Rnematoid arthritis
Reading File
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND treatment
Finding Sources
Searching PubMed
"rheumatoid arthritis" AND management
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I now have all the content needed for a comprehensive response. Let me compile everything.
Rheumatoid Arthritis (RA)
Definition
Rheumatoid arthritis is a chronic systemic autoimmune disorder that principally attacks synovial joints, producing a nonsuppurative, proliferative, and inflammatory synovitis. It often progresses to destruction of articular cartilage and, in some cases, bony fusion (ankylosis). Extra-articular lesions can occur in the skin, heart, blood vessels, and lungs.
- Robbins & Kumar Basic Pathology, p. 792
Epidemiology
| Feature | Detail |
|---|---|
| Prevalence | 1-2% of adults (US: 0.25-1%) |
| Sex ratio | Women : Men = 3 : 1 |
| Peak incidence | 20-50 years (third to fifth decades) |
| Genetics | ~50% of risk is inherited; HLA-DR4 strongly associated with ACPA-positive RA |
| Twins | Higher concordance in monozygotic vs dizygotic twins |
- Textbook of Family Medicine 9e, p. 877
Pathogenesis
The autoimmune response is initiated by CD4+ helper T cells reacting against joint antigens. Key mechanisms:
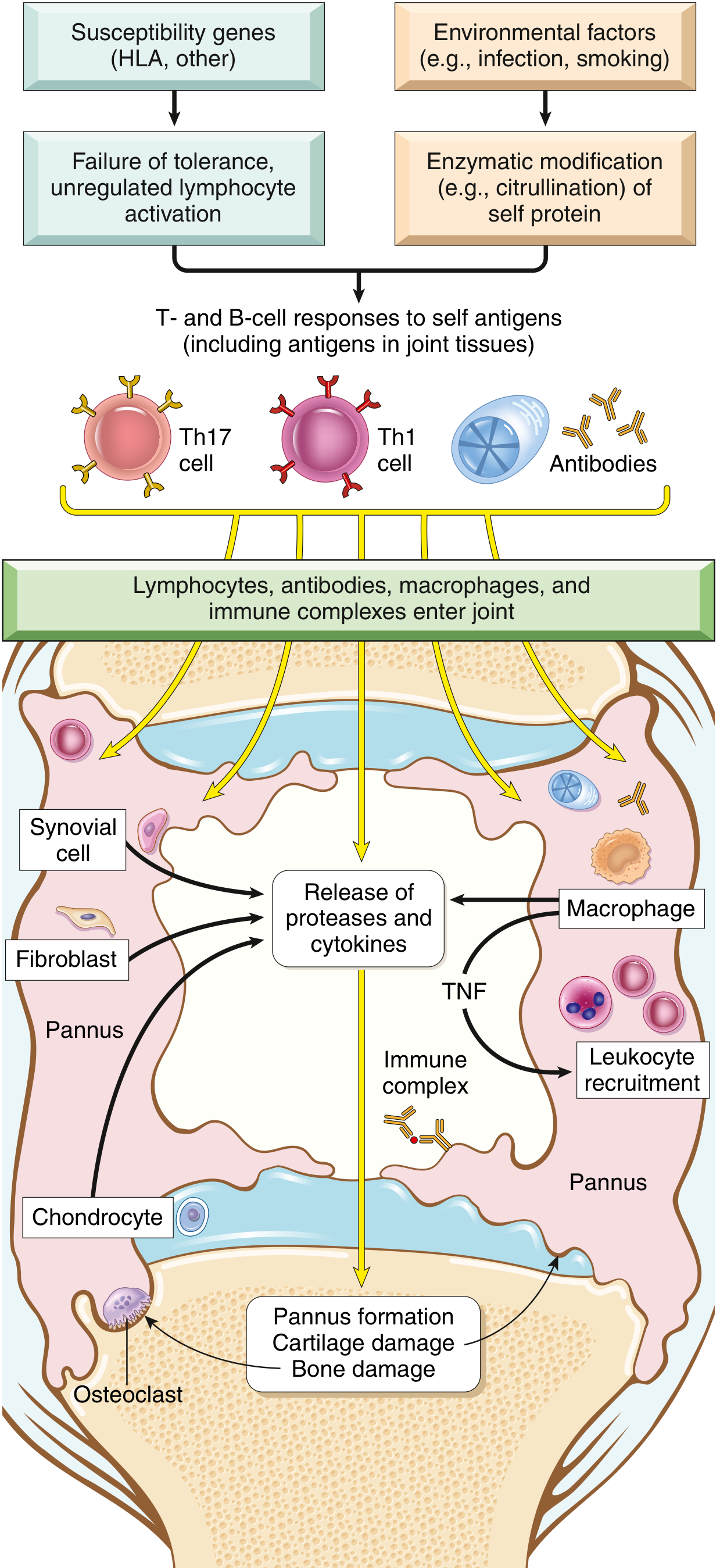
Key cytokines and effectors:
- TNF, IL-1, IL-6 (from macrophages) - recruit and activate leukocytes; stimulate proteases that destroy hyaline cartilage. TNF is considered the key mediator - hence the therapeutic efficacy of TNF antagonists.
