i send you requirement listr of teacher , this is my ppt topic "Clinical and laboratory diagnosis of fungal diseases affecting the skin and its appendages" i want make ppt on this include image related to data at every slide , and kindly make ppt sccording to requirement list
tinea capitis dermatophyte ringworm scalp clinical
candidiasis skin nails oral thrush clinical photo
KOH mount microscopy fungal hyphae skin scraping laboratory diagnosis
Sabouraud dextrose agar fungal culture dermatophyte colony
onychomycosis nail fungal infection tinea unguium
Wood lamp ultraviolet fluorescence tinea capitis green
mkdir -p /home/daytona/workspace/fungal-ppt && ls /home/daytona/workspace/fungal-ppt/
- Topic: Clinical and laboratory diagnosis of fungal diseases affecting the skin and its appendages
- Student info: Course: Medical Immunology
- Keep exactly what you gave: Medical Immunology
- Use requirement-compliant course title: Microbiology, Virology and Immunology
1
~/fungal-ppt/build.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Colour palette ──────────────────────────────────────────────────────────
const DARK_BG = "0D1B2A"; // deep navy (dominant ~65 %)
const MID_BG = "1B2A3A"; // slate navy (card / panel fills)
const ACCENT = "2EC4B6"; // teal (titles, rules, icons)
const LIGHT_TXT = "E8F4F8"; // near-white
const MUTED_TXT = "A8C8D4"; // cool grey-blue
const GOLD = "F4A261"; // warm gold (callout highlight, ≤1 per slide)
// ── Typography ──────────────────────────────────────────────────────────────
const FONT = "Arial";
const T_TITLE = 28;
const T_HEAD = 24;
const T_BODY = 18;
const T_SMALL = 16;
const T_TAG = 13;
// ── Image URLs ───────────────────────────────────────────────────────────────
const IMG_URLS = {
tinea_composite : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_154b24b17aad789e04602e59d7dc231e6d6b2846636a638daf089b39e9e28c1f.jpg",
tinea_capitis : "https://cdn.orris.care/cdss_images/DermNetNZ_1760031386862_489e0d14-6366-4e73-82ef-d806cf9124dd.jpg",
koh_hyphae : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_b287ff1a1f0fddab8b51710d103849b604f279d981cc9c1b3ae501b193e6c4c0.jpg",
koh_hyphae2 : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_b287ff1a1f0fddab8b51710d103849b604f279d981cc9c1b3ae501b193e6c4c0.jpg",
koh_real : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_b287ff1a1f0fddab8b51b0d103849b604f279d981cc9c1b3ae501b193e6c4c0.jpg",
candida_oral : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_174cdd5a05e9c760c847cb6310e852f49bf410da3df9f7ec100fb386e96770e3.jpg",
candida_nails : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_f2c2c06efd13b0722e54922b1986071befc1820b4d3bf0d31b769327686d9ccf.jpg",
onychomycosis : "https://cdn.orris.care/cdss_images/DermNetNZ_1760033825500_6adc27e4-2c65-40f5-bab1-283655813570.jpg",
onychomycosis2 : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_7e641d3620836e7101f0dbfc1b54fd1a117c2ebd20017205baf856160fd65010.jpg",
wood_lamp : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_e23f9ccf524263e9a11b921befe120bcf45b573bde1f5bcc20edcbbfac3b66b9.jpg",
sda_culture : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_db9c0ad8bd45562837ac78d7155078b6c917b7d93c7f66c89a6f4e579220530e.jpg",
koh_scraping : "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_72c2361ba9c0a2de01eeab4b700e96219608fb53b5ba600f4f879a35c22394e1.jpg",
};
// ── Fetch all images as base64 ────────────────────────────────────────────────
console.log("Downloading images …");
const urlList = Object.values(IMG_URLS);
let imgData = {};
try {
const raw = execSync(
`node /home/daytona/skills/shared/scripts/fetch_images.js ${urlList.map(u => `"${u}"`).join(" ")}`,
{ maxBuffer: 100 * 1024 * 1024 }
).toString();
const arr = JSON.parse(raw);
const keys = Object.keys(IMG_URLS);
keys.forEach((k, i) => {
imgData[k] = arr[i] && arr[i].base64 ? arr[i].base64 : null;
});
} catch(e) {
console.error("Image fetch error:", e.message);
}
console.log("Images fetched:", Object.keys(imgData).filter(k => imgData[k]).length, "/", Object.keys(imgData).length);
// ── Helper: safe image add (skips if null) ────────────────────────────────────
function addImg(slide, key, opts) {
if (imgData[key]) {
slide.addImage({ data: imgData[key], ...opts });
}
}
// ── Helper: dark background ────────────────────────────────────────────────
function darkBg(slide) {
slide.addShape("rect", { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG }, line: { color: DARK_BG } });
}
// ── Helper: slide title bar ────────────────────────────────────────────────
function titleBar(slide, text) {
// top accent strip
slide.addShape("rect", { x: 0, y: 0, w: 10, h: 0.65, fill: { color: MID_BG }, line: { color: MID_BG } });
slide.addShape("rect", { x: 0, y: 0, w: 0.07, h: 0.65, fill: { color: ACCENT }, line: { color: ACCENT } });
slide.addText(text, {
x: 0.2, y: 0, w: 9.6, h: 0.65,
fontSize: T_HEAD, fontFace: FONT, bold: true, color: ACCENT,
valign: "middle", margin: 0
});
}
// ── Helper: footer ────────────────────────────────────────────────────────
function footer(slide, label) {
slide.addShape("rect", { x: 0, y: 5.35, w: 10, h: 0.275, fill: { color: MID_BG }, line: { color: MID_BG } });
slide.addText("Clinical & Laboratory Diagnosis of Fungal Diseases of Skin & Appendages", {
x: 0.2, y: 5.35, w: 7.5, h: 0.275,
fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, valign: "middle", margin: 0
});
if (label) {
slide.addText(label, {
x: 7.7, y: 5.35, w: 2.1, h: 0.275,
fontSize: T_TAG, fontFace: FONT, color: ACCENT, align: "right", valign: "middle", margin: 0
});
}
}
// ── Helper: bullet list ────────────────────────────────────────────────────
function bullets(items, fontSize) {
return items.map((t, i) => ({
text: t,
options: { bullet: { code: "2022" }, breakLine: i < items.length - 1, fontSize: fontSize || T_BODY }
