Various Hepatic diseases
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have excellent content from multiple authoritative textbooks. Let me compile this into a comprehensive, well-structured overview.
Hepatic Diseases - Comprehensive Overview (Medical Student Edition)
Sources: Robbins & Kumar Basic Pathology, Schwartz's Principles of Surgery, Yamada's Textbook of Gastroenterology, Textbook of Family Medicine
Classification of Hepatic Diseases
Hepatic diseases are broadly grouped into:
| Category | Examples |
|---|---|
| Infectious / Viral | Hepatitis A, B, C, D, E |
| Toxic / Drug-induced | Alcoholic liver disease, drug-induced hepatitis |
| Metabolic / Fatty Liver | NAFLD, NASH |
| Chronic / End-stage | Cirrhosis, portal hypertension |
| Acute Failure | Acute liver failure, acute-on-chronic failure |
| Neoplastic | Hepatocellular carcinoma (HCC) |
| Genetic / Metabolic | Hemochromatosis, Wilson's disease, α1-AT deficiency |
| Autoimmune | Autoimmune hepatitis, primary biliary cholangitis |
| Vascular | Budd-Chiari syndrome, hepatorenal syndrome |
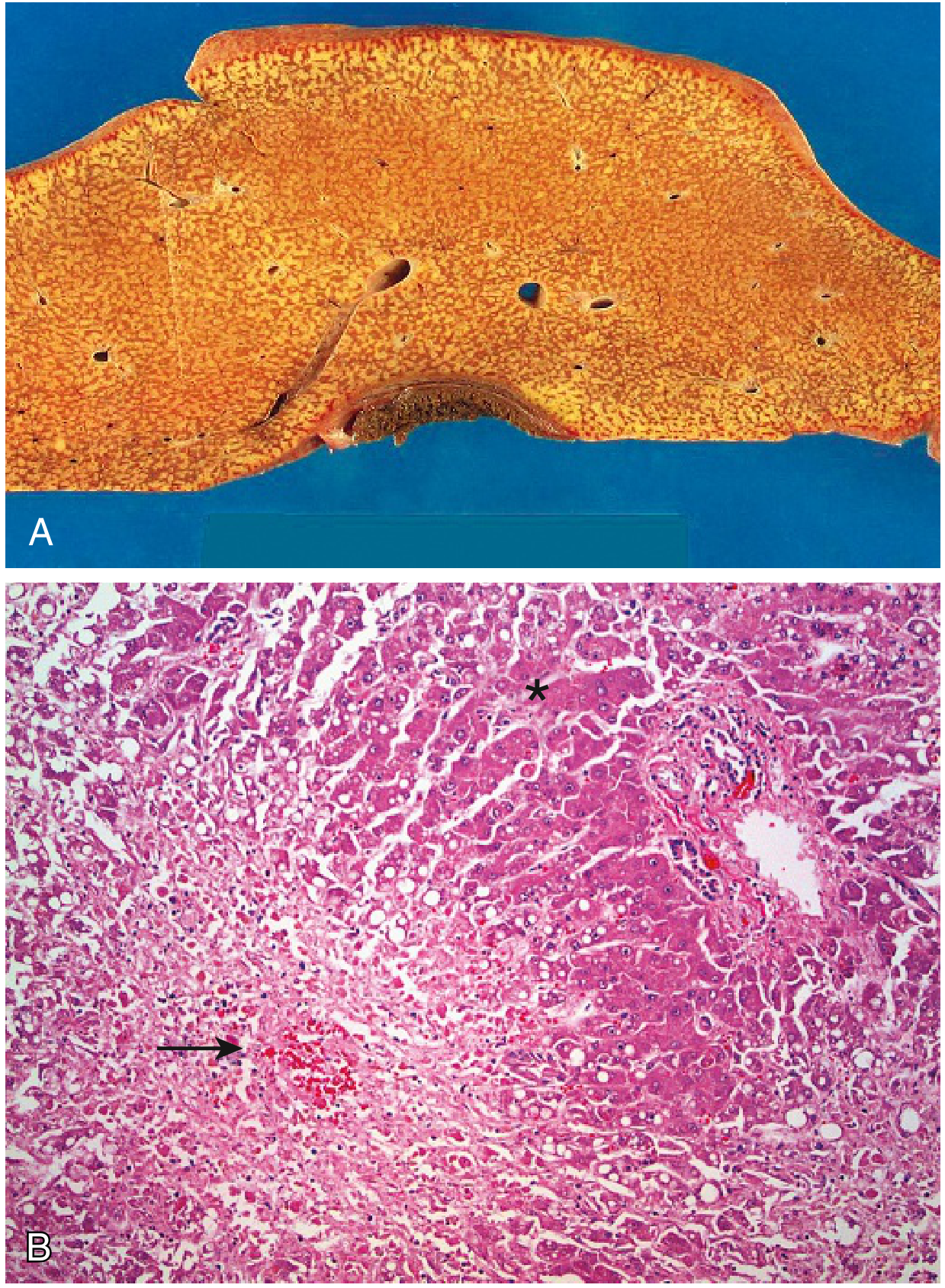
1. Acute Liver Failure (ALF)
Definition: Acute liver illness producing hepatic encephalopathy within 6 months of initial diagnosis, in the absence of prior liver disease.
