Give answer on Silicosis for md exams 10 marks
From fishman and murray only
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content I need from both Fishman's and Murray & Nadel's. Let me compile a comprehensive 10-mark MD exam answer.
SILICOSIS
[10 Marks - MD Examination Answer]
Sources: Fishman's Pulmonary Diseases and Disorders (5th ed.) & Murray & Nadel's Textbook of Respiratory Medicine
DEFINITION
Silicosis is a fibrosing lung disease caused by the inhalation, retention, and pulmonary reaction to crystalline silica (silicon dioxide, SiO2), most commonly in the form of quartz, and less commonly as cristobalite and tridymite - collectively called "free silica" to distinguish them from silicates. Amorphous silica is relatively non-toxic. Silica content in different rock formations (sandstone, granite, slate) varies from 20% to nearly 100%.
(Fishman's Pulmonary Diseases and Disorders, p. 1551; Murray & Nadel's, p. 2344)
OCCUPATIONS AND INDUSTRIES AT RISK
Silicosis is the oldest known occupational lung disease (alluded to by Hippocrates and Pliny). Respirable particles of 0.5-5.0 μm aerodynamic diameter are the most hazardous. At-risk groups include:
| High-risk Industries | High-risk Occupations |
|---|---|
| Metal mining | Sandblasters / abrasive blasters |
| Quarrying, drilling, tunneling | Stone masons, stone carvers |
| Iron and steel foundries | Pottery workers |
| Construction / road demolition | Dental technicians |
| Engineered stone fabrication | Jewelers (chalk molds) |
| Ceramic / pottery manufacturing | Roof bolters |
New and emerging risk groups include workers fabricating artificial/engineered stone countertops (a severe silicosis risk with accelerated disease) and workers producing stressed denim by sandblasting.
(Fishman's p. 1551-1552; Murray & Nadel's p. 2344)
PATHOGENESIS
Dust particles of respirable size deposit in the alveoli and are engulfed by alveolar macrophages. The balance between dust deposition and clearance (via the mucociliary escalator and macrophage engulfment) determines lung dust burden. Key mechanisms:
- Particle uptake - Alveolar macrophages engulf silica particles; the unique surface physico-chemical properties of crystalline silica make it toxic to macrophages
- Macrophage injury - Silica induces lysosomal membrane disruption, releasing lysosomal enzymes and reactive oxygen species, leading to macrophage death
- Inflammatory cascade - Dead macrophages release silica particles which are re-engulfed by new macrophages, perpetuating an unrelenting cycle. Macrophages release pro-inflammatory and pro-fibrotic mediators (IL-1, TNF-α, TGF-β)
