sarcidosis
Reading File
Finding Sources
Searching PubMed
sarcoidosis
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have all the material needed to write a thorough, well-organized answer. Here it is:
Sarcoidosis
Definition and Epidemiology
Sarcoidosis is a chronic multisystem granulomatous disease of unknown etiology, characterized by the formation of non-caseating (non-necrotizing) granulomas in affected tissues. It occurs worldwide, in patients of every age, ethnicity, and socioeconomic class, though patterns of prevalence vary considerably.
- Prevalence: Highest in Scandinavia (Sweden: 64/100,000). In the United States: 10.9/100,000 in White persons vs. 35.5/100,000 in African Americans.
- Sex: Women are slightly more affected, particularly African American women aged 30-39. Late-onset disease (ages 65-69) is 5x more common in women.
- Lifetime risk: 0.85% (White U.S. residents) vs. 2.4% (Black U.S. residents).
- Onset: Most commonly between ages 20-40, with a second peak at ages 65-69.
- Andrews' Diseases of the Skin, p. 1321
Pathophysiology
The disease is driven by a Th1/Th17 immune response in which activated macrophages and CD4+ helper T cells form granulomas. IL-2 and IFN-γ secreting CD4+ Th cells play a key role, along with TNF and other Th1/Th17 cytokines.
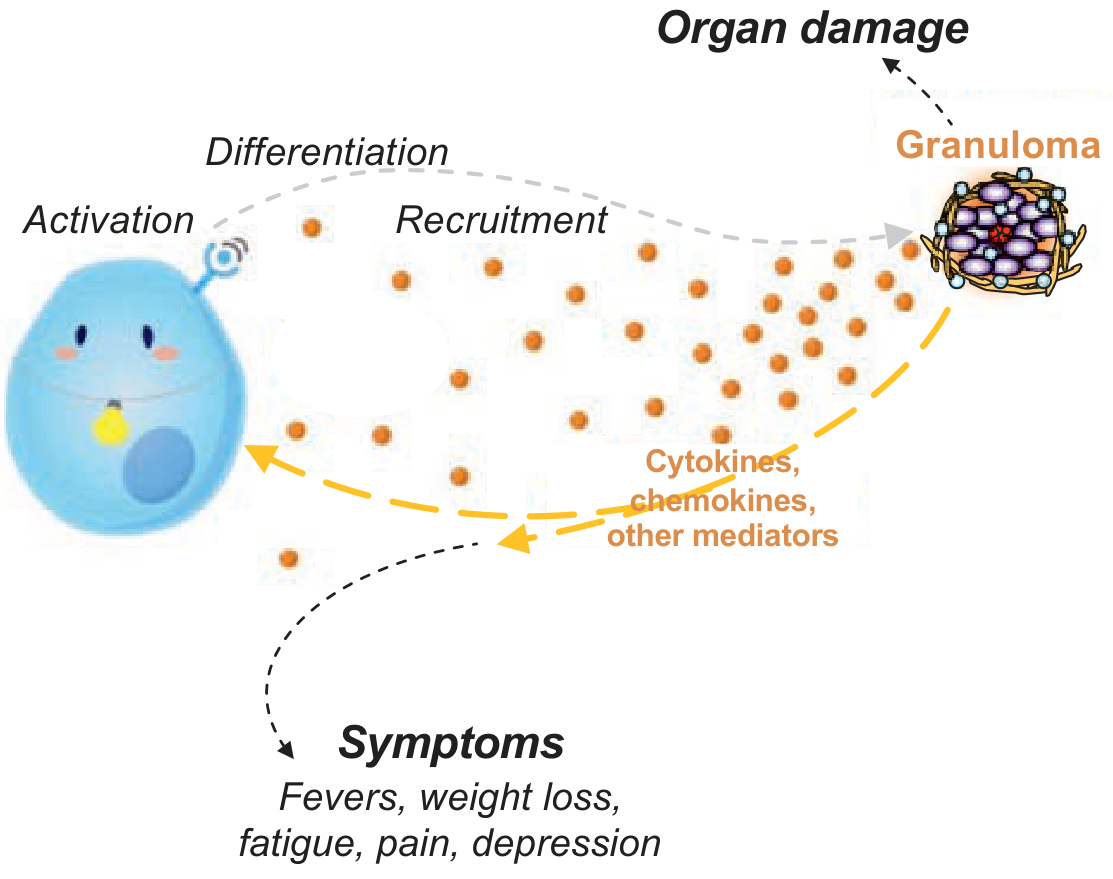
Circulating cytokines, chemokines, and other mediators not only cause direct granulomatous organ damage but also produce systemic symptoms (fatigue, fever, weight loss, depression) through non-tissue-damaging mechanisms - called parasarcoidosis syndromes.
