Shoulder joint
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content and rich diagrams. Let me compile the full answer.
Shoulder Joint (Glenohumeral Joint)
Source: Gray's Anatomy for Students, THIEME Atlas of Anatomy
Type and Articulation
The glenohumeral joint is a synovial ball-and-socket (multiaxial) joint between:
- The large spherical head of the humerus
- The small, shallow glenoid cavity of the scapula
Both surfaces are covered by hyaline cartilage. It is the most mobile joint in the body, achieving this at the cost of skeletal stability - which is instead provided by muscles, tendons, and ligaments.
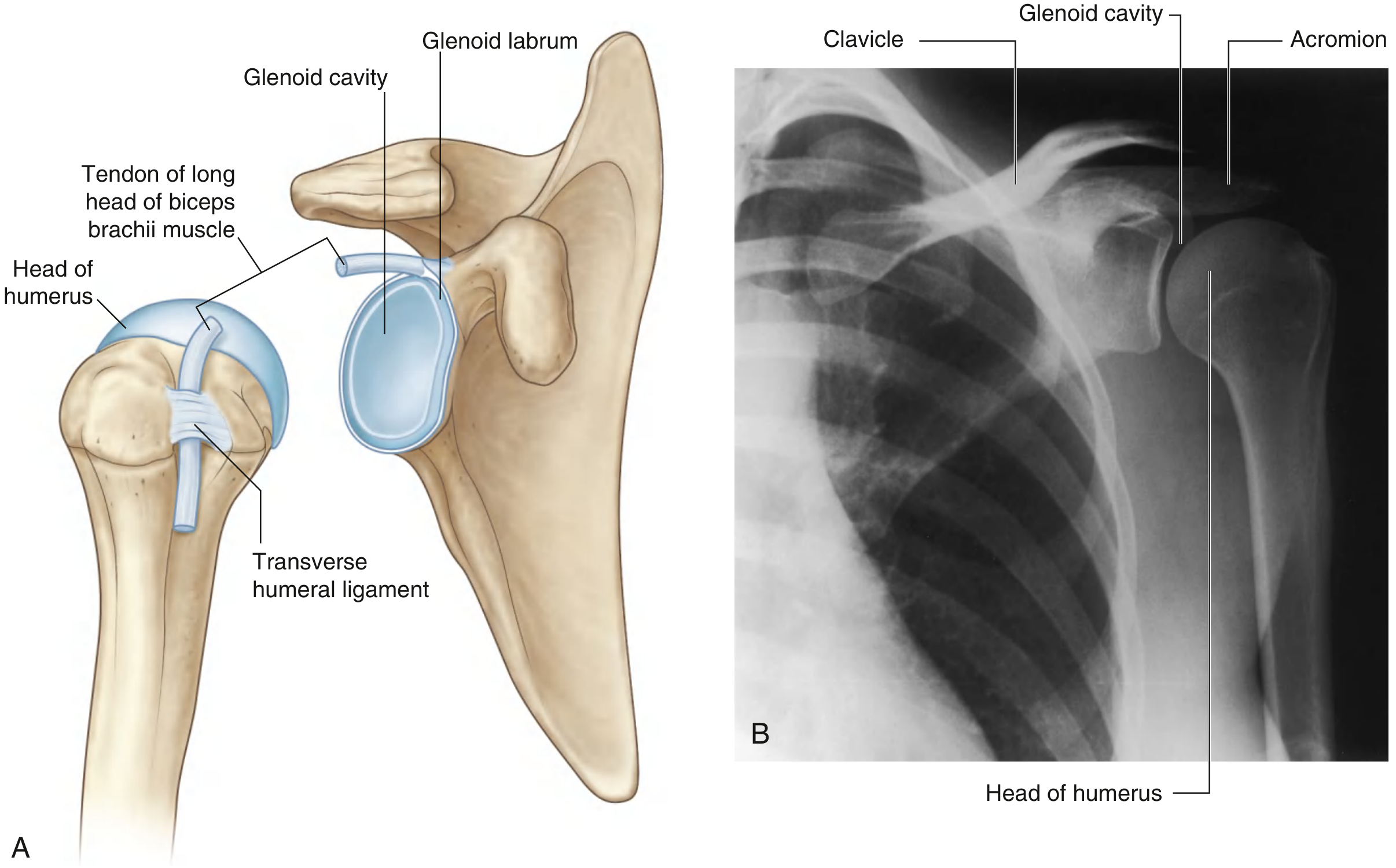
Fig. 7.25 - Articular surfaces of the right glenohumeral joint and its normal radiograph (Gray's Anatomy for Students)
Glenoid Labrum
The glenoid cavity is small relative to the humeral head. It is deepened and expanded peripherally by the glenoid labrum - a fibrocartilaginous rim attached to the margin of the fossa. Superiorly, the labrum is continuous with the tendon of the long head of biceps brachii, which attaches to the supraglenoid tubercle and passes through the articular cavity superior to the humeral head.