- IL-17 (from Th17 cells) - recruits neutrophils and monocytes.
- RANKL (on activated T cells) - stimulates osteoclasts → bone resorption.
Autoantibodies:
- Anti-Citrullinated Peptide Antibody (ACPA): Targets proteins where arginine is posttranslationally converted to citrulline (fibrinogen, type II collagen, α-enolase, vinculin). Present in up to 70% of RA patients. Highly specific diagnostic marker.
- Rheumatoid Factor (RF): IgM or IgA autoantibodies binding the Fc portion of IgG. Present in ~80% of patients. Less specific - can appear in healthy individuals.
Genetic + Environmental factors:
-
HLA-DR4 allele linked to ACPA-positive RA.
-
Molecular mimicry: a citrullinated vinculin epitope resembles a microbial epitope, presented by HLA-DR4.
-
Environmental triggers include smoking, infections, and gut microbiome alterations.
-
Robbins & Kumar Basic Pathology, pp. 791-793
Morphology / Pathology
Joint changes:
- Synovium becomes edematous, thickened, and hyperplastic with villi
- Synoviocyte hyperplasia and proliferation
- Dense infiltrates of CD4+ T cells, B cells, plasma cells, and macrophages
- Increased vascularity (angiogenesis)
- Neutrophils and fibrin on synovial surfaces
- Osteoclastic activity → periarticular erosions and subchondral cysts