- Fibrogenesis - TGF-β drives fibroblast proliferation and collagen deposition, producing the characteristic whorled hyalinized collagen nodule
- Cumulative exposure - Tissue reaction severity is determined by the quantity and duration of accumulated dust and the surface physico-chemical properties of the particles
(Murray & Nadel's p. 2826; Fishman's p. 1552)
CLINICOPATHOLOGICAL TYPES
Three clinicopathological forms are recognized:
1. Chronic (Simple) Silicosis
- Most common form; follows exposure measured in decades (typically >10 years at moderate dust levels)
- Pathological hallmark: silicotic nodule - well-circumscribed, with:
- Central zone of acellular hyalinized collagen with a whorled ("onion-skin") appearance
- Peripheral zone of dust-laden macrophages
- Nodules appear first in hilar lymph nodes, then lung parenchyma
- Distribution: bilateral, predominantly upper lung zones
- May progress to complicated silicosis (PMF) with nodule coalescence
2. Accelerated Silicosis
- Follows heavier exposure over 5-10 years
- Similar pathology to chronic silicosis but more rapid progression
- Greater risk of complications (TB, autoimmune disease)
3. Acute Silicosis (Silicoproteinosis)
- Follows massive, intense, short-term exposure (weeks to 5 years) to very high concentrations of fine-particle silica
- Pathologically resembles pulmonary alveolar proteinosis - alveoli are filled with lipoproteinaceous material (PAS-positive)
- Clinically severe: rapidly progressive dyspnea, hypoxemia, respiratory failure, death
- Must be distinguished from chronic/accelerated forms clinically
(Fishman's p. 1552-1553; Murray & Nadel's p. 2344-2345)
PATHOLOGY
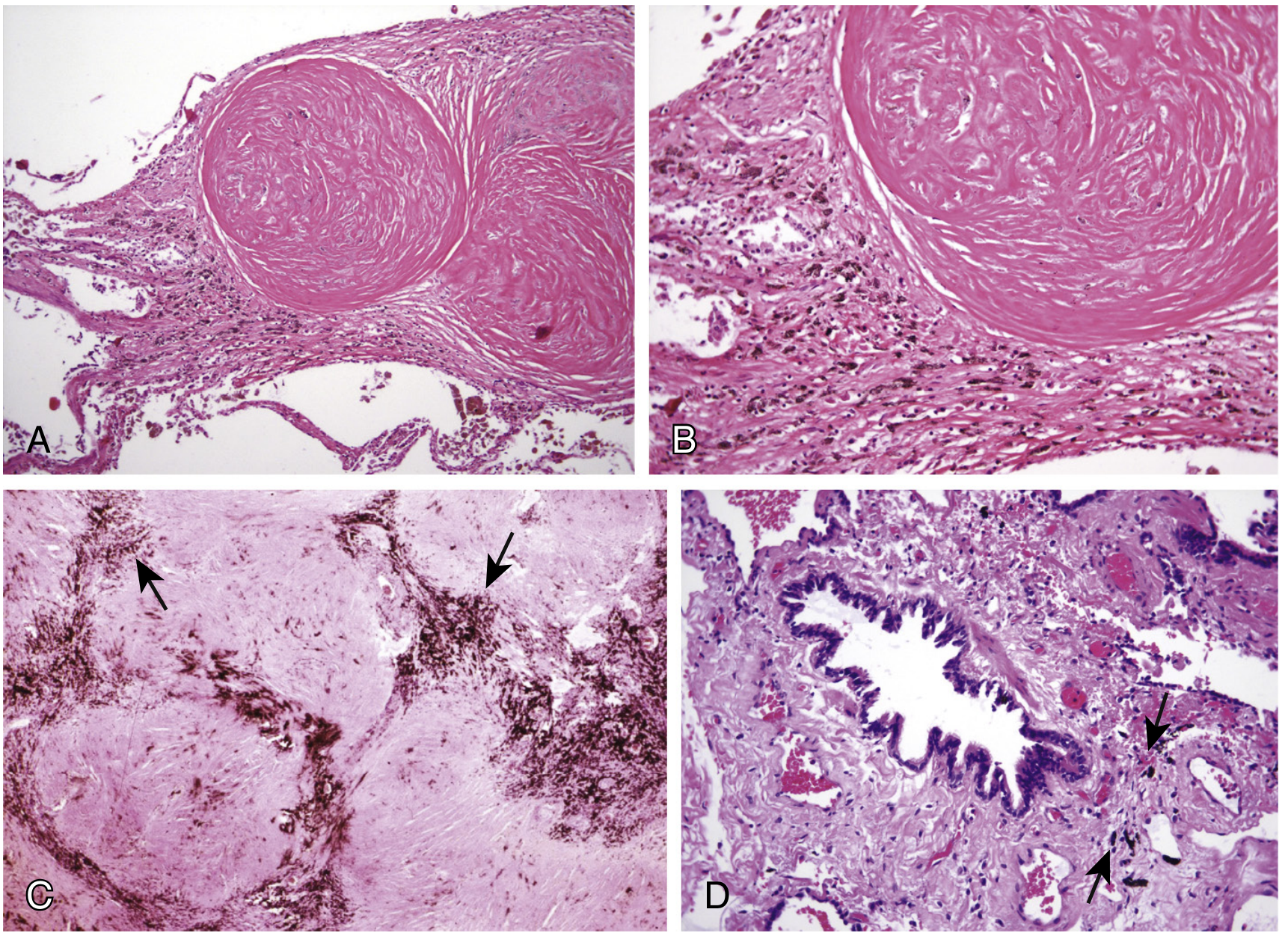
Fig. 101.3 - Pathologic lesions of chronic silicosis. (A-B) Silicotic nodule: central hyalinized whorled collagen with peripheral dust-laden macrophages. (C) PMF: confluent nodules. (D) Mineral dust small airways disease. [Murray & Nadel's, p. 2344]
Progressive Massive Fibrosis (PMF) / Complicated Silicosis:
- Nodules grow and coalesce to form lesions >1 cm (often much larger)
- Predominantly involves upper lobes
- Causes substantial scarring and volume loss
- May cavitate (raises suspicion of superimposed tuberculosis or fungal infection)
- Silicotic nodules may calcify peripherally - "eggshell calcification" of hilar/mediastinal nodes (pathognomonic)
(Murray & Nadel's p. 2344-2345; Fishman's p. 1553)
CLINICAL FEATURES
Symptoms:
- Chronic silicosis: often asymptomatic for years; progressive dyspnea on exertion is the dominant symptom; cough (with or without sputum)
- Accelerated silicosis: more rapid progression of dyspnea
- Acute silicosis: severe dyspnea, cyanosis, weight loss, and respiratory failure
