anastomosed to artery (e.g., radiocephalic, brachiocephalic)
- Arteriovenous Graft (AVG) - synthetic conduit connecting artery to vein
- Central Venous Catheter (CVC) - temporary or tunneled; highest infection risk
- Measured by Urea Reduction Ratio (URR): target ≥65% per session
- Or by spKt/V (single-pool normalized urea clearance): target ≥1.2 on thrice-weekly schedule
- Increasing frequency (6×/week) improves blood pressure, left ventricular hypertrophy regression, and phosphorus control
B. Peritoneal Dialysis (PD)
| Type | Description |
|---|---|
| CAPD (Continuous Ambulatory PD) | Manual exchanges ~4×/day; no machine needed |
| CCPD (Continuous Cyclic PD) | Automated cycler performs exchanges at night |
- Ongoing, gentle, continuous clearance (vs. intermittent HD)
- Small molecules (urea, creatinine) are cleared less efficiently than HD per unit time
- Better preservation of residual kidney function early on
- Preferred for: hemodynamic instability, remote locations, patient preference for independence
C. Continuous Renal Replacement Therapy (CRRT)
6. Treatment Modality Selection
| Factor | Favors HD | Favors PD |
|---|---|---|
| Hemodynamic stability | Unstable → CRRT/SLED | Stable → PD acceptable |
| Vascular access | AVF available | No suitable vascular access |
| Abdominal surgery history | Preferred | Adhesions may prevent PD |
| Patient preference | In-center care | Home independence |
| Residual kidney function | Either | PD preserves better |
| Body size (large) | HD may be more adequate | Less efficient in large patients |
| Visual/dexterity impairment | Center HD | Difficult to self-manage PD |
7. Complications of Dialysis
Hemodialysis Complications
- Hypotension (most common intradialytic complication) - due to rapid fluid removal
- Access problems: thrombosis, stenosis, infection, inadequate flow
- Cardiovascular: LV hypertrophy, arrhythmias, pericarditis
- Infections: bacteremia (especially with CVC access)
- Dialysis disequilibrium syndrome: rapid osmotic shifts causing cerebral edema (especially first sessions)
- Anemia, renal osteodystrophy, amyloidosis (β2-microglobulin accumulation - long-term)
- Chronic inflammation: exposure to impurities in dialysate
Peritoneal Dialysis Complications
- Peritonitis: most common complication - usually gram-positive organisms from skin flora
- Catheter-related infections (exit site, tunnel infections)
- Inadequate ultrafiltration: membrane failure over time
- Hernias, hydrothorax: pressure-related
- Metabolic: hyperglycemia (from dextrose), hypertriglyceridemia, protein loss
8. Outcomes and Prognosis
- Dialysis does not cure CKD; it maintains life until transplantation or death
- Kidney transplantation is superior to dialysis in all eligible patients - better survival, quality of life, and cost-effectiveness
- The 5-year survival of patients on dialysis in developed countries is approximately 35-40%
- Cardiovascular disease remains the leading cause of death in dialysis patients
- More frequent dialysis (nocturnal HD 6×/week) has shown 46% mortality reduction at median 3.6-year follow-up compared to conventional thrice-weekly HD
9. Recent Evidence (2024-2025)
Summary
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 323
- Goldman-Cecil Medicine, International Edition, Chapter 117 (Table 117-1)
- Brenner and Rector's The Kidney - Chapters 81, 96
- Comprehensive Clinical Nephrology, 7th Edition
- Flythe JE & Watnick S. Dialysis for Chronic Kidney Failure: A Review. JAMA. 2024 Nov 12. PMID: 39356511
Create infographic image
Medical infographic titled "Introduction to Dialysis" with a clean, professional clinical design. Include the following sections clearly organized: 1. HEADER: "INTRODUCTION TO DIALYSIS" with a kidney icon and subtitle "Renal Replacement Therapy" 2. WHAT IS DIALYSIS? - Brief definition box: "Artificial filtration of blood when kidneys fail — removes waste, excess solutes & fluid" 3. WHEN IS IT NEEDED? - Box showing indications: eGFR < 10 mL/min, Uremic symptoms, Hyperkalemia, Fluid overload, Metabolic acidosis, Uremic encephalopathy, Pericarditis 4. HOW IT WORKS - Two mechanisms side by side: - DIFFUSION: solutes move along concentration gradient (urea, K+, phosphate removed) - CONVECTION (ULTRAFILTRATION): fluid removed by pressure gradient 5. TWO MAIN TYPES - Split panel: LEFT: HEMODIALYSIS (HD) - icon of dialysis machine - "Blood filtered outside body through artificial membrane" - 3x/week, 3-4 hrs - Access: AVF (preferred), AVG, CVC RIGHT: PERITONEAL DIALYSIS (PD) - icon of abdomen/catheter - "Uses peritoneal membrane inside abdomen" - CAPD (manual 4x/day) or CCPD (automated nightly) 6. SPECIAL TYPES - small boxes: CRRT (ICU, continuous), SLED/PIRRT (ICU, 6-12 hrs) 7. COMPLICATIONS - two columns: HD: Hypotension, Access thrombosis, Infection, Arrhythmia | PD: Peritonitis, Catheter infection, Ultrafiltration failure 8. KEY FACT BANNER at bottom: "800,000+ ESKD patients in the US | Leading causes: Diabetes (45%), Hypertension (30%) | Transplantation remains gold standard" Use a blue and teal color scheme, modern medical icons, clean sans-serif fonts, and a white background. Make it visually rich, organized with clear section borders and labels.