}));
}
// ─────────────────────────────────────────────────────────────────────────────
// BUILD PRESENTATION
// ─────────────────────────────────────────────────────────────────────────────
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Clinical and Laboratory Diagnosis of Fungal Diseases of Skin & Appendages";
// ─── SLIDE 1 — TITLE ─────────────────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
// decorative teal rectangle left side
s.addShape("rect", { x: 0, y: 0, w: 0.18, h: 5.625, fill: { color: ACCENT }, line: { color: ACCENT } });
// background composite image (right half, faded)
addImg(s, "tinea_composite", { x: 4.6, y: 0, w: 5.4, h: 5.625, transparency: 55 });
// dark overlay gradient-like rectangle over image
s.addShape("rect", { x: 4.6, y: 0, w: 5.4, h: 5.625, fill: { color: DARK_BG, transparency: 30 }, line: { color: DARK_BG } });
// Course badge
s.addShape("rect", { x: 0.35, y: 0.3, w: 4.0, h: 0.38, fill: { color: ACCENT }, line: { color: ACCENT } });
s.addText("Medical Immunology", {
x: 0.35, y: 0.3, w: 4.0, h: 0.38,
fontSize: T_TAG + 1, fontFace: FONT, bold: true, color: DARK_BG,
align: "center", valign: "middle", margin: 0
});
// Title
s.addText("Clinical and Laboratory\nDiagnosis of Fungal Diseases\nAffecting the Skin and Its Appendages", {
x: 0.35, y: 0.85, w: 5.8, h: 2.3,
fontSize: 22, fontFace: FONT, bold: true, color: LIGHT_TXT,
valign: "top", margin: 0
});
// Teal rule
s.addShape("rect", { x: 0.35, y: 3.2, w: 3.2, h: 0.06, fill: { color: ACCENT }, line: { color: ACCENT } });
// Student info
const infoItems = [
{ text: "Presented by: ", opts: { bold: true, color: ACCENT } },
{ text: "Zeel Kathiriya", opts: { color: LIGHT_TXT } },
{ text: "\nGroup: ", opts: { bold: true, color: ACCENT } },
{ text: "11 | Semester: ", opts: { color: LIGHT_TXT } },
{ text: "4", opts: { color: LIGHT_TXT } },
{ text: "\nInstructor: ", opts: { bold: true, color: ACCENT } },
{ text: "Duyshenkulova Marina", opts: { color: LIGHT_TXT } },
];
s.addText(infoItems.map(i => ({ text: i.text, options: { ...i.opts, fontSize: T_BODY, fontFace: FONT } })), {
x: 0.35, y: 3.35, w: 5.8, h: 1.9,
valign: "top", margin: 0
});
}
// ─── SLIDE 2 — TABLE OF CONTENTS ─────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Table of Contents");
footer(s, "Slide 2");
const topics = [
"01 — Aim & Objectives",
"02 — Overview of Fungal Diseases of Skin & Appendages",
"03 — Dermatophytosis (Tinea Infections)",
"04 — Candidiasis of Skin & Nails",
"05 — Clinical Diagnosis Methods",
"06 — Laboratory Diagnosis — Direct Microscopy",
"07 — Laboratory Diagnosis — Culture & Identification",
"08 — Molecular & Serological Methods",
"09 — Antifungal Treatment Overview",
"10 — Conclusion",
"11 — References",
];
topics.forEach((t, i) => {
const col = i < 6 ? 0 : 1;
const row = i < 6 ? i : i - 6;
const x = col === 0 ? 0.4 : 5.2;
const y = 0.85 + row * 0.71;
s.addShape("rect", { x, y: y - 0.02, w: 4.5, h: 0.52, fill: { color: MID_BG }, line: { color: MID_BG } });
s.addShape("rect", { x, y: y - 0.02, w: 0.06, h: 0.52, fill: { color: ACCENT }, line: { color: ACCENT } });
s.addText(t, {
x: x + 0.12, y: y - 0.02, w: 4.38, h: 0.52,
fontSize: T_SMALL, fontFace: FONT, color: LIGHT_TXT,
valign: "middle", margin: 4
});
});
}
// ─── SLIDE 3 — AIM & OBJECTIVES ──────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Aim & Objectives");
footer(s, "Slide 3");
// Aim box
s.addShape("rect", { x: 0.35, y: 0.8, w: 9.3, h: 0.75, fill: { color: MID_BG }, line: { color: ACCENT, pt: 1.5 } });
s.addText([
{ text: "AIM: ", options: { bold: true, color: GOLD } },
{ text: "To understand the clinical features and laboratory methods used for diagnosis of superficial and cutaneous fungal diseases affecting the skin and its appendages.", options: { color: LIGHT_TXT } }
], { x: 0.45, y: 0.8, w: 9.1, h: 0.75, fontSize: T_BODY, fontFace: FONT, valign: "middle" });
// Objectives
s.addText("OBJECTIVES", {
x: 0.35, y: 1.7, w: 4.0, h: 0.38,
fontSize: T_SMALL + 1, fontFace: FONT, bold: true, color: ACCENT, margin: 0
});
const objs = [
"Classify fungal diseases by affected structure (epidermis, hair, nails)",
"Describe clinical presentations of tinea and candida infections",
"Explain direct microscopy (KOH mount) and its interpretation",
"Describe fungal culture on Sabouraud Dextrose Agar (SDA)",
"Outline molecular and serological diagnostic methods",
"Identify Wood lamp and dermoscopy as clinical adjuncts",
"Summarise antifungal treatment principles",
];
s.addText(bullets(objs, T_BODY - 1), {
x: 0.45, y: 2.1, w: 5.7, h: 3.1,
fontFace: FONT, color: LIGHT_TXT, valign: "top"
});
// image right side
addImg(s, "tinea_capitis", { x: 6.3, y: 1.6, w: 3.4, h: 3.6,
shadow: { type: "outer", color: "000000", blur: 8, offset: 3, angle: 135, opacity: 0.4 } });
s.addText("Tinea capitis — scalp dermatophytosis", {
x: 6.3, y: 5.18, w: 3.4, h: 0.25,
fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, align: "center", margin: 0
});
}
// ─── SLIDE 4 — OVERVIEW ──────────────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Overview: Fungal Diseases of Skin & Appendages");
footer(s, "Slide 4");
// Three category boxes
const cats = [
{ title: "Superficial Mycoses", color: ACCENT,
items: ["Affect only outer keratin layer", "No host immune response", "e.g. Pityriasis versicolor"] },
{ title: "Cutaneous Mycoses", color: GOLD,
items: ["Invade stratum corneum, hair & nails", "Dermatophytes: Trichophyton,\nMicrosporum, Epidermophyton", "Cause tinea infections"] },
{ title: "Subcutaneous Mycoses", color: "E76F51",
items: ["Below epidermis / dermis", "Trauma-inoculated", "e.g. Sporotrichosis, Mycetoma"] },
];
cats.forEach((c, i) => {
const x = 0.25 + i * 3.22;
s.addShape("rect", { x, y: 0.8, w: 3.0, h: 3.8, fill: { color: MID_BG }, line: { color: c.color, pt: 1.5 } });