Causes (US):
- ~50%: acetaminophen overdose (accidental or deliberate)
- Remainder: autoimmune hepatitis, other drugs/toxins, acute hepatitis A and B
- In Asia: hepatitis B and E predominate
Pathology (Massive Hepatic Necrosis):
- Liver is small and shrunken due to parenchymal loss
- Large zones of destruction with occasional islands of regenerating hepatocytes
- Minimal scarring (too acute)
Clinical Features:
| Feature | Mechanism |
|---|---|
| Jaundice + cholestasis | Bilirubin retention |
| Hepatic encephalopathy | Elevated ammonia (fails urea cycle); cerebral edema |
| Asterixis ("liver flap") | Ammonia-mediated CNS impairment |
| Coagulopathy | Loss of hepatic synthesis of clotting factors; paradoxic DIC |
| Portal hypertension | Ascites, hepatic encephalopathy |
| Hepatorenal syndrome | Nitric oxide-mediated splanchnic vasodilation → renal hypoperfusion |
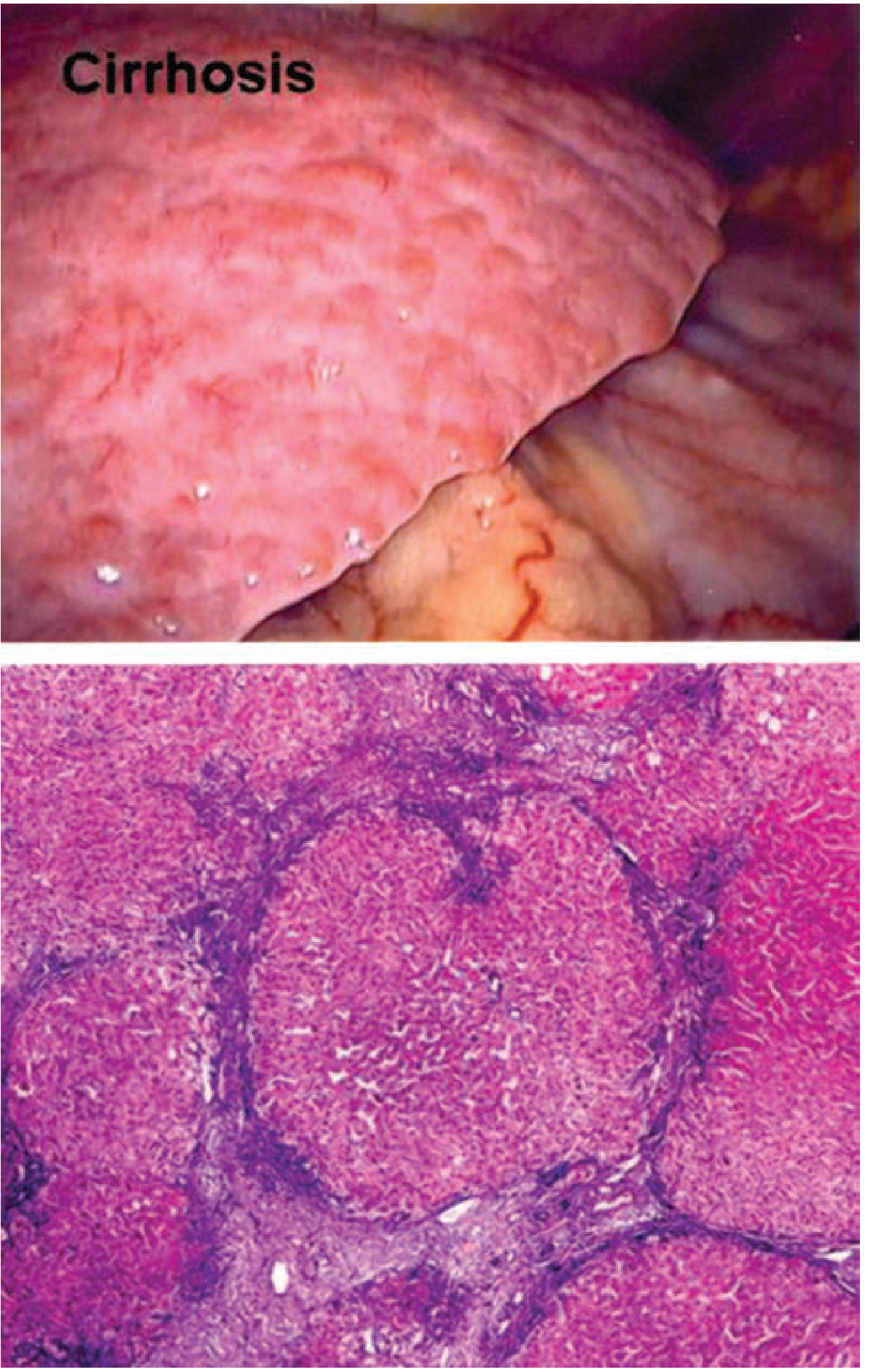
2. Cirrhosis & Chronic Liver Failure
Definition: Diffuse transformation of the entire liver into regenerative parenchymal nodules surrounded by fibrous bands - the final common pathway of chronic hepatic insult.

Etiology of Cirrhosis
| Cause | Notes |
|---|---|
| Viral hepatitis (B, C, D) | Most common globally |
| Alcohol abuse | Alcoholic hepatitis → cirrhosis |
| NAFLD/NASH | Most common chronic liver disease worldwide |
| Autoimmune hepatitis | Responds well to steroids if caught early |
| Hemochromatosis | Iron overload |
| Wilson's disease | Copper overload |
| α1-Antitrypsin deficiency | Genetic; causes lung + liver disease |
| Primary biliary cirrhosis | Autoimmune bile duct destruction |
| Budd-Chiari syndrome | Hepatic vein outflow obstruction |
| Drugs/toxins | Methotrexate, amiodarone, etc. |
| Cryptogenic | ~30% (many are unrecognized NASH) |
Morphologic Types
- Micronodular: Thick regular septa, uniform small nodules (typical of alcohol)
- Macronodular: Variable-sized septa and nodules (typical of viral hepatitis)
- Mixed: Conversion from micro to macronodular over time
Complications of Cirrhosis (End-Stage Liver Disease)
Portal Hypertension - the hallmark:
- Mechanism: Increased vascular resistance at sinusoidal level (myofibroblast contraction + scarring) + increased portal blood flow (splanchnic vasodilation)
- Results in esophagogastric varices (in ~40% of advanced disease) - risk of massive, fatal hematemesis