Joint Capsule
The fibrous membrane of the joint capsule attaches to:
- The margin of the glenoid cavity (outside the glenoid labrum)
- The anatomical neck of the humerus (extending inferiorly onto the shaft)
The capsule is loose inferiorly - this redundant region accommodates full abduction of the arm.
The capsule is thickened in three places to form ligaments:
Glenohumeral Ligaments (anterosuperior thickenings)
Three bands pass from the superomedial glenoid margin to the lesser tubercle and anatomical neck:
| Ligament | Position | Function |
|---|---|---|
| Superior glenohumeral ligament | Superior | Limits inferior translation |
| Middle glenohumeral ligament | Anterior | Limits lateral rotation & anterior translation |
| Inferior glenohumeral ligament | Inferior | Most important stabilizer - limits inferior & anterior translation |
Coracohumeral Ligament
A strong, broad band from the base of the coracoid process to the greater and lesser tubercles. It stabilizes the tendon of the long head of biceps as it passes through the intertubercular groove.
Transverse Humeral Ligament
Spans between the greater and lesser tubercles, holding the biceps tendon in the intertubercular (bicipital) groove.
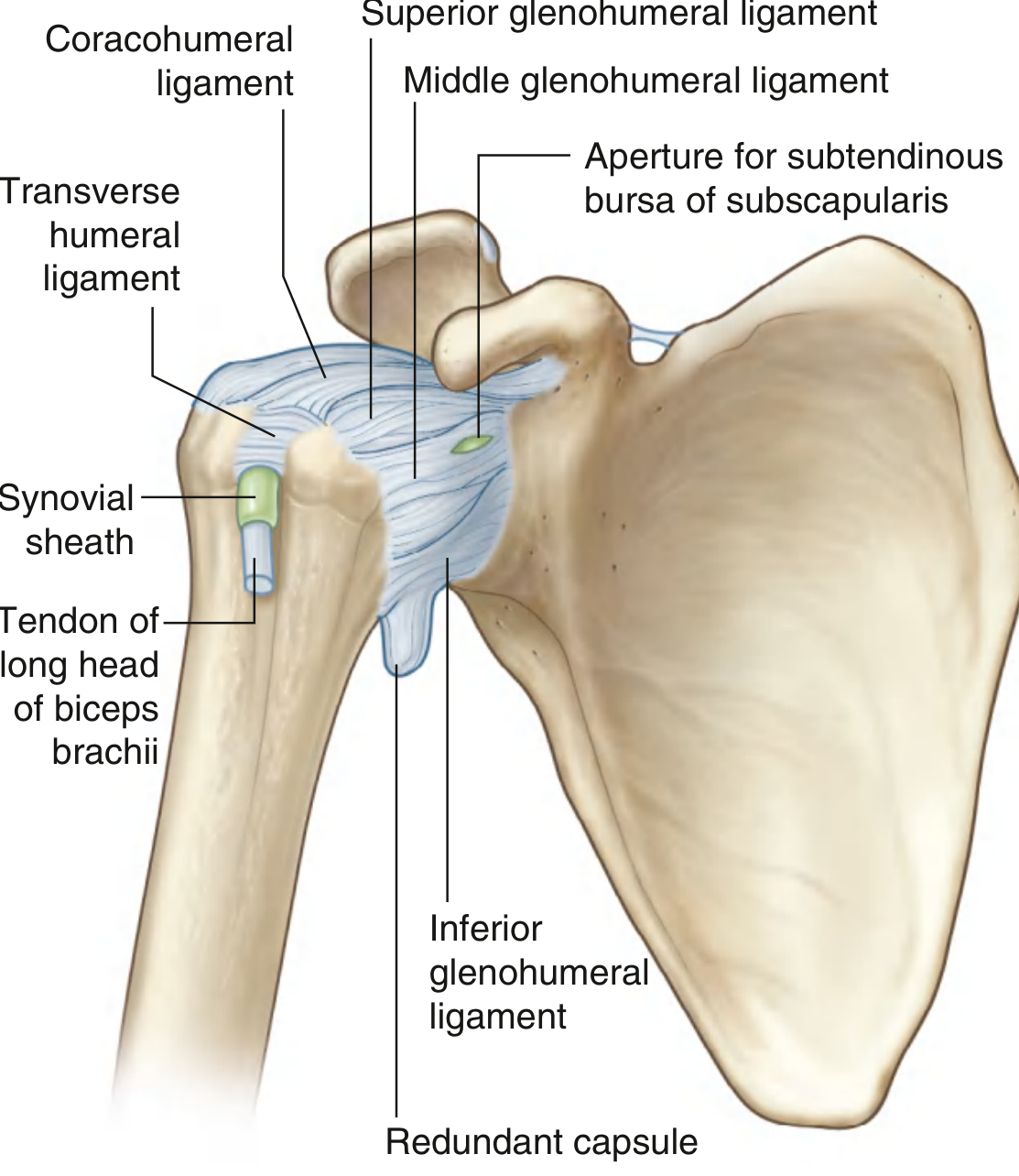
Fig. 7.27 - Capsule of the right glenohumeral joint (Gray's Anatomy for Students)
Synovial Membrane
The synovial membrane attaches to the margins of the articular surfaces and lines the fibrous capsule. It is loose inferiorly (redundant folds in adduction). It protrudes through apertures in the fibrous membrane to form bursae.
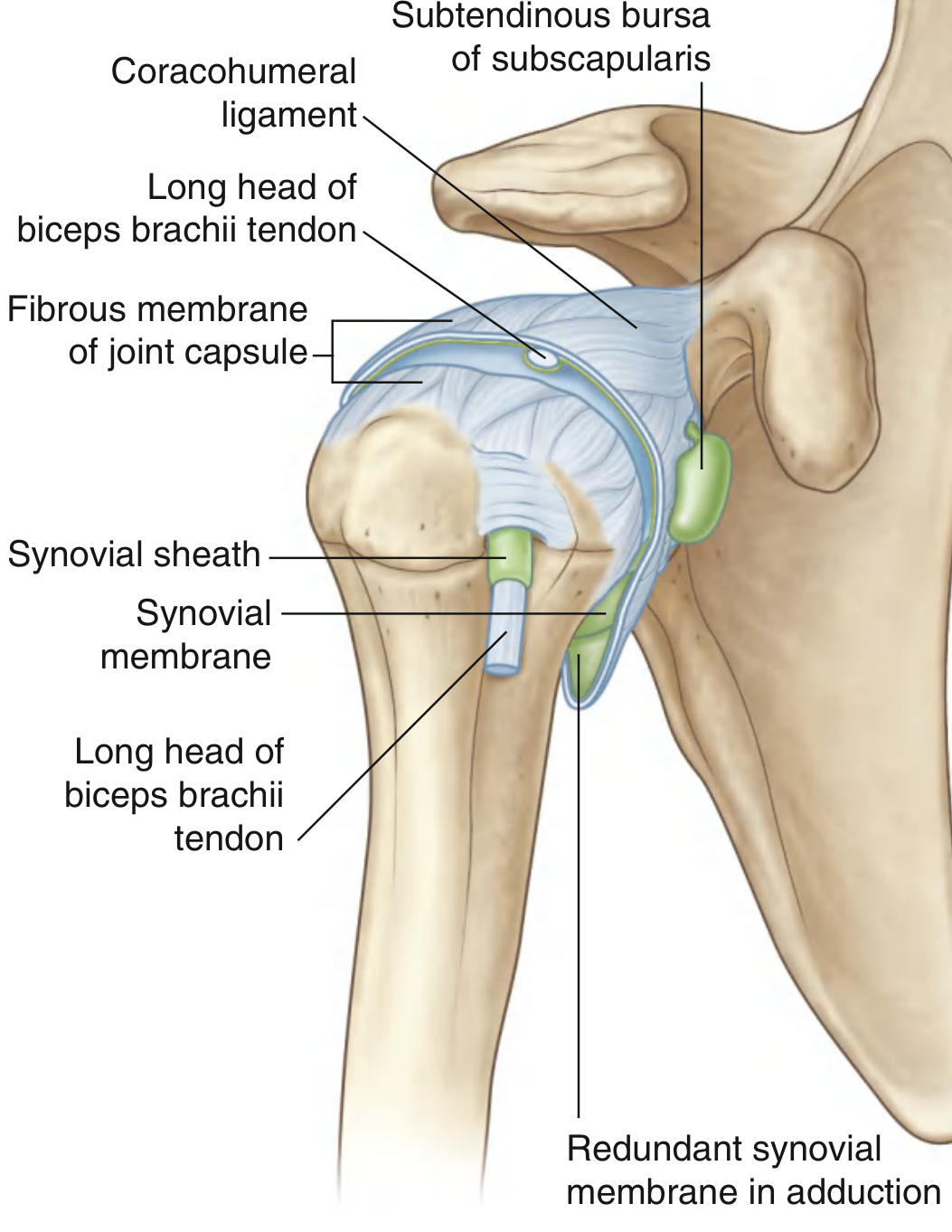
Fig. 7.26 - Synovial membrane and joint capsule (Gray's Anatomy for Students)
Bursae
Communicating with the joint cavity:
- Subtendinous bursa of subscapularis - between subscapularis tendon and fibrous membrane (most consistent; opens through the anterior capsule)
- Bicipital synovial sheath - the synovial membrane wraps the long head of biceps tendon as it descends into the intertubercular sulcus
Not communicating with the joint cavity:
- Subacromial (subdeltoid) bursa - between the acromion/deltoid and the supraspinatus/capsule (clinically very important; impingement occurs here)
- Bursa between the acromion and skin
- Bursa between the coracoid process and joint capsule
Stabilizers of the Joint
Rotator Cuff (SITS)
The tendons of the four rotator cuff muscles blend with and reinforce the joint capsule, forming a musculotendinous collar around the posterior, superior, and anterior aspects:
| Muscle | Position | Action at Glenohumeral Joint |
|---|---|---|
| Supraspinatus | Superior | Initiates abduction (first 15°); holds head in glenoid |
| Infraspinatus | Posterior | Lateral rotation |
| Teres minor | Posterior | Lateral rotation |
| Subscapularis | Anterior | Medial rotation |
The inferior aspect of the joint has no rotator cuff protection - this is the weakest part, explaining why most shoulder dislocations are inferior/anterior.
Long Head of Biceps Brachii
Passes through the joint superiorly; restricts upward migration of the humeral head.
Coracoacromial Arch
A bony arch formed by the coracoid process, acromion, and the coracoacromial ligament - creates a structural roof that prevents superior dislocation.