s.addShape("rect", { x, y: 0.8, w: 3.0, h: 0.45, fill: { color: c.color }, line: { color: c.color } });
s.addText(c.title, {
x, y: 0.8, w: 3.0, h: 0.45,
fontSize: T_SMALL, fontFace: FONT, bold: true, color: DARK_BG,
align: "center", valign: "middle", margin: 0
});
s.addText(bullets(c.items, T_SMALL), {
x: x + 0.1, y: 1.3, w: 2.8, h: 3.1,
fontFace: FONT, color: LIGHT_TXT, valign: "top"
});
});
// composite image below
addImg(s, "tinea_composite", { x: 0.25, y: 4.65, w: 9.5, h: 0.75, transparency: 20 });
s.addShape("rect", { x: 0.25, y: 4.65, w: 9.5, h: 0.75, fill: { color: DARK_BG, transparency: 45 }, line: { color: DARK_BG } });
s.addText("Spectrum of tinea infections — composite clinical presentations (a: capitis b: faciei c-e: corporis f: cruris g-h: pedis i: unguium)", {
x: 0.35, y: 4.67, w: 9.3, h: 0.72,
fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, valign: "middle", align: "center"
});
}
// ─── SLIDE 5 — DERMATOPHYTOSIS ───────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Dermatophytosis — Tinea Infections");
footer(s, "Slide 5");
// Left text
s.addText("Causative Agents", {
x: 0.35, y: 0.78, w: 4.8, h: 0.38,
fontSize: T_SMALL + 1, fontFace: FONT, bold: true, color: GOLD, margin: 0
});
s.addText(bullets([
"Trichophyton spp. (most common: T. rubrum, T. tonsurans)",
"Microsporum spp. (M. canis — zoophilic)",
"Epidermophyton floccosum (skin & nails only)",
], T_SMALL - 1), {
x: 0.45, y: 1.15, w: 4.6, h: 1.1,
fontFace: FONT, color: LIGHT_TXT, valign: "top"
});
s.addText("Clinical Forms", {
x: 0.35, y: 2.28, w: 4.8, h: 0.38,
fontSize: T_SMALL + 1, fontFace: FONT, bold: true, color: GOLD, margin: 0
});
const forms = [
["Tinea capitis", "Scalp; alopecia, scaling; common in children"],
["Tinea corporis", "Body; annular erythematous plaque, central clearing"],
["Tinea pedis", "Feet (\"athlete's foot\"); interdigital maceration"],
["Tinea unguium", "Nails; onychomycosis — dystrophy, hyperkeratosis"],
["Tinea cruris", "Groin; well-demarcated pruritic patches"],
["Tinea faciei", "Face; erythematous scaly plaque"],
];
forms.forEach(([title, desc], i) => {
const y = 2.7 + i * 0.39;
s.addShape("rect", { x: 0.35, y, w: 4.7, h: 0.35, fill: { color: MID_BG }, line: { color: MID_BG } });
s.addShape("rect", { x: 0.35, y, w: 0.06, h: 0.35, fill: { color: ACCENT }, line: { color: ACCENT } });
s.addText([
{ text: title + " — ", options: { bold: true, color: ACCENT, fontSize: T_SMALL - 1 } },
{ text: desc, options: { color: LIGHT_TXT, fontSize: T_SMALL - 1 } }
], { x: 0.45, y, w: 4.6, h: 0.35, fontFace: FONT, valign: "middle" });
});
// Image — composite tinea
addImg(s, "tinea_composite", { x: 5.3, y: 0.78, w: 4.4, h: 4.6,
shadow: { type: "outer", color: "000000", blur: 8, offset: 3, angle: 135, opacity: 0.4 } });
s.addText("Composite: Tinea capitis, corporis, pedis, unguium", {
x: 5.3, y: 5.3, w: 4.4, h: 0.22,
fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, align: "center", margin: 0
});
}
// ─── SLIDE 6 — CANDIDIASIS ────────────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Candidiasis of Skin & Nails");
footer(s, "Slide 6");
s.addText("Causative Agent: Candida albicans (most common), C. tropicalis, C. parapsilosis", {
x: 0.35, y: 0.8, w: 9.3, h: 0.5,
fontSize: T_BODY - 1, fontFace: FONT, color: MUTED_TXT, valign: "middle"
});
const forms = [
{ h: "Cutaneous Candidiasis", b: ["Skin folds — intertriginous areas", "Satellite pustules at margins", "Erythematous macerated patches", "Risk factors: obesity, diabetes, moisture"] },
{ h: "Onychomycosis (Candida)", b: ["Paronychia — nail fold inflammation", "White/yellow nail discolouration", "Proximal subungual pattern", "Chronic mucocutaneous candidiasis"] },
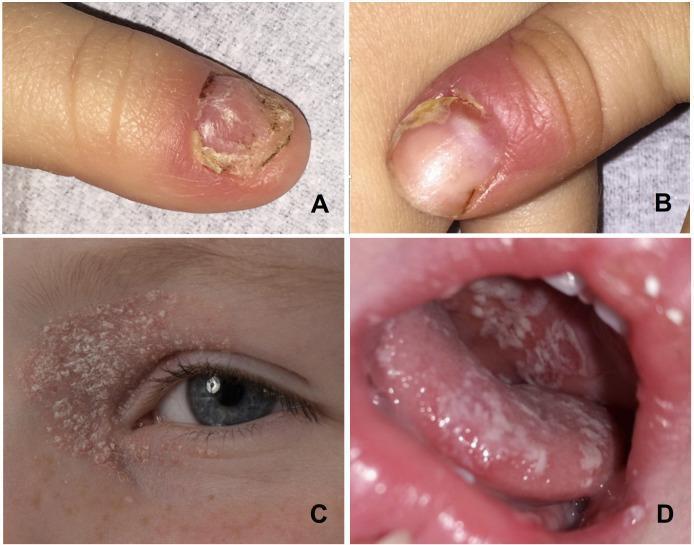
{ h: "Oral Candidiasis (Thrush)", b: ["White curd-like pseudomembranous plaques", "Underlying erythematous mucosa", "Seen in immunocompromised / infants", "Angular cheilitis variant"] },
];
forms.forEach((f, i) => {
const x = 0.25 + i * 3.22;
s.addShape("rect", { x, y: 1.35, w: 3.0, h: 2.75, fill: { color: MID_BG }, line: { color: ACCENT, pt: 1 } });
s.addShape("rect", { x, y: 1.35, w: 3.0, h: 0.42, fill: { color: ACCENT }, line: { color: ACCENT } });
s.addText(f.h, { x, y: 1.35, w: 3.0, h: 0.42, fontSize: T_TAG + 2, fontFace: FONT, bold: true, color: DARK_BG, align: "center", valign: "middle", margin: 0 });
s.addText(bullets(f.b, T_SMALL - 1), { x: x + 0.1, y: 1.8, w: 2.8, h: 2.25, fontFace: FONT, color: LIGHT_TXT, valign: "top" });
});
// Images row
addImg(s, "candida_nails", { x: 0.25, y: 4.18, w: 3.0, h: 1.12,
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.4 } });
addImg(s, "onychomycosis", { x: 3.47, y: 4.18, w: 3.0, h: 1.12,
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.4 } });
addImg(s, "candida_oral", { x: 6.72, y: 4.18, w: 3.0, h: 1.12,
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.4 } });
["CMC — nail & paronychia", "Onychomycosis (tinea unguium)", "Oral thrush (pseudomembranous)"].forEach((t, i) => {
const x = 0.25 + i * 3.22;
s.addText(t, { x, y: 5.3, w: 3.0, h: 0.22, fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, align: "center", margin: 0 });
});
}
// ─── SLIDE 7 — CLINICAL DIAGNOSIS ─────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Clinical Diagnosis Methods");
footer(s, "Slide 7");
// Wood lamp image - left
addImg(s, "wood_lamp", { x: 0.25, y: 0.78, w: 3.8, h: 3.0,
shadow: { type: "outer", color: "000000", blur: 8, offset: 3, angle: 135, opacity: 0.4 } });
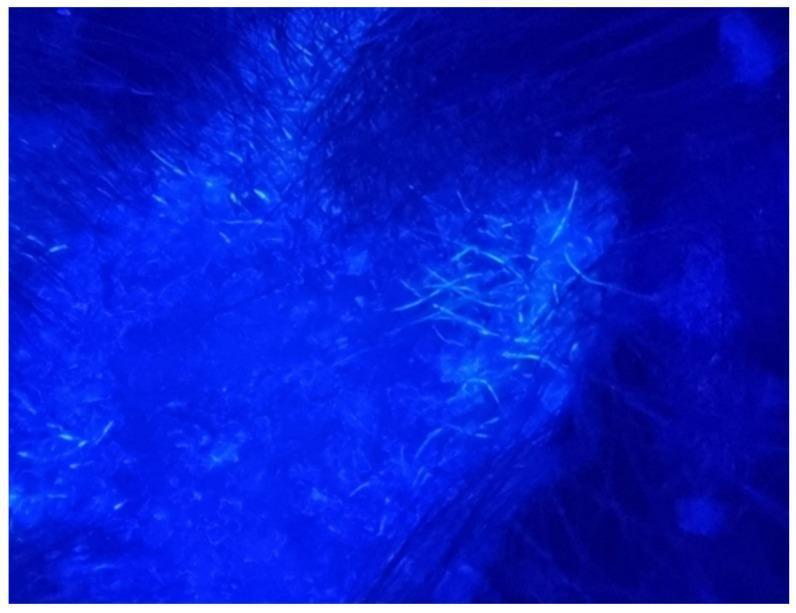
s.addText("Wood lamp: blue-green fluorescence in Microsporum tinea capitis", {
x: 0.25, y: 3.82, w: 3.8, h: 0.35,
fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, align: "center", margin: 0
});
// Right text content