- Ascites - transudate; serum-to-ascites albumin gradient (SAAG) ≥1.1 g/dL
- Splenomegaly - can cause hypersplenism (thrombocytopenia, pancytopenia)
- Caput medusae - recanalization of umbilical vein
Hepatic Encephalopathy: Ammonia accumulation → CNS impairment; asterixis
Hyperestrogenemia (in males): Palmar erythema, spider angiomas, gynecomastia, hypogonadism (from impaired estrogen metabolism)
Coagulopathy: ↓ clotting factors, easy bruising, bleeding
Hepatorenal Syndrome: Nitric oxide-mediated renal hypoperfusion in absence of intrinsic renal disease
ESLD Statistics:
- 5-year mortality: 50% (70% of deaths from liver failure)
- US: ~30,000 deaths/year from cirrhosis
- Additional 10,000-12,000 deaths/year from HCC
3. Viral Hepatitis
The hepatotropic viruses share the liver as their primary target. Key comparison table:
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|---|
| Genome | ssRNA | Partial dsDNA | ssRNA | Circular defective ssRNA | ssRNA |
| Transmission | Fecal-oral | Parenteral, sexual, perinatal | Parenteral | Parenteral | Fecal-oral |
| Incubation | 2-6 wks | 2-26 wks | 4-26 wks | Same as HBV | 4-5 wks |
| Chronic hepatitis | Never | 5-10% | >80% | 10% (coinfection); 90-100% (superinfection) | Immunocompromised only |
| Fulminant | ~0.1% | 0.1-0.5% | Rare | High with superinfection | Esp. in pregnancy |
| Carrier state | No | Yes | Yes | Yes | No |
Source: Robbins & Kumar Basic Pathology, Table 14.2
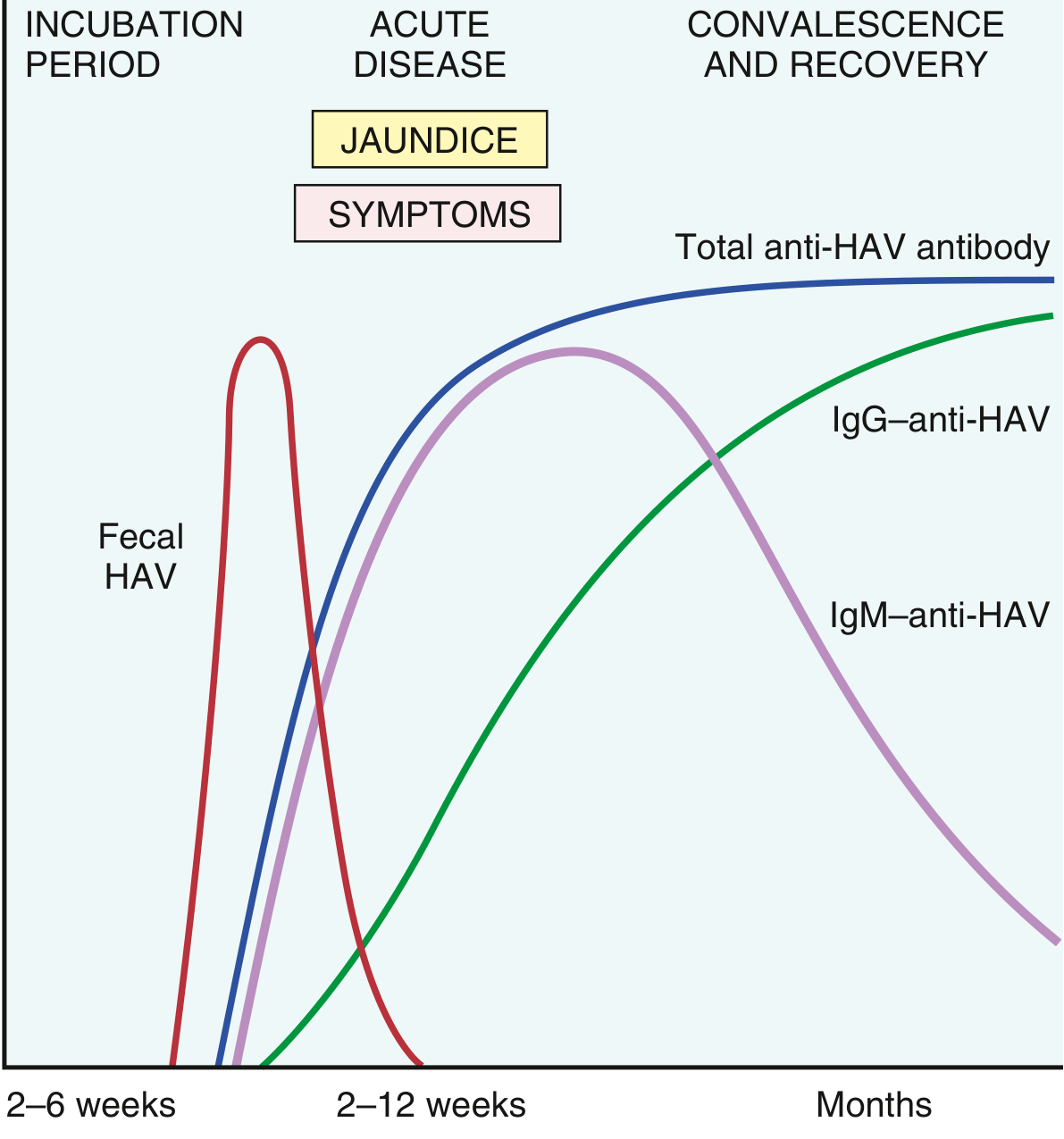
Hepatitis A (HAV)
- Picornavirus, nonenveloped ssRNA
- Fecal-oral spread; shed in stool 2-3 weeks before and 1 week after onset of jaundice
- Incubation: 2-6 weeks; endemic in areas of poor sanitation
- Self-limited - no chronic hepatitis, no carrier state
- Immunity follows infection: IgM (acute marker) then IgG (lifelong immunity)
- Rarely fulminant (~0.1%)
- Diagnosis: IgM anti-HAV (acute); IgG anti-HAV (past infection/immunity)
Hepatitis B (HBV)
- Hepadnavirus, partially double-stranded circular DNA
- Global burden: 2 billion ever infected; 250 million chronically infected; 75% of carriers in Asia/Pacific
- Transmission varies by region: perinatal (high-prevalence areas), sexual/IVDU (low-prevalence)
- Key viral antigens:
- HBsAg - surface antigen; first to appear; positivity >6 months = chronic