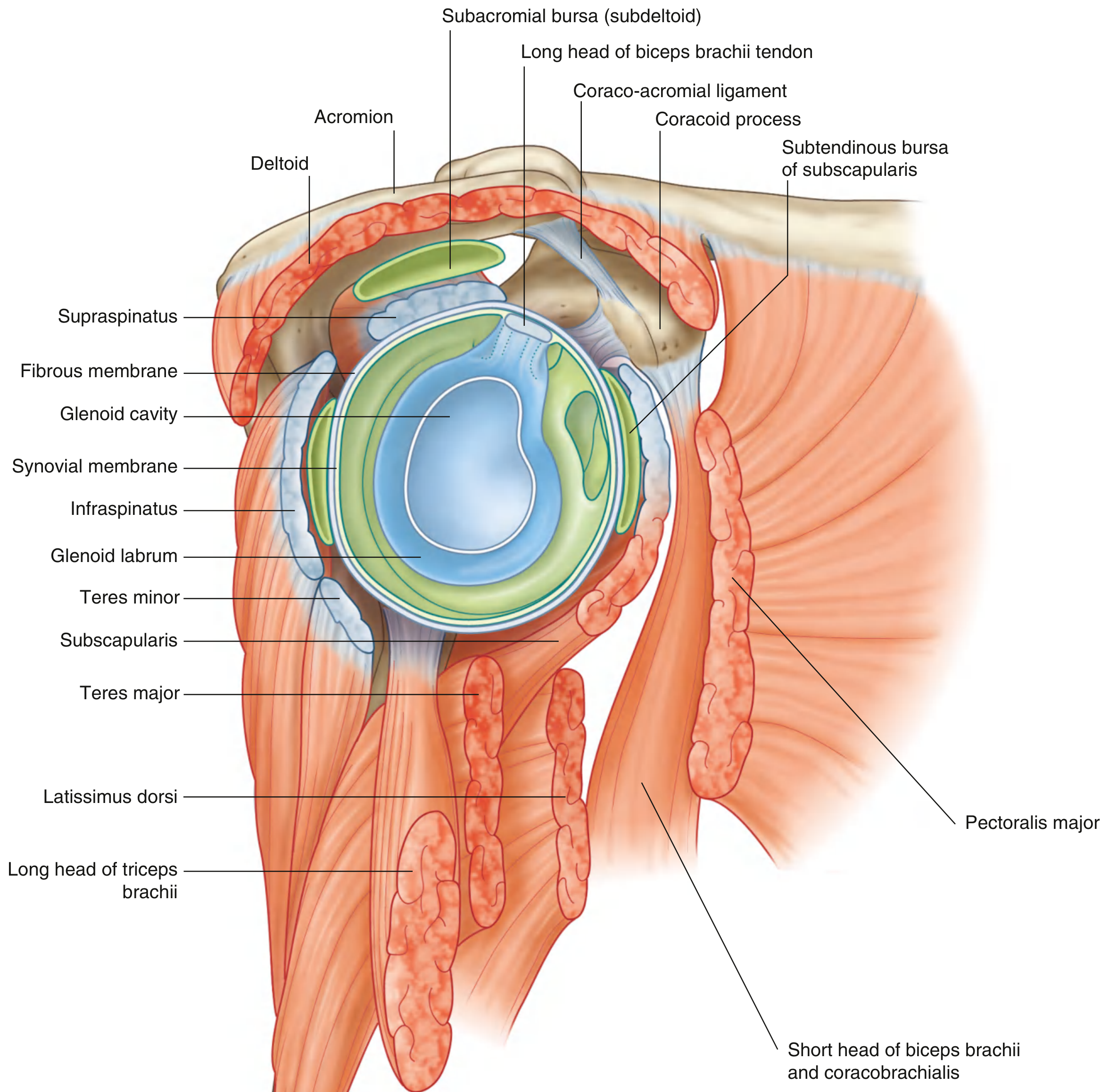
Fig. 7.28 - Lateral view of glenohumeral joint with surrounding muscles (Gray's Anatomy for Students)
Movements and Muscles
| Movement | Primary Muscles | Range |
|---|---|---|
| Flexion | Anterior deltoid, pectoralis major (clavicular head), coracobrachialis, biceps brachii | 0-180° |
| Extension | Posterior deltoid, teres major, latissimus dorsi | 0-60° |
| Abduction | Supraspinatus (0-15°), deltoid (15-90°), trapezius + serratus anterior for scapular rotation (90-180°) | 0-180° |
| Adduction | Pectoralis major, latissimus dorsi, teres major | 0-45° |
| Medial rotation | Subscapularis, pectoralis major, latissimus dorsi, teres major, anterior deltoid | 0-70° |
| Lateral rotation | Infraspinatus, teres minor, posterior deltoid | 0-90° |
| Circumduction | Combination of all above | Full arc |
Note: True full arm elevation to 180° requires ~120° at the glenohumeral joint + ~60° scapulothoracic rotation (scapulohumeral rhythm = 2:1 ratio).