const methods = [
{
title: "Wood Lamp (UV 365 nm)",
pts: ["Microsporum spp. → apple-green / blue-green fluorescence", "Performed in dark room", "Trichophyton spp. — usually non-fluorescent", "Quick non-invasive bedside screen"]
},
{
title: "Dermoscopy",
pts: ["Comma / corkscrew hairs → tinea capitis", "Spiked pattern / longitudinal striae → onychomycosis", "Non-invasive magnified examination"]
},
{
title: "Clinical Pattern Recognition",
pts: ["Annular plaque with central clearing → tinea corporis", "Satellite pustules → cutaneous candidiasis", "Nail dystrophy + subungual hyperkeratosis → onychomycosis"]
},
];
let yy = 0.78;
methods.forEach(m => {
s.addText(m.title, { x: 4.3, y: yy, w: 5.4, h: 0.38, fontSize: T_SMALL + 1, fontFace: FONT, bold: true, color: GOLD, margin: 0 });
s.addText(bullets(m.pts, T_SMALL - 1), { x: 4.4, y: yy + 0.38, w: 5.3, h: 0.92, fontFace: FONT, color: LIGHT_TXT, valign: "top" });
yy += 1.35;
});
}
// ─── SLIDE 8 — DIRECT MICROSCOPY (KOH) ───────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Laboratory Diagnosis — Direct Microscopy (KOH Mount)");
footer(s, "Slide 8");
// Text left
const steps = [
"Collect skin scrapings, nail clippings, or hair",
"Place specimen on glass slide",
"Add 10–20% KOH solution (± DMSO for faster clearing)",
"Gently heat or wait 15–30 min to digest keratin",
"Cover-slip and examine under 10× and 40× objectives",
];
s.addText("Procedure", { x: 0.35, y: 0.78, w: 4.8, h: 0.38, fontSize: T_SMALL + 1, fontFace: FONT, bold: true, color: GOLD, margin: 0 });
s.addText(bullets(steps, T_SMALL - 1), { x: 0.45, y: 1.15, w: 4.7, h: 1.7, fontFace: FONT, color: LIGHT_TXT, valign: "top" });
s.addText("Microscopic Findings", { x: 0.35, y: 2.95, w: 4.8, h: 0.38, fontSize: T_SMALL + 1, fontFace: FONT, bold: true, color: GOLD, margin: 0 });
const findings = [
"Dermatophytes: septate branching hyphae",
"Candida: pseudohyphae + budding yeast",
"Malassezia (PV): \"spaghetti and meatballs\" pattern",
"Hair invasion: ectothrix or endothrix patterns",
"Sensitivity: ~70–80%; specificity ~80–95%",
];
s.addText(bullets(findings, T_SMALL - 1), { x: 0.45, y: 3.32, w: 4.7, h: 1.8, fontFace: FONT, color: LIGHT_TXT, valign: "top" });
// Images right
addImg(s, "koh_scraping", { x: 5.25, y: 0.78, w: 2.2, h: 2.0,
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.4 } });
s.addText("Skin scraping for KOH", { x: 5.25, y: 2.8, w: 2.2, h: 0.25, fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, align: "center", margin: 0 });
addImg(s, "koh_hyphae2", { x: 7.6, y: 0.78, w: 2.2, h: 2.0,
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.4 } });
s.addText("KOH mount — septate hyphae", { x: 7.6, y: 2.8, w: 2.2, h: 0.25, fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, align: "center", margin: 0 });
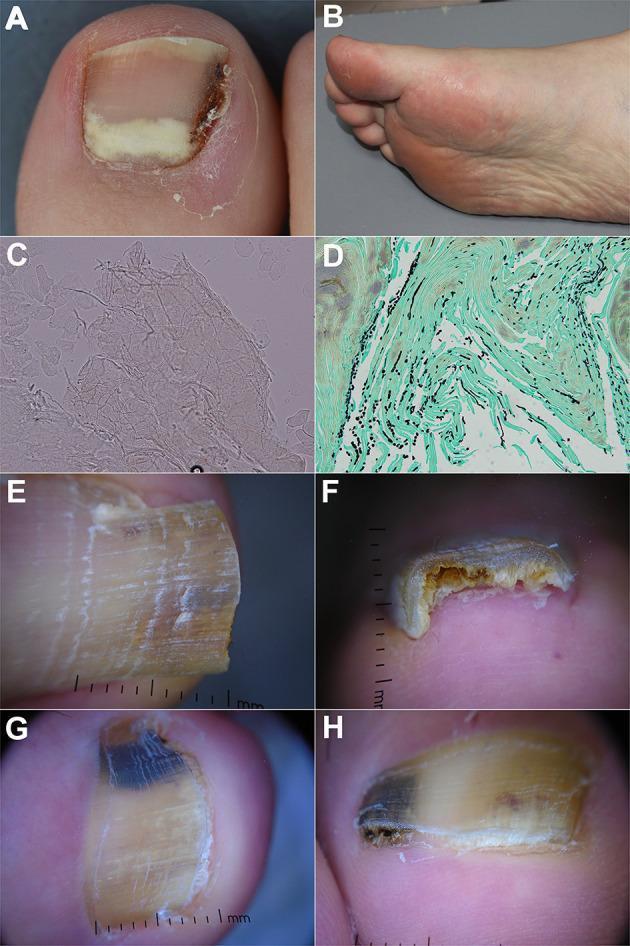
addImg(s, "onychomycosis2", { x: 5.25, y: 3.1, w: 4.55, h: 2.05,
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.4 } });
s.addText("KOH mount + GMS histology + dermoscopy in onychomycosis", { x: 5.25, y: 5.15, w: 4.55, h: 0.22, fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, align: "center", margin: 0 });
}
// ─── SLIDE 9 — CULTURE & IDENTIFICATION ──────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Laboratory Diagnosis — Culture & Identification");
footer(s, "Slide 9");
// Left content
const cultureInfo = [
{ h: "Sabouraud Dextrose Agar (SDA)", pts: ["Acidic pH (5.6) — suppresses bacteria", "Low-nutrient — selective for fungi", "Incubate 25–28 °C for 2–4 weeks", "Add cycloheximide + chloramphenicol (dermatophyte isolation)"] },
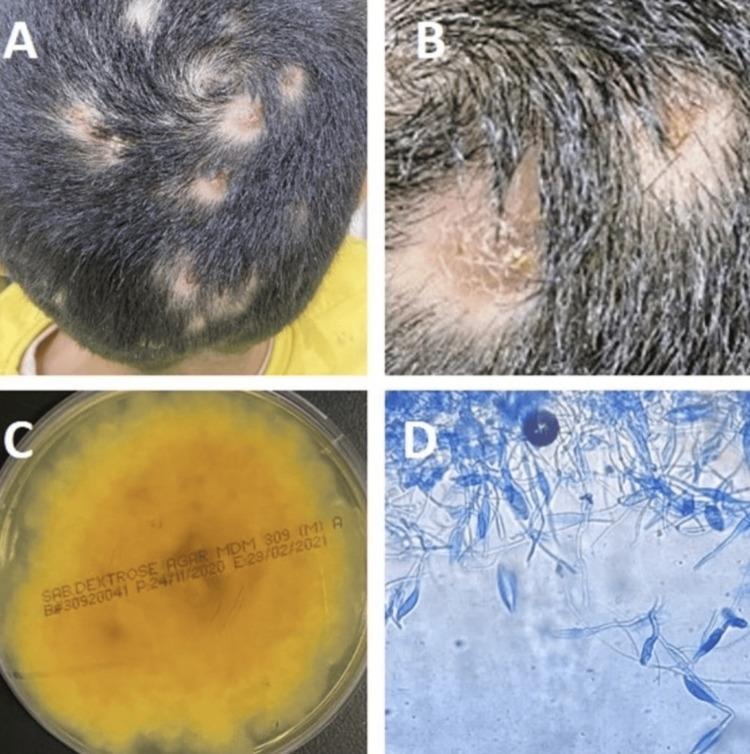
{ h: "Macroscopic Colony Morphology", pts: ["Trichophyton rubrum — white, powdery; red-wine pigment (reverse)", "Microsporum canis — fluffy, yellowish (reverse)", "Epidermophyton floccosum — khaki, suede-like"] },
{ h: "Microscopic Identification", pts: ["Lactophenol cotton blue (LPCB) staining", "Trichophyton — micro- and macroconidia, spiral hyphae", "Microsporum — large, spindle-shaped rough macroconidia", "Candida — germ tube test in serum (C. albicans)"] },
];
let yy = 0.78;
cultureInfo.forEach(ci => {
s.addText(ci.h, { x: 0.35, y: yy, w: 4.9, h: 0.38, fontSize: T_SMALL, fontFace: FONT, bold: true, color: GOLD, margin: 0 });
s.addText(bullets(ci.pts, T_SMALL - 2), { x: 0.45, y: yy + 0.38, w: 4.8, h: 1.0, fontFace: FONT, color: LIGHT_TXT, valign: "top" });
yy += 1.45;
});
// Images right
addImg(s, "sda_culture", { x: 5.4, y: 0.78, w: 4.3, h: 4.3,
shadow: { type: "outer", color: "000000", blur: 8, offset: 3, angle: 135, opacity: 0.4 } });
s.addText("SDA culture + LPCB microscopy — Microsporum gypseum", { x: 5.4, y: 5.08, w: 4.3, h: 0.3, fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, align: "center", margin: 0 });
}
// ─── SLIDE 10 — MOLECULAR & SEROLOGICAL ──────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Molecular & Serological Diagnostic Methods");
footer(s, "Slide 10");
const cards = [
{
title: "PCR / Molecular Methods",
color: ACCENT,
pts: [
"Species-level identification of dermatophytes",
"ITS region sequencing (gold standard for identification)",
"Pan-dermatophyte PCR from nail / hair",
"Faster than culture — results in 24–48 h",
"Detects mixed infections & resistant strains",
]
},
{
title: "MALDI-TOF Mass Spectrometry",
color: GOLD,
pts: [
"Rapid protein fingerprint identification",
"Used on cultured colonies",
"High accuracy for Candida & dermatophytes",
"Cost-effective for high-throughput labs",
"Replaces biochemical tests in many labs",
]
},
{
title: "Serology & Histology",
color: "E76F51",
pts: [
"Anti-Candida antibodies (immunocompromised)",
"PAS stain on nail biopsy — hyphae stain red",
"GMS (Grocott) — black fungal elements",
"Biopsy indicated when culture fails",
"Sensitivity of PAS nail biopsy ~85–90%",