- HBcAg - core antigen (in hepatocytes); serum: anti-HBcAg IgM = acute infection
- HBeAg - secreted pre-core protein; marker of active replication and high infectivity
- HBV DNA - confirms active replication
| Serology | Meaning |
|---|---|
| HBsAg (+), IgM anti-HBc (+) | Acute infection |
| HBsAg (+) >6 months | Chronic infection |
| Anti-HBs (+), anti-HBc (+) | Recovered/immune |
| Anti-HBs (+) only | Vaccinated |
| Anti-HBc IgM (+), HBsAg (-) | Window period |
- Outcomes: Recovery (most adults), chronic hepatitis (5-10%), cirrhosis, HCC, fulminant (0.1-0.5%)
- Risk of chronicity is inversely proportional to age: ~90% in neonates, 5-10% in adults
- HBx protein implicated in HCC pathogenesis
- Treatment: Nucleoside analogues (tenofovir, entecavir); interferon-alpha
Hepatitis C (HCV)
- Flavivirus, ssRNA; most common cause of chronic liver disease in the US (historically)
- Spread primarily parenteral (IVDU, transfusions pre-1992, intranasal cocaine)
- >80% progress to chronic hepatitis - the highest chronicity of all hepatitis viruses
- Silent progression over decades - often discovered incidentally
- Leading indication for liver transplant in the US (now declining with DAA therapy)
- Direct-acting antivirals (DAAs): >90% sustained virologic response (SVR); have transformed management
- Genotype 1 most common in the US
Hepatitis D (HDV)
- Defective RNA virus - requires HBsAg coat to infect (cannot infect without HBV)
- Coinfection (simultaneous HBV + HDV): usually self-limited, 10% chronic
- Superinfection (HDV in chronic HBV carrier): 90-100% chronic, severe disease
Hepatitis E (HEV)
- ssRNA, fecal-oral transmission; similar to HAV epidemiologically
- Self-limited in immunocompetent hosts
- Notable exception: High mortality in pregnant women (up to 20% maternal mortality)
- Can cause chronic hepatitis in immunocompromised patients
4. Alcoholic Liver Disease (ALD)
A spectrum of hepatic injury caused by chronic alcohol use:
| Stage | Features |
|---|---|
| Hepatic steatosis | Fat accumulation in >5% of hepatocytes; reversible with abstinence |
| Alcoholic hepatitis | Hepatocyte necrosis, Mallory bodies (cytokeratin inclusions), neutrophil infiltration, perivenular inflammation; can be acute and severe |
| Alcoholic cirrhosis | Irreversible fibrosis; micronodular pattern typical |