Blood Supply
Predominantly from branches of:
- Anterior circumflex humeral artery
- Posterior circumflex humeral artery
- Suprascapular artery
Nerve Supply
The glenohumeral joint is innervated by branches from:
- Posterior cord of the brachial plexus
- Suprascapular nerve (C5, C6)
- Axillary nerve (C5, C6) - also supplies the deltoid and teres minor
- Lateral pectoral nerve (C5, C6, C7)
Clinical Points
| Condition | Key Anatomy |
|---|---|
| Anterior shoulder dislocation (most common ~95%) | Humeral head dislocates anteroinferiorly through the weak inferior capsule; axillary nerve at risk |
| Rotator cuff tear | Usually supraspinatus; impingement under coracoacromial arch in subacromial space |
| Frozen shoulder (adhesive capsulitis) | Fibrosis and contracture of the inferior redundant capsular folds |
| SLAP lesion | Superior labrum tear involving the biceps anchor (supraglenoid tubercle attachment) |
| Bankart lesion | Avulsion of the anteroinferior glenoid labrum - seen in recurrent anterior dislocations |
| Hill-Sachs lesion | Compression fracture of the posterolateral humeral head from anterior dislocation |
Gray's Anatomy for Students, pp. 826-829 | THIEME Atlas of General Anatomy and Musculoskeletal System
Laq 15 mark on shoulder joint
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have all the material needed for a complete 15-mark long answer. Let me compile it.
SHOULDER JOINT (GLENOHUMERAL JOINT)
Long Answer Question — 15 Marks
I. INTRODUCTION
The shoulder (glenohumeral) joint is the most mobile joint in the human body. It is a multiaxial ball-and-socket synovial joint formed between the large spherical head of the humerus and the small, shallow glenoid cavity of the scapula. This wide range of mobility is achieved at the cost of bony stability, which is instead provided by muscles, tendons, and ligaments.
II. TYPE OF JOINT
| Feature | Detail |
|---|---|
| Type | Synovial, ball-and-socket (spheroidal) |
| Variety | Multiaxial |
| Articular surfaces | Head of humerus + glenoid cavity of scapula |
| Cartilage | Hyaline cartilage on both surfaces |
III. ARTICULAR SURFACES
Fig. 1 - Glenohumeral joint articular surfaces and radiograph (Gray's Anatomy for Students, p. 826)
- Head of humerus - large, rounded, faces medially, upward, and backward; covered with hyaline cartilage.
- Glenoid cavity of scapula - small, pear-shaped, faces laterally and slightly forward; much smaller than the humeral head (occupies only ~1/4 of its area).
Glenoid Labrum
- A fibrocartilaginous rim attached to the periphery of the glenoid cavity.
- Deepens and expands the cavity, improving congruence.
- Superiorly, it is continuous with the tendon of the long head of biceps brachii, which attaches to the supraglenoid tubercle and passes through the articular cavity superior to the humeral head.
