Hernia in detail with images and EhS classification
Reading File
Finding Sources
Searching the Web
EHS classification hernia European Hernia Society grading system
Reading File
Reading File
Reading Web Page
https://jhs.gr.jp/pdf/EHS_groin_hernia_classification.pdf
Searching Images
hernia types anatomy inguinal femoral umbilical classification diagram
Finding Sources
Reading File
Loading Image
Searching Images
EHS classification groin hernia lateral medial femoral grid table
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC2719726/
I now have comprehensive material to write a detailed, well-illustrated answer. Let me compile it:
Hernia: Comprehensive Overview with EHS Classification
Definition
A hernia is the protrusion of a viscus, or part of a viscus, through a normal or abnormal aperture in the walls of its containing cavity. The essential components are:
- Covering (hernial sac): derived from peritoneum
- Contents: bowel, omentum, or other abdominal organs
- Defect: the fascial/muscular aperture through which protrusion occurs
Anatomical Classification
Groin (Inguinal Region) Hernias
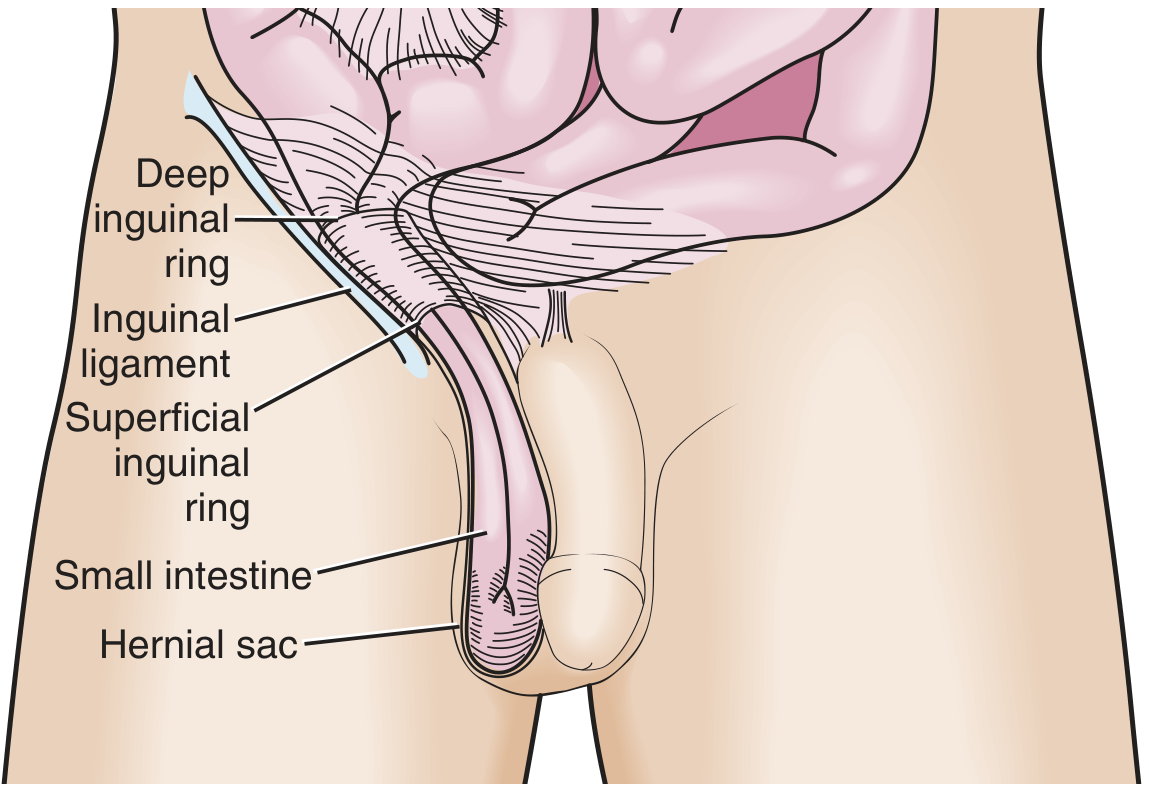
Indirect inguinal hernia — the most common type (65% of all groin hernias). The sac passes through the deep inguinal ring, travels lateral to the inferior epigastric vessels, through the inguinal canal, and may descend into the scrotum. It follows the path of the processus vaginalis and is often congenital in origin.