- Key pathologic finding: Mallory-Denk bodies (eosinophilic cytoplasmic inclusions)
- Acetaldehyde, oxidative stress, and cytokines (esp. TNF-α) drive injury
- Folate deficiency contributes to disease progression
- Abstinence can lead to regression of fibrosis (even established cirrhosis in some cases)
- Lab findings: AST:ALT ratio >2:1 (almost classic for ALD); GGT elevated
5. Non-Alcoholic Fatty Liver Disease (NAFLD) / NASH
NAFLD spectrum:
- Steatosis (simple fatty liver): ≥5% hepatocytes with fat; relatively benign
- NASH (Non-alcoholic steatohepatitis): Steatosis + hepatocellular ballooning + inflammation - progressive form
- Fibrosis → Cirrhosis: ~1 in 10 NASH patients progress to cirrhosis
- NASH-associated HCC: Risk lower than HCV cirrhosis but rising due to sheer prevalence
NAFLD is now the most common chronic liver disease worldwide, driven by the obesity epidemic.
Associations: Obesity, type 2 diabetes, metabolic syndrome, dyslipidemia, insulin resistance
Diagnosis: Steatosis on imaging (US, MRI) or biopsy; NASH requires biopsy to confirm (steatosis + lobular inflammation + ballooning + exclusion of alcohol use)
Management: Weight loss, exercise, treatment of metabolic comorbidities; resmetirom (THR-β agonist) is a recently approved drug for NASH with fibrosis
Liver transplant relevance:
- Leading and fastest-growing indication for liver transplant in the US
-
30% macrovesicular steatosis in donor liver increases risk of graft failure
6. Hepatocellular Carcinoma (HCC)
Epidemiology:
- 13th most common cancer in the US; 5th most common cause of cancer death globally
- 85% of cases in low-/middle-income countries (Eastern Asia, sub-Saharan Africa)
- Most rapidly increasing neoplasm in the United States
Risk factors:
- Cirrhosis of any cause is present in 70-90% of HCC cases
- HBV + HCV account for 80% of HCC worldwide
- Aflatoxin B1 (contaminated food, Africa/Asia)
- NASH/NAFLD, alcoholic cirrhosis, diabetes (Western countries)
- Hemochromatosis, Wilson's disease, α1-AT deficiency, porphyria cutanea tarda
Presentation:
- Often asymptomatic early
- Late: jaundice, hepatomegaly, ascites, peripheral edema, RUQ pain, variceal bleeding
Diagnosis:
- AFP (alpha-fetoprotein) - elevated in many cases
- Imaging: triphasic contrast CT or MRI - nodules >1 cm with "arterial enhancement + washout" = diagnostic without biopsy