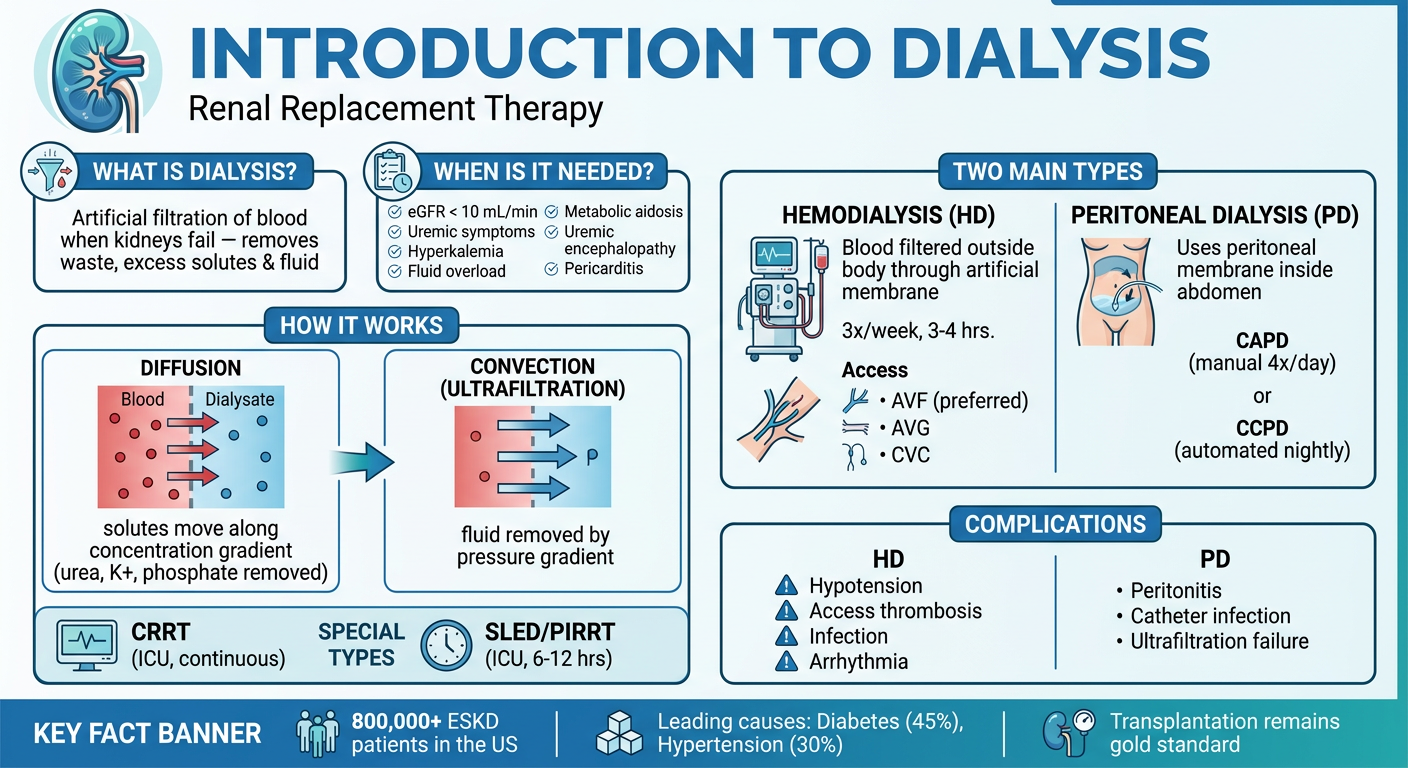
- Definition - what dialysis is and why it's needed
- Indications - when to start (eGFR, uremic symptoms, etc.)
- Mechanisms - diffusion vs. convection/ultrafiltration
- Two main types - Hemodialysis (HD) vs. Peritoneal Dialysis (PD) with key differences
- Special ICU modalities - CRRT and SLED/PIRRT
- Complications - for both HD and PD
- Key epidemiology - US prevalence, leading causes of ESKD