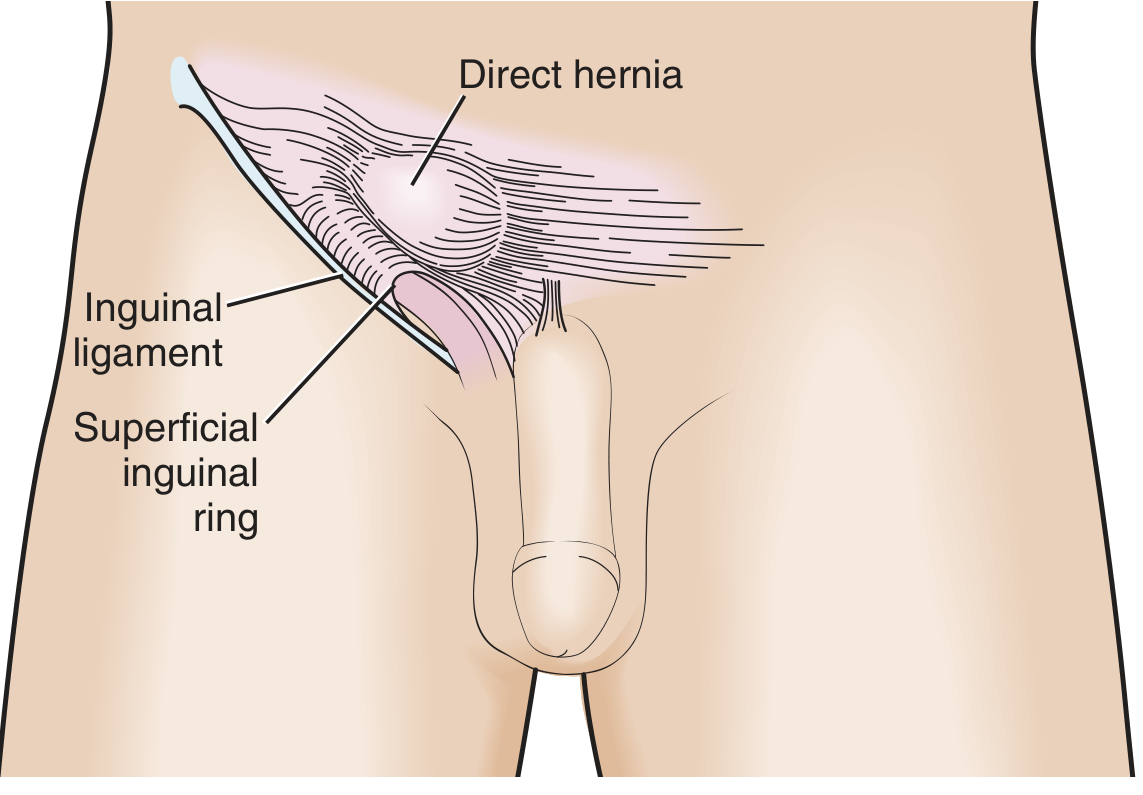
Direct inguinal hernia — the sac pushes through the posterior wall of the inguinal canal (Hesselbach's triangle), medial to the inferior epigastric vessels. It is an acquired weakness, related to aging, obesity, and connective tissue disorders.
Femoral hernia — protrudes through the femoral canal, inferior to the inguinal ligament, medial to the femoral vein and lateral to the lacunar ligament. More common in women. Up to 45% are incarcerated at presentation due to the narrow, rigid femoral ring.
The anatomical relationships of all three groin hernias relative to the inferior epigastric vessels and femoral sheath:
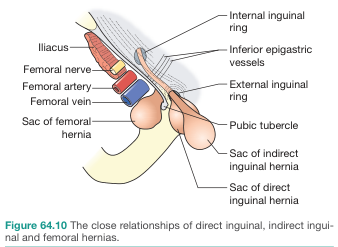
Pantaloon hernia — a combination of direct and indirect components straddling the inferior epigastric vessels, resembling trouser legs.