IV. JOINT CAPSULE
The fibrous membrane of the capsule:
- Attaches medially: to the margin of the glenoid cavity, outside the glenoid labrum
- Attaches laterally: to the anatomical neck of humerus (medially extends further down onto the shaft)
- Is loose and redundant inferiorly - this fold accommodates full abduction of the arm
- Has openings that allow communication with bursae
Synovial Membrane
- Lines the entire fibrous capsule
- Is loose inferiorly (accommodates abduction)
- Protrudes through capsule openings to form bursae
- Wraps the long head of biceps tendon as it descends through the joint into the intertubercular sulcus (forming a synovial sheath)
Fig. 2 - Synovial membrane and joint capsule of right glenohumeral joint (Gray's Anatomy for Students, p. 826)
V. LIGAMENTS
Fig. 3 - Capsule of right glenohumeral joint showing all ligaments (Gray's Anatomy for Students, p. 827)
A. Glenohumeral Ligaments (3 bands - anterosuperior thickenings of capsule)
These pass from the superomedial glenoid margin to the lesser tubercle and anatomical neck of humerus:
| Ligament | Position | Function |
|---|---|---|
| Superior glenohumeral ligament | Superior | Limits inferior translation; taut in adduction |
| Middle glenohumeral ligament | Anterior | Limits anterior translation & lateral rotation (30-60° abduction) |
| Inferior glenohumeral ligament | Inferior | Most important stabilizer; limits anterior/inferior translation (>60° abduction) |
B. Coracohumeral Ligament
- Strong, broad band from the base of the coracoid process to the greater and lesser tubercles
- Reinforces the capsule superiorly
- Stabilizes the tendon of the long head of biceps as it enters the intertubercular groove
C. Transverse Humeral Ligament
- Bridges the greater and lesser tubercles
- Retains the tendon of long head of biceps in the intertubercular (bicipital) sulcus
D. Coracoacromial Ligament (not part of capsule)
- Connects the coracoid process to the acromion
- Forms the coracoacromial arch - prevents superior dislocation of the humeral head
VI. BURSAE
Communicating with joint cavity:
- Subtendinous bursa of subscapularis - between the subscapularis tendon and the fibrous capsule (opens through an anterior aperture); most constant
- Bicipital synovial sheath - surrounds the biceps tendon in the intertubercular sulcus
Non-communicating bursae:
- Subacromial (subdeltoid) bursa - between acromion/deltoid and supraspinatus/capsule; clinically very important (site of impingement syndrome)
- Subcoracoid bursa - between coracoid process and joint capsule
- Subscapular bursa - between skin and acromion
VII. STABILITY OF THE JOINT
The joint relies on dynamic and static stabilizers rather than bony congruence:
Static Stabilizers
- Glenoid labrum (deepens socket)
- Glenohumeral ligaments
- Negative intra-articular pressure
- Coracoacromial arch (prevents superior displacement)
Dynamic Stabilizers - The ROTATOR CUFF (SITS)
Fig. 4 - Lateral view of glenohumeral joint with rotator cuff and surrounding muscles (Gray's Anatomy for Students, p. 828)
The tendons of four rotator cuff muscles blend with the joint capsule and form a musculotendinous collar around the posterior, superior, and anterior aspects:
| Muscle | Position | Action | Nerve |
|---|---|---|---|
| Supraspinatus | Superior | Initiates abduction (0-15°); compresses head into glenoid | Suprascapular (C5, C6) |
| Infraspinatus | Posterior | Lateral rotation | Suprascapular (C5, C6) |
| Teres minor | Posteroinferior | Lateral rotation | Axillary (C5, C6) |
| Subscapularis | Anterior | Medial rotation | Upper & lower subscapular (C5, C6) |
Weak point: The inferior aspect of the joint has NO rotator cuff coverage - this is why most dislocations are anteroinferior.
Long Head of Biceps Brachii
- Passes superiorly through the joint
- Restricts upward migration of the humeral head
VIII. MOVEMENTS AND MUSCLES
| Movement | Prime Movers | Range |
|---|---|---|
| Flexion | Anterior deltoid, pectoralis major (clavicular), biceps brachii, coracobrachialis | 0-180° |
| Extension | Posterior deltoid, teres major, latissimus dorsi | 0-60° |
| Abduction | Supraspinatus (0-15°), deltoid (15-90°) + scapular rotation (90-180°) | 0-180° |
| Adduction | Pectoralis major, latissimus dorsi, teres major | 0-45° |
| Medial rotation | Subscapularis, pectoralis major, latissimus dorsi, teres major, anterior deltoid | 0-70° |
| Lateral rotation | Infraspinatus, teres minor, posterior deltoid | 0-90° |
| Circumduction | All above in sequence | Full arc |
Scapulohumeral rhythm: Full arm elevation to 180° = 120° glenohumeral + 60° scapulothoracic rotation (2:1 ratio).