Key genetic associations:
- HLA-DRB1 variants increase risk
- HLA-DQB1*0201 and HLA-DRB1*0301 associate with acute disease and good prognosis
- HLA-B8/DR3 associated with Löfgren syndrome
- TNF promoter polymorphisms linked to erythema nodosum
- ANXA11, BTNL2, CCR5 polymorphisms also identified
A notable metabolic effect: active sarcoidosis upregulates 1-alpha-hydroxylase, converting inactive 25-OH vitamin D to active 1,25-OH vitamin D, causing hypercalcemia.
- Fishman's Pulmonary Diseases and Disorders, pp. 470-475
Organ Involvement
Sarcoidosis earns its reputation as a "great imitator" - it can affect virtually any organ.
| Organ System | Prevalence | Key Manifestations |
|---|---|---|
| Pulmonary | >90% | Restrictive/obstructive disease, reduced DLCO, bilateral hilar adenopathy, pulmonary fibrosis, pulmonary hypertension |
| Constitutional | >50% | Fever, night sweats, fatigue, weight loss |
| Skin | 20-30% | Lupus pernio, papules/plaques/nodules, erythema nodosum, scar/tattoo granulomas |
| Eyes | 20-30% | Anterior/posterior uveitis, optic neuritis, chorioretinitis |
| Hematologic | 20-30% | Lymphadenopathy, splenomegaly, anemia, lymphopenia |
| Cardiac | 5-20% | Arrhythmias, heart block, dilated cardiomyopathy, sudden death |
| Liver/abdominal | 10-20% | Hepatomegaly, granulomatous hepatitis, portal hypertension |
| Joints/MSK | 10-20% | Arthralgia, polyarthritis, Achilles tendinitis, dactylitis |
| Neurologic | 5-10% | Bell's palsy (most common), basilar meningitis, optic neuropathy, small fiber neuropathy |
| Renal | <10% | Nephrocalcinosis, renal calculi, interstitial nephritis |
- Fishman's Pulmonary Diseases and Disorders, Table 53-2
Key Specific Syndromes
Löfgren Syndrome: Acute triad of erythema nodosum + bilateral hilar adenopathy + periarthritis/arthritis, typically with fever. Generally carries a good prognosis.
Lupus Pernio: Indurated plaques/nodules on the nose and central face - a marker of chronic sarcoidosis strongly associated with upper airway granulomatous infiltration, pulmonary fibrosis, and persistent pulmonary involvement.
Cardiac Sarcoidosis: Clinically apparent in <10% of U.S. cases, but autopsy studies show myocardial involvement in >20% (U.S.) and >50% (Japan). Ventricular arrhythmias and high-degree heart block can cause sudden death.
Neurosarcoidosis: Cranial neuropathies dominate; VII nerve (Bell's) palsy is most common. Hypothalamic involvement can cause diabetes insipidus, hypogonadism, or hyperprolactinemia.
Chest Radiographic Staging (Scadding)
| Stage | Finding | Prognosis |
|---|---|---|
| 0 | Normal | - |
| I | Bilateral hilar adenopathy only | >80% resolve at 2-5 years |
| II | Hilar adenopathy + parenchymal infiltrates | Intermediate |
| III | Parenchymal infiltrates only (no adenopathy) | <30% resolve |
| IV | Pulmonary fibrosis | Does not resolve |
Diagnosis
The diagnosis is never fully secure and requires:
- Compatible clinical and radiologic presentation
- Histologic demonstration of non-necrotizing granulomas (ideally in two or more organs)
- Exclusion of other causes (especially tuberculosis, fungal infections, other granulomatous diseases)
Useful workup:
- Chest radiograph and HRCT
- Pulmonary function tests (FVC, DLCO - DLCO is the most sensitive early marker)
- Serum ACE (angiotensin-converting enzyme) - elevated in ~60%, neither sensitive nor specific
- 24-hour urinary calcium (hypercalciuria)
- LFTs, renal function, serum calcium
- Ophthalmologic examination (slit-lamp)
- ECG (screening for cardiac involvement)
- Serum LDH, lysozyme
- BAL: CD4:CD8 ratio >3.5 is suggestive
- FDG-PET/CT: useful for detecting active inflammation in cardiac and neurologic sarcoidosis and identifying the best biopsy site
- Cardiac MRI with gadolinium: reveals myocardial inflammation and scarring in a non-coronary distribution
Biopsy sites (least invasive first): skin lesions, peripheral lymph nodes, transbronchial lung biopsy (high yield ~70-90%), EBUS-guided mediastinal biopsy.