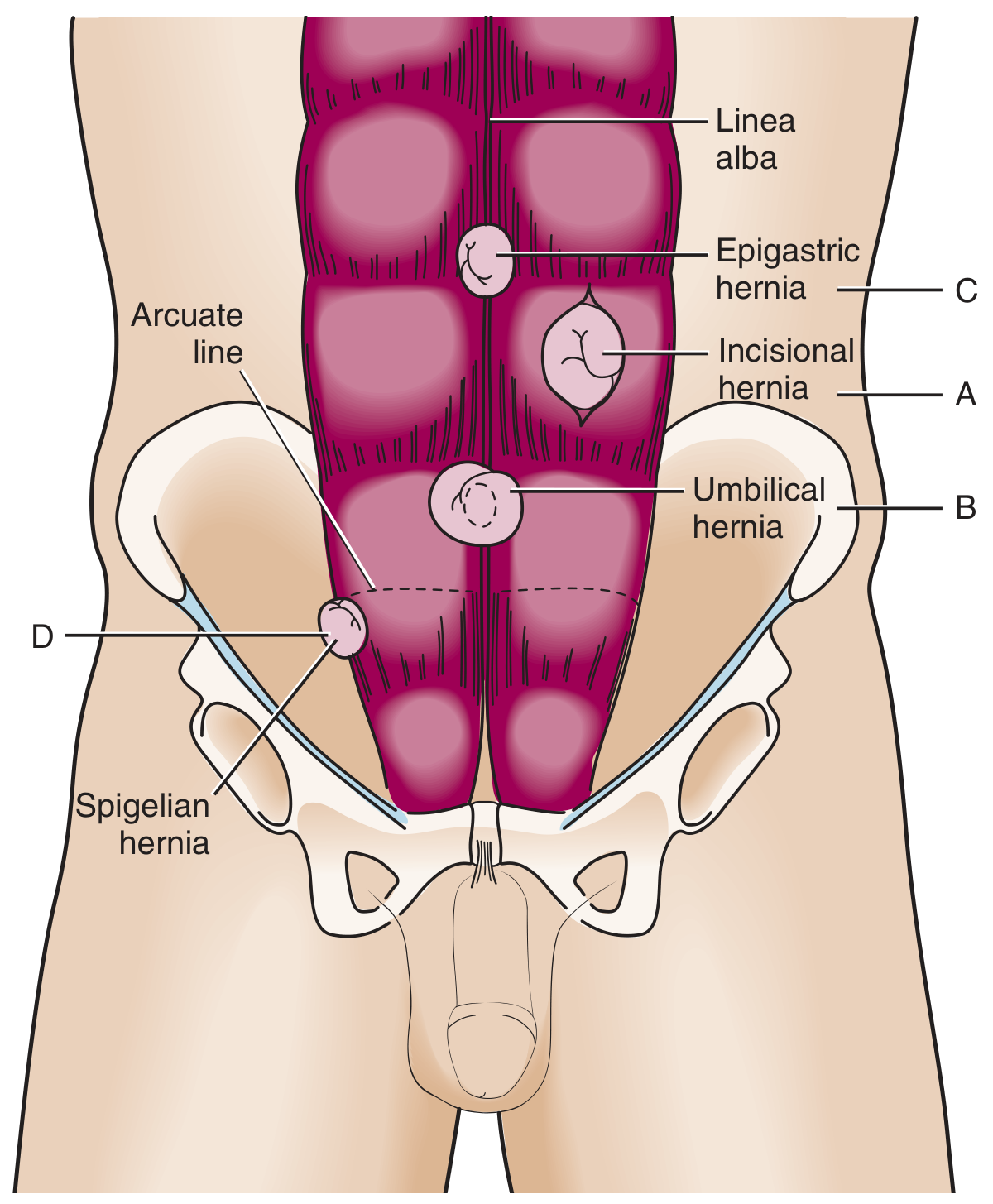
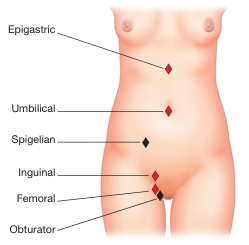
Ventral (Anterior Abdominal Wall) Hernias
The major ventral hernias with their anatomical sites:
| Type | Location | Key Features |
|---|---|---|
| Incisional | Any prior surgical scar | Occurs in ~20% post-laparotomy; 20–50% recurrence rate; incarceration risk low |
| Umbilical | Umbilical fibromuscular ring | Common in infants (congenital), resolves by age 5; adult form prone to strangulation |
| Epigastric | Linea alba, xiphoid–umbilicus | Usually small, contains preperitoneal fat; also seen in ~4% of pediatric hernias |
| Spigelian | Lateral rectus edge at arcuate line | Rare; interstitial position → high incarceration rate (~20%); US/CT often needed |
| Parastomal | Around stoma site | Incisional variant with specific repair challenges |
External Surface of Abdomen — Hernia Sites Overview
Diaphragmatic Hernias
There are three main types:
- Sliding (Type I) hiatal hernia — gastro-oesophageal junction migrates above the diaphragm; most common (>95% of hiatal hernias)
- Rolling/Paraesophageal hernia — gastric fundus herniates alongside the oesophagus; GEJ remains below diaphragm
- Congenital (Bochdalek/Morgagni) — usually left-sided; presents at birth with respiratory failure
Internal Hernias
These occur through normal or abnormal peritoneal/mesenteric apertures without external bulge:
