type 1 diabetes
Reading File
Finding Sources
Searching PubMed
"type 1 diabetes"[MeSH Terms]
Searching the Web
type 1 diabetes 2025 2026 guidelines management updates
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile a thorough, well-structured response.
Type 1 Diabetes Mellitus
Definition and Epidemiology
Type 1 diabetes (T1DM), previously called insulin-dependent diabetes, is a multisystem metabolic disease resulting from immune-mediated destruction of the insulin-producing beta (β) cells of the islets of Langerhans in the pancreas. This leads to an absolute deficiency of insulin, requiring lifelong hormone replacement.
- Affects approximately 0.2% of the U.S. population
- Peak onset at 11-12 years of age, though latent forms (LADA - Latent Autoimmune Diabetes in Adults) can present in adulthood
- Incidence appears to be increasing in North America and Europe
- About 90% or more of islets must be destroyed before clinical manifestations appear - meaning there is often a long, silent preclinical period of years
- Between 13% and 80% of patients worldwide first present with diabetic ketoacidosis (DKA) - Cellular and Molecular Immunology, p. 1286; Goldman-Cecil Medicine, 22e
Pathophysiology
Autoimmune Mechanism
β-cell destruction involves several parallel mechanisms:
- CD4+ Th1 cells reactive with islet antigens (including insulin itself)
- CD8+ cytotoxic T lymphocytes (CTLs) directly lyse islet cells
- Local cytokine production (TNF and IL-1) damages islet cells
- Autoantibodies against islet cell components
The pancreatic lesion is called insulitis - characterized by cellular necrosis and lymphocytic infiltration of both CD4+ and CD8+ T cells, macrophages. Over time, islets become completely devoid of β cells while other pancreatic cells (alpha cells, etc.) remain intact - illustrating the specificity of the autoimmune attack.
Key autoantibodies used in diagnosis and risk stratification:
- Anti-GAD65 (anti-glutamic acid decarboxylase)
- Anti-IA-2 (tyrosine phosphatase)
- Anti-IA-2β (zinc transporter)
- Anti-insulin antibodies
- Anti-ZnT8
In susceptible children who have not yet developed diabetes, the presence of islet cell antibodies is predictive of future T1DM development.
What happens without insulin
Without functional β cells, the pancreas cannot:
- Maintain low basal insulin levels (which normally suppress lipolysis, proteolysis, and glycogenolysis)
- Release a bolus of insulin in response to meals
The graph below shows the dramatic contrast in insulin response between normal subjects, T1DM, and T2DM during an IV glucose load:
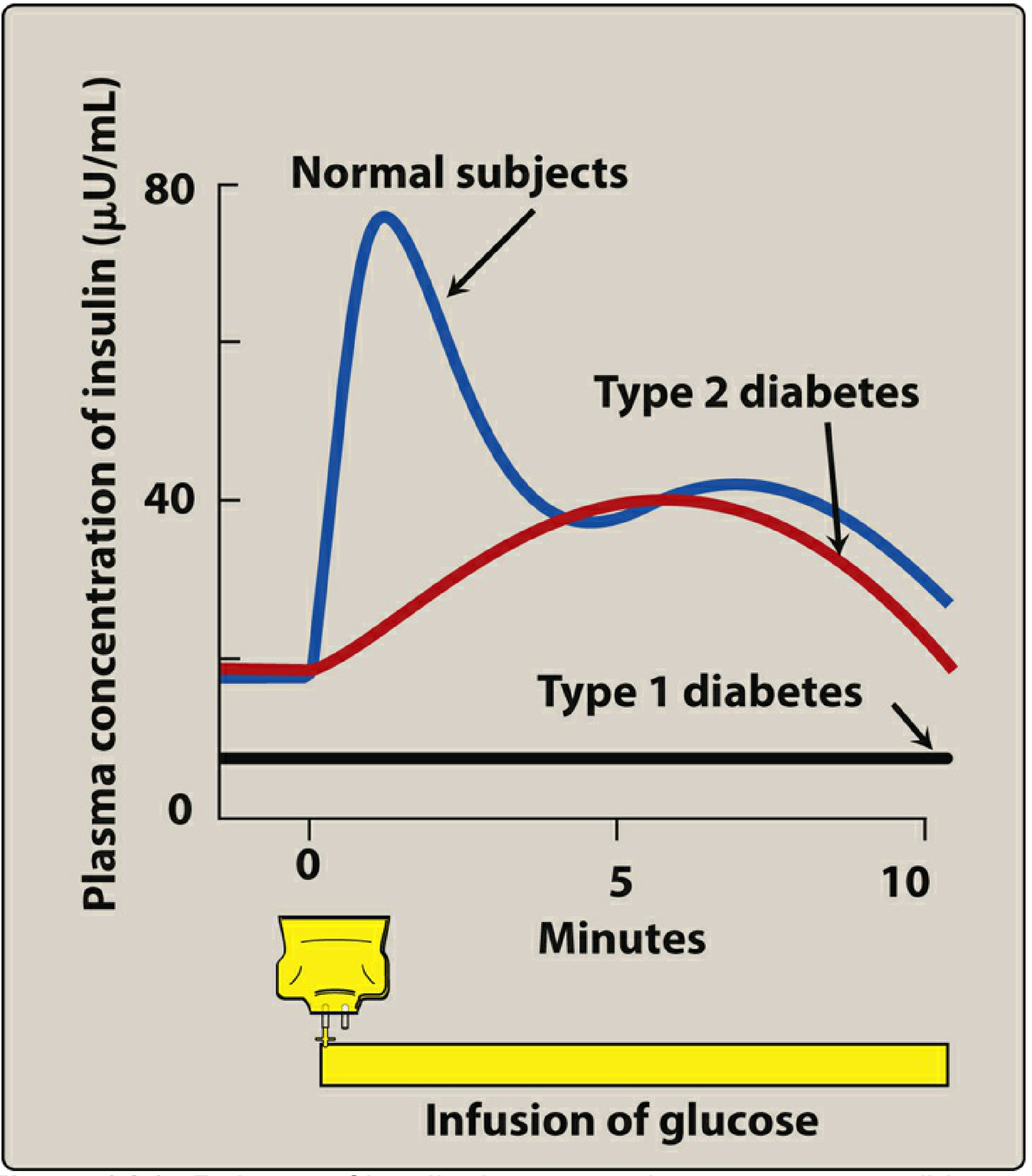
Lippincott Illustrated Reviews: Pharmacology - Figure 24.3. In T1DM, there is essentially no insulin response to glucose.