- Biopsy if imaging inconclusive
Staging: Barcelona Clinic Liver Cancer (BCLC) system - most widely used, only prospectively validated
Treatment:
- Curative: Surgical resection (70% recurrence rate), liver transplantation (Milan criteria: single lesion <5 cm OR ≤3 lesions each <3 cm)
- Locoregional: Radiofrequency ablation, transarterial chemoembolization (TACE)
- Systemic: Sorafenib, atezolizumab + bevacizumab (first-line for advanced disease)
Prognosis:
- 5-year survival: 34% (confined to liver), 12% (regional LN involvement), <3% (metastatic)
7. Genetic/Metabolic Liver Diseases
| Disease | Defect | Key Features |
|---|---|---|
| Hereditary Hemochromatosis | HFE gene mutation → iron overload | "Bronze diabetes" (skin pigmentation, cirrhosis, DM, cardiomyopathy, hypogonadism); Prussian blue stain for iron |
| Wilson's Disease | ATP7B mutation → copper accumulation | Young patient; Kayser-Fleischer rings (cornea), hepatitis/cirrhosis, neuropsychiatric symptoms; low ceruloplasmin |
| α1-Antitrypsin Deficiency | Misfolded AAT retained in ER | Liver disease (PAS+ diastase-resistant globules in hepatocytes) + emphysema |
| Primary Biliary Cholangitis (PBC) | Autoimmune destruction of intrahepatic bile ducts | Middle-aged women; pruritus, fatigue; anti-mitochondrial antibody (AMA) positive; ↑ ALP |
| Autoimmune Hepatitis | Autoimmune hepatocyte destruction | Females; ↑ IgG; anti-smooth muscle antibody (ASMA) or ANA; responds to corticosteroids |
8. Vascular Hepatic Disorders
| Condition | Mechanism | Key Features |
|---|---|---|
| Budd-Chiari Syndrome | Hepatic vein thrombosis | Painful hepatomegaly, ascites, acute liver failure; associated with hypercoagulable states, polycythemia vera, pregnancy |
| Congestive Hepatopathy | Right heart failure → hepatic venous congestion | "Nutmeg liver" (centrilobular congestion); ascites, ↑ transaminases |
| Hepatorenal Syndrome (HRS) | Functional renal failure in liver failure | No intrinsic renal disease; type 1 (acute, rapidly progressive), type 2 (slower); triggered by SBP, diuretics, GI bleed |
| Portal Vein Thrombosis | Thrombosis of portal vein | Variceal bleeding without cirrhosis; associated with prothrombotic states, abdominal sepsis |
9. Drug-Induced Liver Injury (DILI)
- One of the most common causes of acute liver failure