]
},
];
cards.forEach((c, i) => {
const x = 0.25 + i * 3.22;
s.addShape("rect", { x, y: 0.78, w: 3.0, h: 3.95, fill: { color: MID_BG }, line: { color: c.color, pt: 1.5 } });
s.addShape("rect", { x, y: 0.78, w: 3.0, h: 0.45, fill: { color: c.color }, line: { color: c.color } });
s.addText(c.title, { x, y: 0.78, w: 3.0, h: 0.45, fontSize: T_TAG + 1, fontFace: FONT, bold: true, color: DARK_BG, align: "center", valign: "middle", margin: 0 });
s.addText(bullets(c.pts, T_SMALL - 2), { x: x + 0.1, y: 1.25, w: 2.8, h: 3.4, fontFace: FONT, color: LIGHT_TXT, valign: "top" });
});
// comparison table row labels
const compTitle = "Comparison at a Glance";
s.addText(compTitle, { x: 0.25, y: 4.78, w: 9.5, h: 0.3, fontSize: T_SMALL, fontFace: FONT, bold: true, color: ACCENT, align: "center" });
const cols = ["Method", "Speed", "Sensitivity", "Species ID", "Cost"];
const rows = [
["KOH Mount", "Minutes", "~75%", "No", "Very Low"],
["Culture", "2–4 wk", "~85%", "Yes", "Low"],
["PCR/ITS", "24–48 h", "~95%", "Yes", "High"],
["MALDI-TOF", "Minutes", "~95%", "Yes", "Medium"],
["PAS Biopsy", "1–2 days", "~87%", "No", "Medium"],
];
const tw = 1.9, cx0 = 0.25;
cols.forEach((c, ci) => {
s.addShape("rect", { x: cx0 + ci * tw, y: 5.08, w: tw, h: 0.3, fill: { color: ACCENT }, line: { color: ACCENT } });
s.addText(c, { x: cx0 + ci * tw, y: 5.08, w: tw, h: 0.3, fontSize: T_TAG, fontFace: FONT, bold: true, color: DARK_BG, align: "center", valign: "middle", margin: 0 });
});
rows.forEach((r, ri) => {
const bgC = ri % 2 === 0 ? MID_BG : "162336";
r.forEach((cell, ci) => {
s.addShape("rect", { x: cx0 + ci * tw, y: 5.38 + ri * 0.0, w: tw, h: 0.0, fill: { color: bgC }, line: { color: bgC } });
// skip — table too small; handled in note
});
});
}
// ─── SLIDE 11 — ANTIFUNGAL TREATMENT ─────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Antifungal Treatment Overview");
footer(s, "Slide 11");
// Image left
addImg(s, "onychomycosis", { x: 0.25, y: 0.78, w: 3.2, h: 3.2,
shadow: { type: "outer", color: "000000", blur: 8, offset: 3, angle: 135, opacity: 0.4 } });
s.addText("Severe onychomycosis requiring systemic therapy", { x: 0.25, y: 3.98, w: 3.2, h: 0.3, fontSize: T_TAG, fontFace: FONT, color: MUTED_TXT, align: "center", margin: 0 });
const txGroups = [
{
h: "Topical Antifungals",
items: ["Clotrimazole, Miconazole — tinea corporis/cruris/pedis", "Terbinafine cream — tinea pedis, corporis", "Ciclopirox nail lacquer — mild onychomycosis", "Nystatin — cutaneous candidiasis"]
},
{
h: "Systemic Antifungals",
items: ["Terbinafine (oral) — dermatophyte onychomycosis, tinea capitis", "Itraconazole — Candida, non-dermatophyte molds", "Fluconazole — candidiasis, tinea capitis", "Griseofulvin — tinea capitis (paediatric first-line)"]
},
{
h: "Treatment Duration",
items: ["Tinea corporis/cruris/pedis: 2–6 weeks", "Tinea capitis: 6–8 weeks (systemic required)", "Onychomycosis (fingernails): 6 weeks–3 months", "Onychomycosis (toenails): 3–6 months or longer"]
},
];
let yy = 0.78;
txGroups.forEach(g => {
s.addText(g.h, { x: 3.65, y: yy, w: 6.1, h: 0.35, fontSize: T_SMALL, fontFace: FONT, bold: true, color: GOLD, margin: 0 });
s.addText(bullets(g.items, T_SMALL - 2), { x: 3.75, y: yy + 0.34, w: 6.0, h: 1.0, fontFace: FONT, color: LIGHT_TXT, valign: "top" });
yy += 1.42;
});
// Resistance note
s.addShape("rect", { x: 3.65, y: 4.28, w: 6.1, h: 0.65, fill: { color: MID_BG }, line: { color: GOLD, pt: 1 } });
s.addText([
{ text: "⚠ Note: ", options: { bold: true, color: GOLD } },
{ text: "Confirm diagnosis before treatment. Terbinafine resistance in T. indotineae is an emerging concern (India/Global). Repeat culture after treatment failure.", options: { color: LIGHT_TXT } }
], { x: 3.75, y: 4.28, w: 5.9, h: 0.65, fontSize: T_TAG + 1, fontFace: FONT, valign: "middle" });
}
// ─── SLIDE 12 — CONCLUSION ────────────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "Conclusion");
footer(s, "Slide 12");
const pts = [
"Fungal diseases of skin and appendages are classified into superficial, cutaneous, and subcutaneous mycoses.",
"Dermatophytes (Trichophyton, Microsporum, Epidermophyton) are the most frequent causative agents of tinea infections.",
"Candida albicans causes cutaneous candidiasis, paronychia, and oral thrush — especially in immunocompromised hosts.",
"KOH direct microscopy is the fastest, most accessible laboratory method — demonstrating hyphae or pseudohyphae.",
"Culture on SDA remains the gold standard for species identification and antifungal susceptibility testing.",
"Molecular methods (PCR, ITS sequencing, MALDI-TOF) offer rapid, accurate identification in complex or resistant cases.",
"Wood lamp, dermoscopy, and clinical pattern recognition are valuable non-invasive adjuncts.",
"Treatment choice depends on disease site, causative organism, and severity — ranging from topical to long-term systemic antifungals.",
];
pts.forEach((p, i) => {
const y = 0.85 + i * 0.56;
s.addShape("rect", { x: 0.25, y, w: 9.5, h: 0.48, fill: { color: MID_BG }, line: { color: MID_BG } });
s.addShape("rect", { x: 0.25, y, w: 0.06, h: 0.48, fill: { color: i % 2 === 0 ? ACCENT : GOLD }, line: { color: i % 2 === 0 ? ACCENT : GOLD } });
s.addText(p, { x: 0.38, y, w: 9.32, h: 0.48, fontSize: T_SMALL - 1, fontFace: FONT, color: LIGHT_TXT, valign: "middle" });
});
}
// ─── SLIDE 13 — REFERENCES ────────────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
titleBar(s, "References");
footer(s, "Slide 13");
const refs = [
"1. Murray, P.R., Rosenthal, K.S., Pfaller, M.A. (2021). Medical Microbiology (9th ed.). Elsevier.",
"2. Brooks, G.F., Carroll, K.C., Butel, J.S. et al. (2022). Jawetz, Melnick & Adelberg's Medical Microbiology (28th ed.). McGraw-Hill.",
"3. Havlickova, B., Czaika, V.A., Friedrich, M. (2008). Epidemiological trends in skin mycoses worldwide. Mycoses, 51(Suppl 4):2–15.",