- Complicated silicosis (PMF): significant dyspnea, cough with black sputum (melanoptysis)
Physical Examination:
- May be unremarkable in simple silicosis
- Advanced disease: reduced breath sounds, fine crackles, signs of cor pulmonale (right heart failure), clubbing is uncommon
(Fishman's p. 1553; Murray & Nadel's p. 2345)
RADIOGRAPHIC FEATURES
Chest X-ray:
- Small rounded opacities (nodules), predominantly in upper and mid zones, bilaterally
- ILO profusion scores used to quantify disease
- PMF: large opacities (>1 cm) in upper zones, which migrate toward the hilum as they enlarge
- Eggshell calcification of hilar/mediastinal lymph nodes (pathognomonic but not always present)
HRCT (more sensitive than CXR):
- Centrilobular and subpleural nodules, upper lobe predominance
- Branching pattern of nodules (pseudoplaque)
- Ground-glass opacity in acute silicosis
- PMF: large irregular masses with background nodules
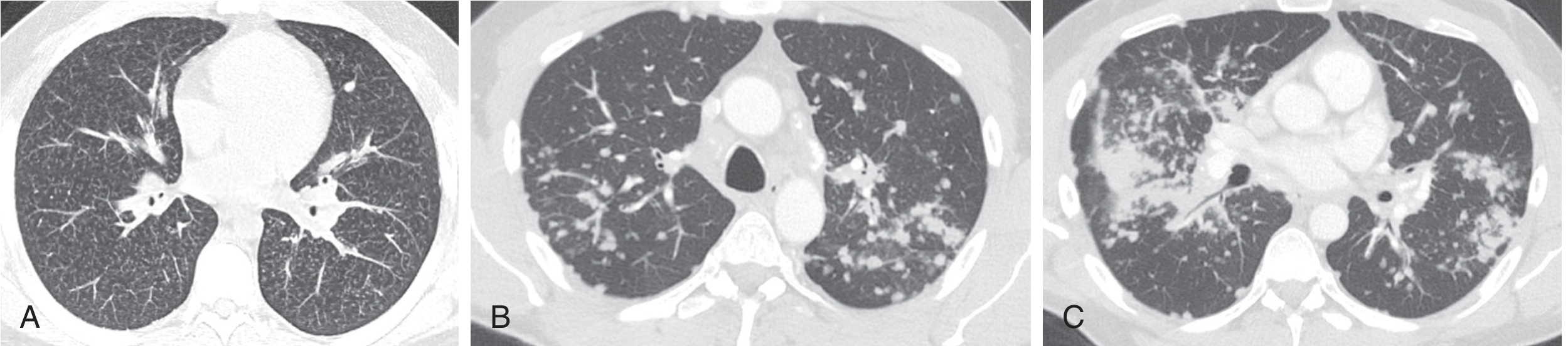
Fig. 101.4 - CT appearances: (A) micronodules, (B) simple silicosis nodules, (C) PMF [Murray & Nadel's, p. 2347]
(Fishman's p. 1553; Murray & Nadel's p. 2345-2346)
PULMONARY FUNCTION TESTS
No single characteristic pattern is present:
- May be normal in simple silicosis
- Restrictive pattern with reduced TLC, FVC (most classic)
- Obstructive pattern - actually the more common finding in many studies; silica exposure causes clinically important airflow limitation independent of radiographic abnormality (related to silica-induced emphysema)
- Mixed pattern in advanced disease
- DLCO (diffusing capacity) may be reduced, even without spirometric abnormality
- Advanced disease: severe restriction, hypoxemia, cor pulmonale
- In acute silicosis: rapid progression to gas exchange failure and respiratory failure
- 6-minute walk distance (6MWD) is a prognostic factor for hospitalization and mortality
(Fishman's p. 1553-1554; Murray & Nadel's p. 2346)
COMPLICATIONS
-
Tuberculosis (Silicotuberculosis) - Most important and serious complication
- Silica dust impairs macrophage killing of mycobacteria
- Risk of TB is substantially elevated (6-30x that of general population)
- PPD induration >10 mm is considered positive in silica-exposed workers
- Any cavitation in a silicosis patient should raise suspicion for TB
- Active TB should be treated with standard regimens; rifampicin must be included
- In miners with significant silica exposure, treatment should be more prolonged given risk of recurrence
-
Lung Cancer - In 1997, IARC reclassified crystalline silica as a Group I carcinogen ("sufficient evidence" in humans). Risk is especially elevated in those with silicosis itself. The relationship between silicosis/fibrosis and cancer continues to be studied.