- Paraduodenal — most common congenital internal hernia
- Foramen of Winslow hernia — bowel enters the lesser sac
- Iatrogenic — after Roux-en-Y gastric bypass, colectomy, pancreaticoduodenectomy (mesocolon or mesentery division)
- Obturator / sciatic notch hernias — uncommon but important causes of obscure SBO
Pathological States
| State | Definition | Surgical urgency |
|---|---|---|
| Reducible | Contents return to abdomen spontaneously or manually | Elective |
| Irreducible / Incarcerated | Contents cannot be returned; no vascular compromise | Urgent |
| Obstructed | Incarcerated bowel with luminal obstruction | Urgent / emergency |
| Strangulated | Ischemia of hernial contents from compression at neck | Emergency |
| Richter hernia | Only part of bowel wall in the sac → partial obstruction possible without complete obstruction | Emergency |
CT of a groin hernia (axial and coronal views showing the herniating segment and hernia orifice):
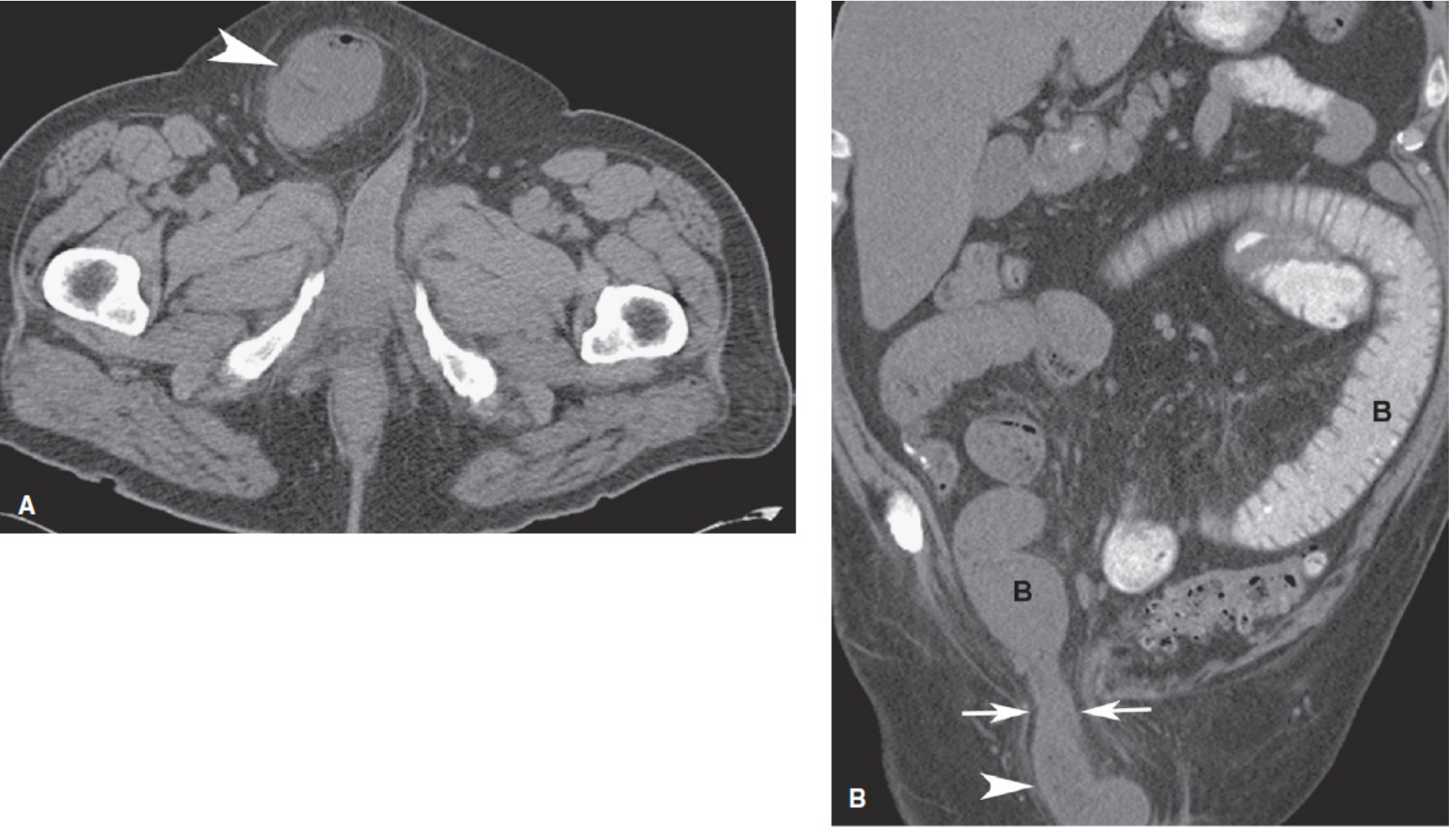
Strangulation risk is highest with femoral hernias (~40–45%), intermediate with umbilical hernias (up to 60% show strangulation at surgery), and lowest with incisional hernias (~2%). — Sleisenger & Fordtran's Gastrointestinal and Liver Disease
EHS (European Hernia Society) Classification