Pannus formation: A mass of edematous synovium, inflammatory cells, granulation tissue, and fibroblasts that grows over and erodes articular cartilage. In advanced disease, pannus bridges bones → fibrous ankylosis → bony ankylosis.
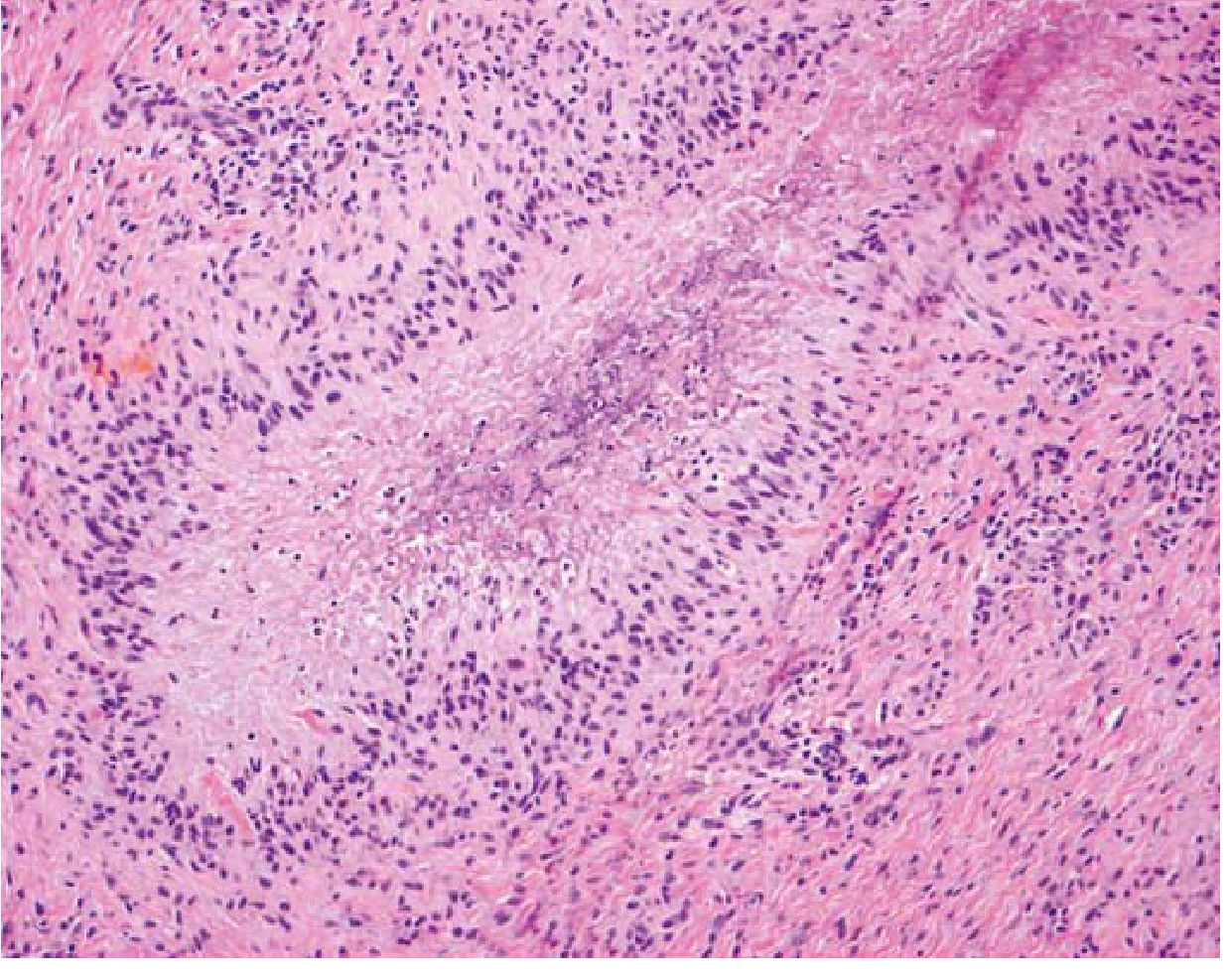
Rheumatoid nodules: Subcutaneous firm, nontender oval masses over bony prominences (forearm, elbows, occiput, lumbosacral area). Microscopically resemble necrotizing granulomas:
Clinical Features
Onset
- ~70% insidious (over weeks to months)
- ~10% acute onset (best prognosis)
- ~20% intermediate
- "Palindromic RA": brief episodes of swelling in large joints (knee, wrist) that resolve completely between attacks
Articular features
- Symmetric synovitis of small joints first - PIP, MCP joints of hands and feet
- Larger joints (wrists, ankles, elbows, knees) involved later
- Joints: swollen, warm, painful, stiff (especially in the morning)
- Morning stiffness >1 hour - hallmark
- Constitutional symptoms: fatigue, malaise, weight loss, low-grade fever, anemia
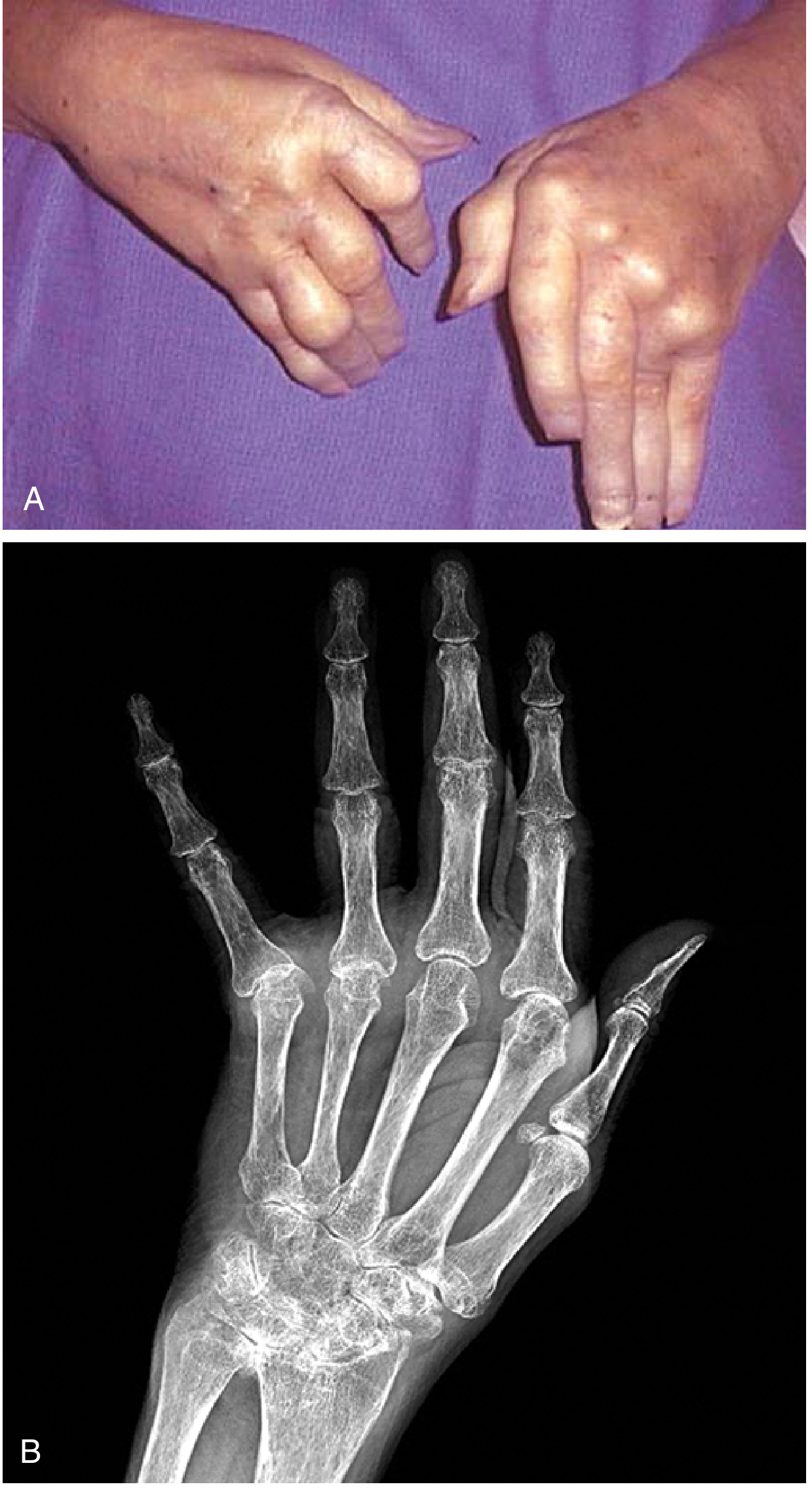
Characteristic deformities
- Ulnar deviation of fingers
- Swan-neck deformity (PIP hyperextension, DIP flexion)
- Boutonniere deformity (PIP flexion, DIP hyperextension)
Extra-articular manifestations
- Rheumatoid nodules (skin)