-
Connective Tissue Diseases - Strong association with:
- Scleroderma (systemic sclerosis) - the "Erasmus syndrome" (scleroderma + silicosis in miners)
- Rheumatoid arthritis (Caplan's syndrome when rheumatoid nodules develop in silicotic lungs)
- SLE and ANCA-associated vasculitis
- Mechanisms likely involve silica-induced immune dysregulation
-
Renal Disease - Silica exposure associated with ~5.1% excess risk of end-stage renal disease (ESRD) and excess risk of ANCA-associated glomerulonephritis
-
Cardiovascular disease - Right heart failure (cor pulmonale) from pulmonary hypertension in advanced disease
-
Infections - In acute silicosis: Nocardia and fungal infections (in addition to TB)
(Fishman's p. 1554-1555; Murray & Nadel's p. 2345-2346)
DIAGNOSIS
The diagnosis is most commonly established on the basis of:
- Occupational exposure history - sufficient duration and intensity of crystalline silica exposure (most important - job titles alone are insufficient; a complete exposure history including military service, summer jobs, and avocations is essential)
- Characteristic chest imaging - bilateral upper-zone nodularity, with or without PMF or eggshell calcification
- Compatible clinical picture
Lung biopsy is rarely required in typical cases. It may be warranted when:
- Radiological features are atypical
- Concern for neoplasm or tuberculosis exists
- The exposure history is uncertain
When tissue is obtained, open or thoracoscopic biopsy is preferred for adequate material. EBUS-TBNA can be useful for mediastinal lymphadenopathy.
BAL and transbronchial biopsy may aid diagnosis in atypical cases.
(Fishman's p. 1554; Murray & Nadel's p. 2346)
MANAGEMENT
No specific treatment reverses established silicosis. Management is supportive and preventive:
A. Medical Treatment
- Bronchodilators - for symptomatic airflow obstruction; systemic/inhaled corticosteroids if reversible component is documented
- Oxygen therapy - indicated when PaO2 ≤55 mmHg; improves exercise tolerance, reduces dyspnea, prevents arrhythmias and polycythemia
- Vaccination - influenza and pneumococcal vaccines are recommended
- Whole lung lavage - has been used to remove accumulated dust and inflammatory mediators; evidence for routine use is insufficient but may be considered in acute/accelerated silicosis
- Antifibrotics (experimental) - Nintedanib and Pirfenidone are being investigated in trials of silicosis/pneumoconiosis given overlap with IPF pathways (TGF-β, fibroblast proliferation); NIPS trial ongoing
B. Treatment of Complications
- TB/mycobacterial disease: standard regimens including rifampicin; prolonged treatment in heavy silica-exposed miners; long-term follow-up for recurrence
- Connective tissue diseases: immunosuppressive therapy as indicated
- Cor pulmonale: standard heart failure management, oxygen
C. Lung Transplantation
- Option for end-stage disease with severe functional limitation
D. Secondary Prevention
- Removal from further silica exposure is essential
- Smoking cessation is imperative
(Fishman's p. 1554-1555; Murray & Nadel's p. 2346-2347)
PREVENTION
Prevention is the most important strategy:
- Engineering controls - wet drilling, enclosed cabs, local exhaust ventilation, substitution of non-siliceous abrasives for sandblasting
- Administrative controls - job rotation, limiting time in high-exposure areas
- Personal protective equipment - appropriate respirators (not dust masks)
- Medical surveillance - periodic chest radiographs (ILO classification) and spirometry for exposed workers
- Regulatory controls - OSHA permissible exposure limits (PEL) for respirable silica (0.05 mg/m³)
- No preventive drug therapy has proven effective
(Fishman's p. 1555; Murray & Nadel's p. 2346)
PROGNOSIS
- Chronic simple silicosis: may remain stable or slowly progress; disease can progress even after cessation of exposure
- PMF: progressive; causes significant disability and reduced lifespan
- Acute silicosis: rapidly fatal; median survival from diagnosis is 2-3 years
- Major causes of death: respiratory failure, cor pulmonale, TB, lung cancer
- Disease may progress or initially develop after cessation of exposure due to incomplete dust clearance - former silica workers should receive regular radiographic and physiologic follow-up
SUMMARY TABLE
| Feature | Chronic Silicosis | Accelerated Silicosis | Acute Silicosis |
|---|---|---|---|
| Latency | >10 years | 5-10 years | Weeks-5 years |
| Dust level | Moderate | High | Massive |
| Pathology | Silicotic nodule | Silicotic nodule | Alveolar proteinosis pattern |
| Radiology | Upper zone nodules | Upper zone nodules (faster) | Ground-glass, lower zones |
| Progression | Slow | Faster | Rapid, fatal |
| PMF risk | Yes | High | Uncommon |
Key exam points to remember:
- Silica = crystalline SiO2 (quartz most common); amorphous silica is non-toxic
- Pathological hallmark = silicotic nodule with whorled hyalinized collagen + peripheral dust-laden macrophages; upper lobe distribution
- Eggshell calcification of hilar nodes = pathognomonic
- Most important complication = silicotuberculosis; IARC Group I carcinogen
- No specific treatment; disease may progress after stopping exposure
- Lung biopsy rarely needed; diagnosis by exposure history + imaging
This is a shared conversation. Sign in to Orris to start your own chat.