The EHS has published distinct classification systems for three hernia categories. These are used to standardise operative reporting, tailor repair techniques, and enable registry-based comparison of outcomes.
1. EHS Groin Hernia Classification (2007)
Published by Miserez et al. based on the Aachen (Schumpelick) classification, this is a simple intraoperative grid system.
The two axes are:
- Type: L = Lateral (indirect), M = Medial (direct), F = Femoral, X = No hernia
- Size: 1 = small (≤1.5 cm / one finger), 2 = medium (1.5–3 cm / two fingers), 3 = large (>3 cm / more than two fingers)
EHS Groin Hernia Grid:
| Right | Left | |
|---|---|---|
| L (Lateral/Indirect) | L0 · L1 · L2 · L3 | L0 · L1 · L2 · L3 |
| M (Medial/Direct) | M0 · M1 · M2 · M3 | M0 · M1 · M2 · M3 |
| F (Femoral) | F0 · F1 · F2 · F3 | F0 · F1 · F2 · F3 |
- Suffix 0 = no hernia present at that site
- Suffixes 1–3 = size categories above
- P is added for recurrent/previous repair (e.g., L2P)
Clinical significance of subgroups:
- L1: Small indirect — posterior wall intact; suture repair may suffice in select cases
- M3: Large direct — EHS guidelines strongly recommend mesh fixation in laparoscopic (TAPP/TEP) repair to reduce recurrence
- F1–F3: All femoral hernias require urgent repair due to high strangulation risk
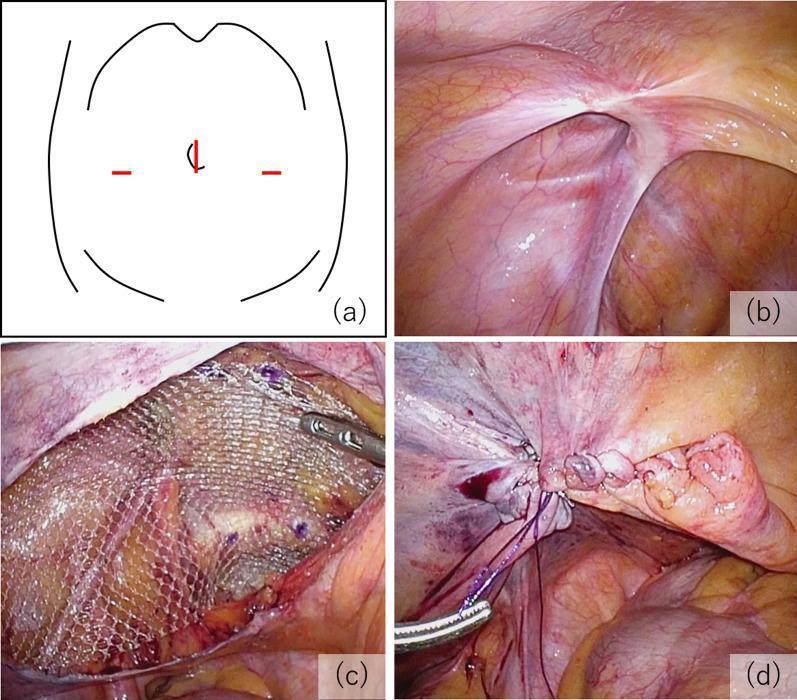
Laparoscopic (TAPP) view of an EHS L2 hernia with mesh placement and peritoneal closure:
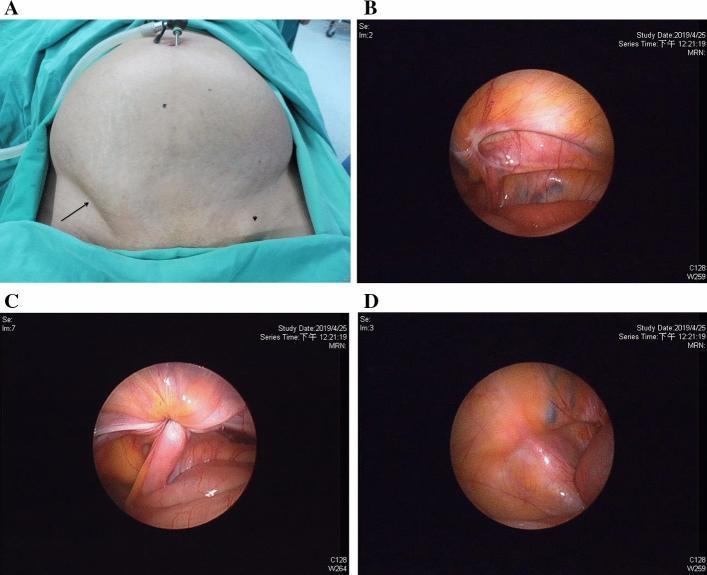
Clinical + laparoscopic findings including EHS L3 indirect and EHS F1 femoral hernia in the same patient:
2. EHS Primary Abdominal Wall Hernia Classification (2009)
Proposed by Muysoms et al. for epigastric, umbilical, Spigelian, and lumbar hernias (excluding incisional and parastomal).
Two variables:
| Variable | Categories |
|---|---|
| Localisation | Epigastric / Umbilical / Spigelian / Lumbar |
| Size (diameter) | Small (<2 cm) / Medium (2–4 cm) / Large (>4 cm) |
Parastomal hernias are deliberately excluded as a distinct group with separate classification.
3. EHS Incisional Hernia Classification (2009)
For postoperative (incisional) hernias, two variables are used. A full grid format was not achieved due to lack of consensus on a single size variable.
Localisation — based on grid coordinates of the abdominal wall:
| Midline | Lateral | |
|---|---|---|
| Subxiphoidal (M1) | Above xiphoid | L1 = subcostal |
| Epigastric (M2) | Xiphoid–umbilicus | L2 = flank |
| Umbilical (M3) | At umbilicus | L3 = iliac |
| Infraumbilical (M4) | Umbilicus–pubis | L4 = lumbar |
| Suprapubic (M5) | Below M4 |
Size — width of defect (most critical variable for repair difficulty):
- W1: < 4 cm
- W2: ≥ 4 cm and < 10 cm
- W3: ≥ 10 cm
Additional recorded variables: R (recurrent, yes/no) and number of previous repairs.