- Pulmonary: interstitial lung disease, rheumatoid nodules
- Cardiovascular: accelerated atherosclerosis, pericarditis
- Ocular: keratoconjunctivitis sicca (secondary Sjogren's), scleritis
- Neurological: cervical myelopathy (atlantoaxial subluxation), peripheral neuropathy
- Vasculitis
- Secondary amyloidosis (with longstanding disease)
Diagnosis
1987 ACR Revised Criteria (Traditional Format)
4 of 7 criteria required; criteria 1-4 must be present ≥6 weeks:
| # | Criterion | Definition |
|---|---|---|
| 1 | Morning stiffness | ≥1 hour before maximal improvement |
| 2 | Arthritis of ≥3 joint areas | Soft tissue swelling observed by physician (14 possible areas: PIP, MCP, wrist, elbow, knee, ankle, MTP bilaterally) |
| 3 | Arthritis of hand joints | Wrist, MCP, or PIP involvement |
| 4 | Symmetric arthritis | Same joint areas on both sides |
| 5 | Rheumatoid nodules | Over bony prominences or extensor surfaces |
| 6 | Serum RF | Positive in <5% of normals |
| 7 | Radiologic changes | Erosions or juxta-articular bony decalcification on PA hand/wrist X-rays |
Note: The 2010 ACR/EULAR criteria are now preferred for early diagnosis and emphasize joint involvement pattern, serology (RF/ACPA), acute phase reactants (CRP/ESR), and symptom duration (score ≥6/10 confirms RA).