The historical Kveim test (intradermal inoculation of sarcoid splenic tissue) is now essentially obsolete.
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 3565-3575
Treatment
There are no FDA-approved systemic therapies for sarcoidosis. Treatment is indicated for threatened organ function, not just for the presence of disease.
Indications for Treatment
- Severe ocular, cardiac, or neurologic disease
- Progressive, persistent, or symptomatic pulmonary disease
- Disfiguring cutaneous disease (especially lupus pernio)
- Persistent hypercalcemia
- Renal or hepatic dysfunction
- Symptomatic myopathy, painful lymphadenopathy
- Severe fatigue and weight loss
Treatment Ladder
1. Corticosteroids (first-line)
- Prednisone 20-40 mg/day, tapered slowly to maintenance 5-15 mg/day
- Duration: minimum 6-24 months (premature taper leads to relapse)
- Inhaled corticosteroids have limited effectiveness alone
- Löfgren syndrome: NSAIDs first; corticosteroids if arthritis is disabling
2. Steroid-sparing agents (second-line)
- Hydroxychloroquine (200-400 mg/day): particularly for skin and hypercalcemia
- Methotrexate (7.5-15 mg/week): most widely used second-line agent
- Azathioprine: alternative immunosuppressant
3. Biologics (refractory disease)
- Infliximab (anti-TNF): evidence-based for pulmonary and cutaneous sarcoidosis; a recent 2025 systematic review and meta-analysis (PMID: 40393718) confirmed efficacy of biologic and targeted synthetic therapies in sarcoidosis
- Adalimumab: alternative anti-TNF
- Caution: anti-TNF agents are contraindicated in active infections (especially TB - screening required)
Cutaneous disease specifically:
-
Intralesional corticosteroid injections (first-line for localized lesions, repeated every 2-4 weeks)
-
Topical steroids often inadequate (poor penetration of thick granulomas)
-
Hydroxychloroquine or methotrexate for refractory/widespread disease
-
Fishman's Pulmonary Diseases and Disorders, pp. 597-619
-
Textbook of Family Medicine 9e, p. 489
Prognosis
- Stage I disease: excellent prognosis; most resolve spontaneously
- Stage II/III: ~50-70% improve with treatment
- Stage IV (fibrotic): irreversible
- Chronic progressive disease occurs in >20% overall
- Monitoring for at least 3 years after apparent remission is recommended; longer for serious pulmonary or extrapulmonary disease
- Special concern: aspergilloma can develop in cavitary/fibrotic upper lobe lesions and is a serious complication
Recent evidence: A 2025 systematic review and meta-analysis in Thorax (PMID: 40393718) confirmed the efficacy of biologics (particularly anti-TNF agents) in sarcoidosis - relevant for refractory cases where standard immunosuppression has failed.
Search for recent clinical guidelines on cardiac sarcoidosis screeningnd year CNS chapter full questions and answers for mpmsu exam
Asking for Preferences
pharmacology 2nd year mbbs CNS chapter answers and questions for mpmsu exams
Reading File
Searching the Web
MPMSU 2nd year MBBS pharmacology CNS chapter previous year questions
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Here is a complete MPMSU-pattern CNS Pharmacology Q&A, organized exactly as the exam expects.
What's Covered (All Major MPMSU CNS Topics):
Long Answer Questions (10 marks each):
- Antiepileptic drugs - classification + Phenytoin (mechanism, uses, adverse effects)
- Antipsychotics - classification + Chlorpromazine in full detail
- Opioid analgesics - classification + Morphine + Morphine vs Pethidine comparison table
Short Answer Questions (5 marks each):
- Benzodiazepines/Diazepam - GABA-A mechanism, frequency of Cl⁻ opening, uses
- Levodopa + Carbidopa - why L-DOPA is used, on-off phenomenon, adverse effects
- Sedative-hypnotics - classification + Barbiturate mechanism (duration of Cl⁻ channel opening)
- Status Epilepticus - stepwise treatment ladder (lorazepam → fosphenytoin → thiopental)
- Antidepressants - all classes (SSRI, TCA, MAOI, SNRI) with mechanisms
Short Notes / Viva (2-3 marks):
- General anesthesia stages (Guedel's stages I-IV)
- Nitrous oxide
- Drug of Choice table (must-memorize for MPMSU)
- Methanol poisoning treatment
Key Mnemonics: NMS vs Serotonin Syndrome, Opioid tolerance "CAD", CPZ side effects "ABCDE"
This is a shared conversation. Sign in to Orris to start your own chat.