- Patterns: Hepatocellular (↑ ALT >> ALP), Cholestatic (↑ ALP >> ALT), or Mixed
- Key offenders:
| Drug | Pattern | Notes |
|---|---|---|
| Acetaminophen | Hepatocellular (zone 3 necrosis) | Dose-dependent; antidote: N-acetylcysteine |
| Isoniazid (INH) | Hepatocellular | Idiosyncratic; serious in elderly |
| Amiodarone | Mixed/steatohepatitis | Phospholipidosis pattern |
| Methotrexate | Fibrosis/cirrhosis | Chronic use; cumulative dose |
| Statins | Hepatocellular (usually mild) | Rarely serious |
| Alcohol | Steatohepatitis | See ALD above |
10. Key Lab Patterns (High-Yield Summary)
| Pattern | Likely Cause |
|---|---|
| ↑↑ AST, ALT (>1000 U/L) | Viral hepatitis, ischemic hepatitis, acetaminophen toxicity |
| AST:ALT >2:1 | Alcoholic liver disease |
| ↑ ALP >> ALT | Cholestatic disease (PBC, PSC, biliary obstruction) |
| ↑ Bilirubin + ↑ PT/INR | Severe hepatic dysfunction |
| ↓ Albumin + ↑ PT/INR | Chronic liver failure (poor synthetic function) |
| ↑ AFP | HCC (also seen in acute hepatitis) |
Summary: Key High-Yield Points
- Cirrhosis = final common pathway of chronic liver injury; defined by nodules + fibrous bands throughout the liver
- Portal hypertension causes the major complications: varices, ascites, encephalopathy, splenomegaly
- HCV has the highest rate of chronicity (>80%); DAAs have revolutionized treatment
- HBV risk of chronicity is inversely related to age (neonates: 90%, adults: 5-10%)
- HAV and HEV are fecal-oral, never chronic in immunocompetent (HEV: dangerous in pregnancy)
- NAFLD/NASH is now the most common chronic liver disease worldwide - driven by the obesity epidemic
- HCC arises on a background of cirrhosis in 70-90% of cases; HBV + HCV account for 80% globally
- Acetaminophen = leading cause of acute liver failure in the US; antidote is N-acetylcysteine
- Wilson's disease = suspect in young patient with hepatitis + neuropsychiatric symptoms + low ceruloplasmin
- MELD score (Model for End-Stage Liver Disease) is used to prioritize liver transplant allocation
Sources: Robbins & Kumar Basic Pathology, 10th ed. | Schwartz's Principles of Surgery, 11th ed. | Yamada's Textbook of Gastroenterology, 7th ed. | Textbook of Family Medicine, 9th ed. | Tietz Textbook of Laboratory Medicine, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.