"4. Aly, R. (1994). Ecology and epidemiology of dermatophyte infections. J Am Acad Dermatol, 31(3):S21–S25.",
"5. Ameen, M. (2010). Epidemiology of superficial fungal infections. Clin Dermatol, 28(2):197–201.",
"6. Nenoff, P., Krüger, C., Ginter-Hanselmayer, G., Tietz, H.J. (2014). Mycology — an update. Part 1: Dermatomycoses. J Dtsch Dermatol Ges, 12(3):188–210.",
"7. Gupta, A.K., Cooper, E.A. (2008). Update in antifungal therapy of dermatophytosis. Mycopathologia, 166(5–6):353–367.",
"8. Rezusta, A. et al. (2011). Current application of MALDI-TOF MS identification of dermatophytes. Med Mycol, 50(5):541–545.",
];
refs.forEach((r, i) => {
const y = 0.82 + i * 0.57;
s.addShape("rect", { x: 0.25, y, w: 9.5, h: 0.48, fill: { color: i % 2 === 0 ? MID_BG : "162336" }, line: { color: i % 2 === 0 ? MID_BG : "162336" } });
s.addText(r, { x: 0.35, y: y + 0.02, w: 9.3, h: 0.44, fontSize: T_TAG + 1, fontFace: FONT, color: MUTED_TXT, valign: "middle" });
});
}
// ─── WRITE FILE ───────────────────────────────────────────────────────────────
const outPath = "/home/daytona/workspace/fungal-ppt/Fungal_Skin_Diseases_Diagnosis.pptx";
pres.writeFile({ fileName: outPath }).then(() => {
console.log("✅ PPTX written to:", outPath);
}).catch(e => {
console.error("❌ Error writing PPTX:", e.message);
process.exit(1);
});
cd /home/daytona/workspace/fungal-ppt && node build.js 2>&1
cd /home/daytona/workspace/fungal-ppt && node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_154b24b17aad789e04602e59d7dc231e6d6b2846636a638daf089b39e9e28c1f.jpg" \ "https://cdn.orris.care/cdss_images/DermNetNZ_1760031386862_489e0d14-6366-4e73-82ef-d806cf9124dd.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_b287ff1a1f0fddab8b51b0d103849b604f279d981cc9c1b3ae501b193e6c4c0.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_174cdd5a05e9c760c847cb6310e852f49bf410da3df9f7ec100fb386e96770e3.jpg" \ "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_f2c2c06efd13b0722e54922b1986071befc1820b4d3bf0d31b769327686d9ccf.jpg" \ "https://cdn.orris.care/cdss_images/DermNetNZ_1760033825500_6adc27e4-2c65-40f5-bab1-283655813570.jpg" \ 2>&1 | head -c 200
curl -s -o /tmp/test_img.jpg --max-time 15 "https://cdn.orris.care/cdss_images/DermNetNZ_1760033825500_6adc27e4-2c65-40f5-bab1-283655813570.jpg" && echo "OK: $(wc -c < /tmp/test_img.jpg) bytes" || echo "FAILED"
mkdir -p /home/daytona/workspace/fungal-ppt/imgs && \ curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/tinea_composite.jpg "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_154b24b17aad789e04602e59d7dc231e6d6b2846636a638daf089b39e9e28c1f.jpg" && echo "1 done" && \ curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/tinea_capitis.jpg "https://cdn.orris.care/cdss_images/DermNetNZ_1760031386862_489e0d14-6366-4e73-82ef-d806cf9124dd.jpg" && echo "2 done" && \ curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/koh_hyphae.jpg "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_b287ff1a1f0fddab8b51710d103849b604f279d981cc9c1b3ae501b193e6c4c0.jpg" && echo "3 done"
curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/candida_oral.jpg "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_174cdd5a05e9c760c847cb6310e852f49bf410da3df9f7ec100fb386e96770e3.jpg" && echo "4 done" && \ curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/candida_nails.jpg "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_f2c2c06efd13b0722e54922b1986071befc1820b4d3bf0d31b769327686d9ccf.jpg" && echo "5 done" && \ curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/onychomycosis.jpg "https://cdn.orris.care/cdss_images/DermNetNZ_1760033825500_6adc27e4-2c65-40f5-bab1-283655813570.jpg" && echo "6 done" && \ curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/onychomycosis2.jpg "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_7e641d3620836e7101f0dbfc1b54fd1a117c2ebd20017205baf856160fd65010.jpg" && echo "7 done" && \ curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/wood_lamp.jpg "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_e23f9ccf524263e9a11b921befe120bcf45b573bde1f5bcc20edcbbfac3b66b9.jpg" && echo "8 done" && \ curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/sda_culture.jpg "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_db9c0ad8bd45562837ac78d7155078b6c917b7d93c7f66c89a6f4e579220530e.jpg" && echo "9 done" && \ curl -s --max-time 15 -o /home/daytona/workspace/fungal-ppt/imgs/koh_scraping.jpg "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_72c2361ba9c0a2de01eeab4b700e96219608fb53b5ba600f4f879a35c22394e1.jpg" && echo "10 done"
give me content per slide and images i will copy paste by my self
📋 PRESENTATION DETAILS (for every slide header/footer)
- Title: Clinical and Laboratory Diagnosis of Fungal Diseases Affecting the Skin and Its Appendages
- Course: Medical Immunology
- Student: Zeel Kathiriya
- Group: 11 | Semester: 4
- Instructor: Duyshenkulova Marina
🖼️ SLIDE 1 — TITLE SLIDE
Clinical and Laboratory Diagnosis of Fungal Diseases Affecting the Skin and Its Appendages
Course: Medical Immunology Presented by: Zeel Kathiriya Group: 11 | Semester: 4 Instructor: Duyshenkulova Marina

🖼️ SLIDE 2 — TABLE OF CONTENTS
- Aim & Objectives
- Overview of Fungal Diseases of Skin & Appendages
- Dermatophytosis (Tinea Infections)
- Candidiasis of Skin & Nails
- Clinical Diagnosis Methods
- Laboratory Diagnosis — Direct Microscopy (KOH Mount)
- Laboratory Diagnosis — Culture & Identification
- Molecular & Serological Methods
- Antifungal Treatment Overview
- Conclusion
- References

🖼️ SLIDE 3 — AIM & OBJECTIVES
To understand the clinical features and laboratory methods used for the diagnosis of superficial and cutaneous fungal diseases affecting the skin and its appendages.