Genetics
About 60 genes are implicated in T1DM susceptibility:
- HLA genes (chromosome 6p) contribute ~50% of genetic risk
- DR4-DQ8 and DR3-DQ2 haplotypes present in ~90% of children with T1DM
- The DR3/DR4 heterozygous genotype carries the highest risk (~5%) and is most common in early-onset disease
- DR15-DQ6 is highly protective (found in only 1% of T1DM vs. 20% of the general population)
- Insulin gene (chromosome 11) - variants affect thymic insulin expression and self-tolerance
- IFIH1 (chromosome 2) - encodes a protein involved in innate RNA virus recognition; high levels may provoke exaggerated antiviral responses that trigger autoimmunity
- Twin concordance is only 30-40%, confirming essential environmental triggers
Environmental Triggers
Epidemics of mumps, rubella, and coxsackievirus have been associated with increased T1DM frequency - likely via molecular mimicry, where viral proteins resemble β-cell antigens and break self-tolerance in genetically predisposed individuals.
The SARS-CoV-2 pandemic was associated with an increase in new-onset T1DM, often presenting as an acute hyperglycemic emergency.
Clinical Presentation
Classic symptoms of insulin deficiency:
- Polydipsia (excessive thirst)
- Polyphagia (excessive hunger)
- Polyuria (increased urination)
- Weight loss
- Fatigue, blurred vision
A minority of U.S. cases, but up to 80% worldwide, first present with diabetic ketoacidosis (DKA) - more common in children under 5 and in those without access to medical care.
Honeymoon Phase
After insulin therapy is started and glucose stabilizes, many patients experience weeks to months of relatively easy control - the "honeymoon phase." This reflects partial β-cell survival (with severely reduced but not zero insulin secretion). The underlying autoimmune destruction continues, and eventually (usually within a few years) insulin requirements rise sharply as C-peptide becomes undetectable.
Diagnosis
According to the American Diabetes Association criteria:
| Test | Diabetic threshold |
|---|---|
| Fasting plasma glucose | ≥126 mg/dL (7.0 mmol/L) |
| 2-hour postprandial glucose | ≥200 mg/dL (11.1 mmol/L) |
| HbA1c | ≥6.5% |
| Random glucose with symptoms | ≥200 mg/dL |
Prediabetes: fasting glucose 100-125 mg/dL, postprandial 140-199 mg/dL, or HbA1c 5.7-6.4%.
Autoantibody testing (GAD65, IA-2, zinc transporter, insulin) helps distinguish T1DM from T2DM, especially when the presentation is ambiguous (e.g., DKA in an obese adult).
Treatment
Insulin Therapy
All patients with T1DM require exogenous insulin to sustain life. Total daily insulin requirement in adults: 0.3-1.0 unit/kg/day, with approximately half as basal and half split into premeal boluses.