Key laboratory tests
- RF - positive in ~80%; also positive in other conditions
- ACPA (anti-CCP) - more specific than RF; positive in ~70%; may precede symptoms by years
- ESR, CRP - elevated in active disease
- CBC - normocytic normochromic anemia is common
- Synovial fluid: >2000 WBC/mm³, predominantly neutrophils; no crystals
Imaging
- X-ray: joint space narrowing, periarticular osteopenia, marginal erosions (appear months-years after onset)
- MRI/Ultrasound: earlier detection of synovitis and erosions
Treatment
Treatment follows a treat-to-target strategy - aiming for remission or low disease activity.
DMARDs (Disease-Modifying Antirheumatic Drugs)
The backbone of RA management. Started early to prevent joint destruction.
| Drug | Class | Key Notes |
|---|---|---|
| Methotrexate | Conventional synthetic DMARD | First-line; monitor LFTs, CBC; supplement folate |
| Hydroxychloroquine | DMARD | Mild disease; retinal toxicity monitoring |
| Sulfasalazine | DMARD | Often combined with MTX + HCQ ("triple therapy") |
| Leflunomide | DMARD | Alternative to MTX |
Biologic DMARDs
Used when csDMARDs fail (typically methotrexate-refractory disease).
Anti-TNF agents (first-line biologics):
- Etanercept - subcutaneous, p75 TNF-α receptor-Fc fusion protein; alone or with MTX
- Infliximab - IV anti-TNF monoclonal antibody (75% human/25% mouse); FDA-approved only with MTX; screen for latent TB (PPD) before starting
- Adalimumab (Humira) - fully human anti-TNF; 40 mg SC every other week; greatest effect when combined with MTX
Other biologics:
- Abatacept (CTLA-4-Ig) - blocks T-cell co-stimulation
- Rituximab - anti-CD20, depletes B cells; used in RF/ACPA-positive disease
- Tocilizumab - anti-IL-6 receptor
- JAK inhibitors (tofacitinib, baricitinib) - targeted synthetic DMARDs
Important: Anti-TNF agents are not curative - patients must remain on them to avoid flares. Long-term use increases risk of opportunistic infections, particularly M. tuberculosis. Screen for latent TB before initiation.
Symptomatic therapy
- NSAIDs: Reduce pain and inflammation but do not alter disease progression. Used to bridge while awaiting DMARD effect. Risk of GI bleeding is significant (one in three RA patients hospitalized or die from GI bleed at some point).
- Glucocorticoids: Intra-articular injections (triamcinolone, methylprednisolone) for localized flares - not >3 times/joint/year. Low-dose oral prednisone as bridge therapy.
Surgery
Indicated in severe disease unresponsive to medical therapy:
- Carpal tunnel release
- Synovectomy
- Joint fusion (arthrodesis)
- Arthroplasty (joint replacement) - ~90% of older patients with severe disease achieve significant functional improvement
Prognosis
- RF-positive, polyarticular disease: >70% chance of joint damage/erosion within 2 years without treatment
- Seronegative patients may stabilize or regress
- Early, aggressive DMARD therapy substantially improves long-term outcomes
- Increased cardiovascular mortality is a major concern
Sources:
- Robbins & Kumar Basic Pathology, pp. 791-793
- Textbook of Family Medicine 9e, pp. 877-884
- Recent review: Management strategies in rheumatoid arthritis - Konzett V, Aletaha D, Nat Rev Rheumatol, Dec 2024 [PMID: 39448800]
This is a shared conversation. Sign in to Orris to start your own chat.