4. EHS Parastomal Hernia Classification (2012)
Defined at a consensus meeting in Toruń, Poland (April 2012):
- Type I: Small (<5 cm), no bowel herniation
- Type II: Small (<5 cm), bowel herniation present
- Type III: Large (≥5 cm), no bowel herniation
- Type IV: Large (≥5 cm), bowel herniation present
Aetiology & Risk Factors
Congenital: Patent processus vaginalis → indirect inguinal hernia; congenital diaphragmatic (Bochdalek) hernia; umbilical hernia of infancy
Acquired — predisposing factors:
- Raised intra-abdominal pressure: chronic cough (COPD), straining (constipation, BPH), obesity, ascites, pregnancy
- Connective tissue weakness: aging, Ehlers-Danlos, Marfan syndrome, collagen metabolism disorders
- Prior surgery: disruption of fascial integrity → incisional hernia (~20% post-laparotomy)
- Nutritional/metabolic: malnutrition, steroid use, wound infection post-surgery
Clinical Features & Diagnosis
Symptoms:
- Reducible swelling aggravated by coughing, standing, straining; relieved by lying down
- Pain or dragging discomfort at the hernia site
- Signs of obstruction (nausea, vomiting, absolute constipation) if incarcerated
Physical examination:
- Inguinal canal examined with inverted scrotal skin in males; Valsalva maneuver increases pressure
- Indirect vs. direct differentiation:
- Indirect: starts lateral to inferior epigastric artery, tip of finger hit during cough, fills scrotum, controlled by pressure over deep ring
- Direct: pushes against finger pad, medial protrusion, not controlled by deep ring pressure
- Femoral: bulge appears below and lateral to pubic tubercle (vs. inguinal = above pubic tubercle)
Imaging:
- CT scan: gold standard for internal hernias, incarcerated/obstructed hernias, and obese patients where palpation is unreliable
- Ultrasound: useful for Spigelian hernias and equivocal groin swellings
- Dynamic MRI: considered if ultrasound is negative or non-diagnostic for occult groin hernias
Management
Conservative
Watchful waiting is acceptable for asymptomatic or minimally symptomatic hernias (especially inguinal hernias in elderly/unfit patients). Trusses are rarely used today and do not prevent incarceration.
Surgical Repair
Open techniques:
- Lichtenstein (tension-free mesh repair) — gold standard for inguinal hernia; mesh laid on posterior inguinal canal wall
- Bassini / Shouldice — tissue repairs (without mesh); reserved for contaminated fields
- McVay (Cooper's ligament repair) — used for femoral hernia repair
- Mayo repair — for umbilical hernia
Laparoscopic / Endoscopic techniques:
- TAPP (TransAbdominal PrePeritoneal) — mesh placed preperitoneally via transabdominal approach; peritoneum closed over mesh
- TEP (Totally ExtraPeritoneal) — mesh placed without entering peritoneum
- Benefits: bilateral repair, early return to activity, less chronic pain; mesh fixation recommended for M3 (large direct) defects
Emergency repair (incarcerated/strangulated):
- Urgent resuscitation, antibiotics, then surgery
- Open tissue repair preferred over mesh in contaminated fields; laparoscopy useful for reduction and viability assessment
- Richter hernias may present without complete obstruction — careful vigilance required since partial strangulation occurs silently
Key Comparisons Summary
| Feature | Indirect Inguinal | Direct Inguinal | Femoral |
|---|---|---|---|
| Path | Through deep ring | Hesselbach's triangle | Femoral canal |
| Relation to epigastric vessels | Lateral | Medial | Below inguinal ligament |
| Sex | M >> F | M >> F | F > M |
| Congenital | Yes (processus vaginalis) | No | No |
| Incarceration risk | Low–Moderate | Low | Very high (40–45%) |
| EHS code | L1–L3 | M1–M3 | F1–F3 |
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine; Mulholland & Greenfield's Surgery (7e); Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Bailey & Love's Short Practice of Surgery (28e); Miserez et al. Hernia 2007 (EHS groin classification); Muysoms et al. Hernia 2009 (EHS primary/incisional classification); EHS/AHS guidelines 2018.
This is a shared conversation. Sign in to Orris to start your own chat.