IX. BLOOD SUPPLY
- Anterior circumflex humeral artery (branch of axillary artery)
- Posterior circumflex humeral artery (passes through quadrangular space with axillary nerve)
- Suprascapular artery (branch of thyrocervical trunk)
X. NERVE SUPPLY
(Hilton's Law: joint supplied by same nerves that supply muscles acting on it)
- Suprascapular nerve (C5, C6) - front and back
- Axillary nerve (C5, C6) - anterior and inferior capsule
- Lateral pectoral nerve (C5, C6, C7)
- Branches from posterior cord of brachial plexus
XI. APPLIED ANATOMY / CLINICAL SIGNIFICANCE
1. Dislocation of the Shoulder
Fig. 5 - Anterior (subcoracoid) dislocation of the shoulder (Pye's Surgical Handicraft)
Anterior dislocation (~95% of all dislocations)
- Most common - head displaces anteroinferiorly, coming to rest below the coracoid process (subcoracoid dislocation)
- Mechanism: forced abduction + external rotation
- Features: flattening of deltoid contour, arm held in slight abduction against the chest, loss of normal rounded shoulder contour
- Axillary nerve is at risk - check sensation over the "regimental badge" area (lateral deltoid)
- Complications: Bankart lesion (avulsion of anteroinferior labrum), Hill-Sachs lesion (compression fracture of posterolateral humeral head)
Posterior dislocation (~5%)
- Less common; arm held in internal rotation
- Often missed on AP radiograph ("light bulb sign")
- Associated with seizures and electrocution
Inferior dislocation (Luxatio Erecta - rarest)
- Arm held elevated/abducted above head
2. Rotator Cuff Tear
- Supraspinatus is most commonly torn (at its "critical zone" near the greater tubercle)
- Caused by impingement under the coracoacromial arch within the subacromial space
- Presents with painful arc (60°-120° of abduction)
3. Adhesive Capsulitis (Frozen Shoulder)
- Fibrosis and contracture of the inferior redundant capsular folds
- Progressive painful restriction of all movements, especially external rotation
4. SLAP Lesion
- Superior Labrum from Anterior to Posterior tear
- Involves the biceps tendon anchor at the supraglenoid tubercle
5. Subacromial Impingement Syndrome
- Compression of supraspinatus tendon and subacromial bursa between the humeral head and coracoacromial arch
- Painful arc at 60°-120° of abduction
SUMMARY DIAGRAM
| Structural Feature | Detail |
|---|---|
| Type | Synovial, ball-and-socket, multiaxial |
| Articular surfaces | Head of humerus + glenoid cavity |
| Labrum | Fibrocartilaginous rim deepening glenoid |
| Capsule attachment | Glenoid margin to anatomical neck of humerus |
| Ligaments | Superior/Middle/Inferior glenohumeral, Coracohumeral, Transverse humeral |
| Communicating bursae | Subscapularis subtendinous bursa, Bicipital sheath |
| Non-communicating bursae | Subacromial/subdeltoid, Subcoracoid |
| Rotator cuff (SITS) | Supraspinatus, Infraspinatus, Teres minor, Subscapularis |
| Blood supply | Anterior/Posterior circumflex humeral, Suprascapular arteries |
| Nerve supply | Suprascapular, Axillary, Lateral pectoral, Posterior cord |
| Weakest point | Inferior - no rotator cuff cover (site of most dislocations) |
Sources: Gray's Anatomy for Students, pp. 826-829 | THIEME Atlas of General Anatomy and Musculoskeletal System | Pye's Surgical Handicraft, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.