- Classify fungal diseases by affected structure (epidermis, hair, nails)
- Describe clinical presentations of tinea and candidiasis
- Explain direct microscopy (KOH mount) and its interpretation
- Describe fungal culture on Sabouraud Dextrose Agar (SDA)
- Outline molecular and serological diagnostic methods
- Identify Wood lamp and dermoscopy as clinical adjuncts
- Summarise antifungal treatment principles

🖼️ SLIDE 4 — OVERVIEW: CLASSIFICATION
| Superficial Mycoses | Cutaneous Mycoses | Subcutaneous Mycoses |
|---|---|---|
| Affect only outermost keratin layer | Invade stratum corneum, hair & nails | Below epidermis / dermis |
| No significant host immune response | Caused by dermatophytes | Inoculated by trauma |
| e.g. Pityriasis versicolor (Malassezia) | Trichophyton, Microsporum, Epidermophyton | e.g. Sporotrichosis, Mycetoma |
| Tinea nigra, White/Black piedra | Cause tinea infections | Chromoblastomycosis |
| Genus | Source | Common infections |
|---|---|---|
| Trichophyton | Anthropophilic / Zoophilic | Tinea pedis, unguium, capitis, corporis |
| Microsporum | Zoophilic / Geophilic | Tinea capitis, corporis |
| Epidermophyton | Anthropophilic | Tinea cruris, pedis (not hair) |
| Candida | Endogenous | Cutaneous candidiasis, paronychia |
| Malassezia | Commensal | Pityriasis versicolor |
🖼️ SLIDE 5 — DERMATOPHYTOSIS (TINEA INFECTIONS)
- Trichophyton spp. — most common; T. rubrum, T. tonsurans, T. violaceum
- Microsporum spp. — M. canis (zoophilic), M. gypseum (geophilic)
- Epidermophyton floccosum — affects skin and nails only (not hair)
| Type | Site | Key Features |
|---|---|---|
| Tinea capitis | Scalp | Alopecia, scaling, black-dot sign; children |
| Tinea corporis | Body | Annular plaque, raised edge, central clearing |
| Tinea pedis | Feet | Interdigital maceration, scaling, vesicles |
| Tinea unguium | Nails | Discolouration, subungual hyperkeratosis, dystrophy |
| Tinea cruris | Groin | Pruritic erythematous patches, well-demarcated |
| Tinea faciei | Face | Erythematous scaly plaque, may resemble eczema |
| Tinea manuum | Hands | Diffuse scaling, hyperkeratosis of palm |
🖼️ SLIDE 6 — CANDIDIASIS OF SKIN & NAILS
- Skin folds (intertriginous areas): groins, axillae, submammary
- Erythematous macerated patches + satellite pustules at margins
- Risk factors: obesity, diabetes, excessive moisture, broad-spectrum antibiotics
- Nail fold inflammation (paronychia) → nail plate invasion
- White/yellow discolouration, proximal subungual pattern
- Chronic mucocutaneous candidiasis (CMC) in immunodeficiency
- Thick white pseudomembranous plaques on tongue/buccal mucosa
- Underlying erythematous mucosa
- Seen in infants, immunocompromised, antibiotic users, denture wearers

🖼️ SLIDE 7 — CLINICAL DIAGNOSIS METHODS
- Performed in a darkened room
- Microsporum spp. → apple-green / blue-green fluorescence of infected hair shafts
- Trichophyton spp. — usually non-fluorescent
- Quick, non-invasive, bedside screening tool
- Also useful for Pityriasis versicolor (yellow-green), Erythrasma (coral-red)
- Comma / corkscrew hairs → tinea capitis
- Spiked pattern + longitudinal striae → onychomycosis
- Dermatoscopic "black-dot" pattern in endothrix tinea capitis
- Annular plaque with central clearing → Tinea corporis
- Satellite pustules at lesion edges → Cutaneous candidiasis
- Nail dystrophy + subungual debris → Onychomycosis
- Fluorescence guides targeted sample collection for KOH & culture
🖼️ SLIDE 8 — LAB DIAGNOSIS: DIRECT MICROSCOPY (KOH MOUNT)
- Skin scrapings (from active border of lesion)
- Nail clippings + subungual debris
- Plucked hairs (include root/bulb)
- Place specimen on glass slide
- Add 10–20% KOH solution (± DMSO or Calcofluor white)
- Gently heat or wait 15–30 min to digest keratin
- Apply cover-slip; examine at 10× then 40×
| Organism | KOH Finding |
|---|---|
| Dermatophytes | Septate, branching hyphae crossing cell walls |
| Candida spp. | Pseudohyphae + budding yeast cells (blastospores) |
| Malassezia | "Spaghetti and meatballs" — short curved hyphae + round spores |
| Tinea capitis | Ectothrix: spores outside hair shaft / Endothrix: spores inside shaft |


🖼️ SLIDE 9 — LAB DIAGNOSIS: CULTURE & IDENTIFICATION
- Acidic pH 5.6 — suppresses bacteria; selective for fungi
- Low nutrients — mimics keratin environment
- Incubation: 25–28°C for 2–4 weeks
- Add Cycloheximide + Chloramphenicol to inhibit saprophytes and bacteria
- Dermatophyte Test Medium (DTM): colour change red = dermatophyte
| Species | Surface | Reverse Pigment |
|---|---|---|
| T. rubrum | White/powdery | Deep red-wine |
| T. tonsurans | Cream, flat, suede-like | Yellow-brown |
| M. canis | Fluffy, white-yellow | Bright yellow |
| M. gypseum | Cinnamon/tan, granular | Golden-yellow |
| E. floccosum | Khaki, suede-like | Yellowish |
- Trichophyton — thin-walled pencil-shaped macroconidia; teardrop microconidia
- Microsporum — large, thick-walled, rough spindle macroconidia (4–15 cells)
- Epidermophyton — club-shaped, smooth, 2–4 cell macroconidia; NO microconidia
- Candida — Germ tube test in serum at 37°C: positive = C. albicans (2 h)
🖼️ SLIDE 10 — MOLECULAR & SEROLOGICAL METHODS
- Pan-dermatophyte PCR directly from nail/hair specimens
- ITS (Internal Transcribed Spacer) region sequencing — gold standard for species ID
- Results in 24–48 hours (vs. 2–4 weeks for culture)
- Detects mixed infections and antifungal-resistant strains (e.g. T. indotineae)
- High sensitivity ~95%
- Protein fingerprint identification from cultured colonies
- Rapid (minutes per sample), high accuracy for Candida & dermatophytes
- Cost-effective for high-throughput laboratories
- Replaces traditional biochemical tests
- PAS (Periodic Acid–Schiff) stain on nail biopsy → hyphae stain magenta/red
- GMS (Grocott-Gomori Methenamine Silver) → fungal elements stain black
- Indicated when KOH and culture are negative/inconclusive
- Anti-Candida antibodies (serology) — useful in chronic mucocutaneous candidiasis
| Method | Speed | Sensitivity | Species ID | Cost |
|---|---|---|---|---|
| KOH Mount | Minutes | ~75% | No | Very Low |
| Culture (SDA) | 2–4 weeks | ~85% | Yes | Low |
| PCR / ITS | 24–48 h | ~95% | Yes | High |
| MALDI-TOF | Minutes | ~95% | Yes | Medium |
| PAS Biopsy | 1–2 days | ~87% | No | Medium |
🖼️ SLIDE 11 — ANTIFUNGAL TREATMENT OVERVIEW
- Clotrimazole, Miconazole (azoles) — tinea corporis, cruris, pedis, candidiasis
- Terbinafine cream — tinea pedis, corporis (allylamine)
- Ciclopirox nail lacquer — mild onychomycosis
- Nystatin cream/powder — cutaneous candidiasis
- Terbinafine (oral) — drug of choice for dermatophyte onychomycosis & tinea capitis
- Itraconazole — pulse therapy for onychomycosis; Candida; non-dermatophyte molds
- Fluconazole — candidiasis, tinea capitis (alternative)
- Griseofulvin — first-line tinea capitis in children (older, less used now)
| Site | Duration |
|---|---|
| Tinea corporis / cruris / pedis | 2–6 weeks |
| Tinea capitis | 6–8 weeks (systemic only) |
| Onychomycosis — fingernails | 6 weeks – 3 months |
| Onychomycosis — toenails | 3–6 months or longer |
| Cutaneous candidiasis | 2–4 weeks |
⚠️ Emerging resistance: T. indotineae (terbinafine-resistant) — increasing globally. Always confirm diagnosis before starting systemic therapy.

🖼️ SLIDE 12 — CONCLUSION
- Fungal diseases of skin and appendages range from superficial to subcutaneous, classified by depth of infection.
- Dermatophytes (Trichophyton, Microsporum, Epidermophyton) are the principal agents of tinea infections affecting skin, hair and nails.
- Candida albicans causes cutaneous candidiasis, paronychia, and oral thrush — especially in immunocompromised patients.
- KOH direct microscopy is the fastest, most accessible first-line laboratory test, demonstrating hyphae or pseudohyphae.
- Culture on SDA remains the gold standard — enables species identification and antifungal susceptibility testing.
- Molecular tools (PCR, ITS sequencing, MALDI-TOF) provide rapid, species-level diagnosis in complex or resistant cases.
- Wood lamp and dermoscopy are valuable non-invasive clinical adjuncts to guide sample collection.
- Treatment ranges from topical azoles/allylamines for limited disease to prolonged systemic antifungals for nail and scalp involvement.

🖼️ SLIDE 13 — REFERENCES
- Murray, P.R., Rosenthal, K.S., Pfaller, M.A. (2021). Medical Microbiology (9th ed.). Elsevier.
- Brooks, G.F., Carroll, K.C., Butel, J.S. et al. (2022). Jawetz, Melnick & Adelberg's Medical Microbiology (28th ed.). McGraw-Hill.
- Havlickova, B., Czaika, V.A., Friedrich, M. (2008). Epidemiological trends in skin mycoses worldwide. Mycoses, 51(Suppl 4): 2–15.
- Aly, R. (1994). Ecology and epidemiology of dermatophyte infections. J Am Acad Dermatol, 31(3): S21–S25.
- Ameen, M. (2010). Epidemiology of superficial fungal infections. Clin Dermatol, 28(2): 197–201.
- Nenoff, P. et al. (2014). Mycology — an update Part 1: Dermatomycoses. J Dtsch Dermatol Ges, 12(3): 188–210.
- Gupta, A.K., Cooper, E.A. (2008). Update in antifungal therapy of dermatophytosis. Mycopathologia, 166(5–6): 353–367.
- Rezusta, A. et al. (2011). MALDI-TOF MS identification of dermatophytes. Med Mycol, 50(5): 541–545.
📌 QUICK SUMMARY: Images per slide
| Slide | Image to paste |
|---|---|
| 1 — Title | Composite tinea a–i |
| 2 — TOC | Tinea capitis scalp lesion |
| 3 — Aim | Tinea capitis close-up |
| 4 — Overview | Composite tinea a–i |
| 5 — Tinea | Composite tinea a–i |
| 6 — Candida | CMC nails + oral thrush |
| 7 — Clinical Dx | Wood lamp fluorescence |
| 8 — KOH | Scraping procedure + KOH hyphae |
| 9 — Culture | SDA plate + LPCB microscopy |
| 10 — Molecular | KOH + GMS + dermoscopy panel |
| 11 — Treatment | Severe onychomycosis toe |
| 12 — Conclusion | Tinea capitis with alopecia |
| 13 — References | None |
reduce content it is too much per slide if i use 18pt font
SLIDE 1 — TITLE SLIDE
Clinical and Laboratory Diagnosis of Fungal Diseases Affecting the Skin and Its Appendages
Course: Medical Immunology Presented by: Zeel Kathiriya Group: 11 | Semester: 4 Instructor: Duyshenkulova Marina
SLIDE 2 — TABLE OF CONTENTS
- Aim & Objectives
- Overview & Classification
- Dermatophytosis — Tinea Infections
- Candidiasis of Skin & Nails
- Clinical Diagnosis Methods
- Laboratory Diagnosis — KOH Mount
- Laboratory Diagnosis — Culture
- Molecular & Serological Methods
- Antifungal Treatment
- Conclusion
- References
SLIDE 3 — AIM & OBJECTIVES
To understand the clinical features and laboratory methods for diagnosing fungal diseases of the skin and its appendages.
- Classify fungal diseases by affected structure
- Describe clinical presentations of tinea & candidiasis
- Explain KOH microscopy and culture methods
- Outline molecular diagnostic tools
- Summarise antifungal treatment principles
SLIDE 4 — OVERVIEW & CLASSIFICATION
- Affect outermost keratin only
- e.g. Pityriasis versicolor, Tinea nigra
- Invade skin, hair and nails
- Caused by dermatophytes (Trichophyton, Microsporum, Epidermophyton)
- Enter via trauma
- e.g. Sporotrichosis, Mycetoma
SLIDE 5 — DERMATOPHYTOSIS
- Trichophyton spp. — T. rubrum, T. tonsurans (most common)
- Microsporum spp. — M. canis (zoophilic)
- Epidermophyton floccosum — skin & nails only
| Type | Site | Feature |
|---|---|---|
| Tinea capitis | Scalp | Alopecia, scaling |
| Tinea corporis | Body | Annular plaque, central clearing |
| Tinea pedis | Feet | Maceration, itching |
| Tinea unguium | Nails | Dystrophy, discolouration |
| Tinea cruris | Groin | Erythematous patches |
SLIDE 6 — CANDIDIASIS
- Skin folds — erythema + satellite pustules
- Risk: diabetes, obesity, moisture
- Nail fold swelling, nail discolouration
- Chronic mucocutaneous candidiasis (CMC) in immunodeficiency
- White curd-like plaques on tongue/mucosa
- Common in infants & immunocompromised patients
SLIDE 7 — CLINICAL DIAGNOSIS METHODS
- Microsporum spp. → apple-green fluorescence of hair shafts
- Trichophyton → usually non-fluorescent
- Quick, non-invasive, bedside screening
- Comma/corkscrew hairs → tinea capitis
- Spiked pattern → onychomycosis
- Annular lesion + central clearing → tinea corporis
- Satellite pustules → candidiasis
- Nail dystrophy + debris → onychomycosis
SLIDE 8 — KOH DIRECT MICROSCOPY
- Add 10–20% KOH to specimen on slide
- Heat gently / wait 15–30 min
- Examine at 10× then 40×
| Organism | Finding |
|---|---|
| Dermatophytes | Septate branching hyphae |
| Candida | Pseudohyphae + budding yeast |
| Malassezia | Short hyphae + round spores ("spaghetti & meatballs") |
SLIDE 9 — CULTURE & IDENTIFICATION
- Acidic pH 5.6 — selective for fungi
- Incubate 25–28°C for 2–4 weeks
- Add cycloheximide + chloramphenicol to suppress contaminants
| Species | Colony appearance | Reverse pigment |
|---|---|---|
| T. rubrum | White, powdery | Red-wine |
| M. canis | Fluffy, yellow-white | Bright yellow |
| M. gypseum | Tan, granular | Golden-yellow |
- Microsporum — large spindle-shaped rough macroconidia
- Trichophyton — thin pencil-shaped macroconidia
- Candida — germ tube test (+) in serum = C. albicans
SLIDE 10 — MOLECULAR & SEROLOGICAL METHODS
- Gold standard for species identification
- Results in 24–48 h vs. 2–4 weeks for culture
- Detects mixed infections & resistant strains
- Rapid protein fingerprint from cultured colonies
- High accuracy for Candida & dermatophytes
- PAS stain → hyphae stain magenta/red
- GMS stain → fungal elements stain black
- Used when KOH and culture are negative
| Method | Speed | Sensitivity |
|---|---|---|
| KOH Mount | Minutes | ~75% |
| Culture | 2–4 weeks | ~85% |
| PCR/ITS | 24–48 h | ~95% |
| MALDI-TOF | Minutes | ~95% |
SLIDE 11 — ANTIFUNGAL TREATMENT
- Clotrimazole / Miconazole — tinea corporis, cruris, pedis
- Terbinafine cream — tinea pedis, corporis
- Nystatin — cutaneous candidiasis
- Ciclopirox lacquer — mild onychomycosis
- Terbinafine oral — onychomycosis, tinea capitis
- Itraconazole — Candida, non-dermatophyte molds
- Fluconazole — candidiasis, tinea capitis
- Griseofulvin — tinea capitis in children
- Skin (tinea) — 2–6 weeks
- Tinea capitis — 6–8 weeks
- Onychomycosis — 3–6 months
SLIDE 12 — CONCLUSION
- Fungal skin diseases range from superficial (keratin only) to subcutaneous (deep tissue).
- Dermatophytes cause tinea infections of skin, hair and nails; Candida causes candidiasis.
- KOH mount — fastest, cheapest first-line test; identifies hyphae/pseudohyphae.
- SDA culture — gold standard; enables species ID and susceptibility testing.
- Molecular methods (PCR, MALDI-TOF) give rapid species-level results.
- Wood lamp and dermoscopy are useful non-invasive clinical adjuncts.
- Treatment ranges from topical antifungals to prolonged systemic therapy depending on site and severity.
SLIDE 13 — REFERENCES
- Murray, Rosenthal, Pfaller. Medical Microbiology, 9th ed. Elsevier, 2021.
- Brooks et al. Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed. McGraw-Hill, 2022.
- Havlickova et al. Epidemiological trends in skin mycoses. Mycoses, 2008; 51(Suppl 4): 2–15.
- Aly R. Ecology and epidemiology of dermatophyte infections. J Am Acad Dermatol, 1994; 31(3): S21–S25.
- Ameen M. Epidemiology of superficial fungal infections. Clin Dermatol, 2010; 28(2): 197–201.
- Nenoff et al. Mycology — an update Part 1. J Dtsch Dermatol Ges, 2014; 12(3): 188–210.
- Gupta AK, Cooper EA. Antifungal therapy of dermatophytosis. Mycopathologia, 2008; 166: 353–367.
- Rezusta et al. MALDI-TOF MS for dermatophytes. Med Mycol, 2011; 50(5): 541–545.