Insulin preparations (Goldman-Cecil Medicine, Table 210-4):
| Type | Examples | Onset | Peak | Duration |
|---|---|---|---|---|
| Rapid-acting analogues (prandial) | Lispro, aspart, glulisine | 15-30 min | 30-90 min | 3-4 hr |
| Short-acting (Regular) | Human insulin U100/U500 | ~30 min | 2-4 hr | 5-8 hr |
| Intermediate (NPH) | Human NPH | 2-4 hr | 6-10 hr | 16-20 hr |
| Long-acting | Glargine U100, detemir | 1.5-2 hr | Peakless | 16-20 hr |
| Ultra-long-acting | Degludec, Glargine U300 | 1.5-2 hr | Peakless | 30-40 hr |
Basal-bolus regimen (MDI - Multiple Daily Injections): The preferred approach for T1DM. Uses a long-acting basal insulin (glargine or degludec) plus rapid-acting insulin before each meal (lispro, aspart, or glulisine). Prandial dose = insulin-to-carbohydrate ratio (commonly 1 unit per 10-15 g carbohydrate) + correction factor (1 unit per 1.7-3.3 mmol/L above target glucose).
Continuous Subcutaneous Insulin Infusion (CSII / insulin pump): Delivers a programmable basal rate throughout the day plus boluses at meals. Eliminates multiple injections and may provide more stable glucose. An automated/closed-loop insulin delivery system ("artificial pancreas") permits the best approximation of normal physiology and maximizes time-in-range.
Adverse effects of insulin: Hypoglycemia (most serious and common), weight gain, local injection site reactions, and lipodystrophy (minimized by rotating sites). Patients with renal insufficiency may need reduced doses.
Adjunctive Therapies
- Pramlintide (amylin analogue, 60-120 μg SC): Reduces postprandial hyperglycemia, lowers HbA1c by 0.3-0.5%, facilitates weight loss. Rarely used due to nausea and additional injections required.
- SGLT-2 inhibitors (low-dose dapagliflozin) and SGLT-1/2 inhibitor (sotagliflozin): Can lower HbA1c by 0.28-0.48% and aid weight loss. However, they carry a 3-6% risk of euglycemic DKA in T1DM. Currently approved for T1DM in many countries but not in the US or UK due to this safety concern.
Diet and Lifestyle
- Carbohydrate counting is the cornerstone of dietary management, enabling appropriate premeal dosing
- Meal-to-meal carbohydrate consistency is an alternative for those unwilling to count
- Mediterranean-style diet is recommended
- Caloric restriction is neither required nor helpful unless the patient is overweight/obese
- Physical activity affects insulin sensitivity and must be factored into dosing
Monitoring
- Self-monitoring of blood glucose (SMBG): fingerstick testing before meals and at bedtime
- Continuous Glucose Monitoring (CGM): Interstitial glucose measured every 1-5 minutes; greatly improves time-in-range and reduces hypoglycemia unawareness
- HbA1c: Monitored every 3 months; reflects average glucose over ~3 months; goal typically <7% for most adults, with individualization
Transplantation
- Whole pancreas transplant: ~70% 5-year graft survival, but complex surgery requiring lifelong immunosuppression. Reserved for patients already receiving a kidney transplant or those with severe, recurrent metabolic crises.
- Islet cell transplantation: Still largely experimental; requires immunosuppression; performed in select research centers.
- Stem cell therapy: Active area of investigation.
Prevention
Three levels of prevention are being investigated:
- Primary prevention: Inhibit development of autoimmunity before any autoantibodies appear
- Secondary prevention: Halt autoimmune progression in antibody-positive individuals before clinical onset. The monoclonal antibody teplizumab (anti-CD3) showed in a landmark trial that a single 14-day course can delay progression to clinical T1DM in high-risk relatives with multiple islet autoantibodies.
- Tertiary prevention: Slow β-cell destruction after diagnosis and prevent complications
Drugs like rituximab, cyclosporine, methotrexate, and anti-CD3 antibodies can slow progression of recent-onset diabetes, but the benefit is not sustained when immunosuppression is withdrawn.
Chronic Complications
Long-term consequences of sustained hyperglycemia affect multiple organ systems:
| Category | Manifestations |
|---|---|
| Macrovascular | Accelerated atherosclerosis - ischemic heart disease, stroke, peripheral artery disease, limb ischemia/necrosis |
| Microvascular (retina) | Diabetic retinopathy - leading cause of preventable blindness |
| Microvascular (kidney) | Diabetic nephropathy - progressive proteinuria, CKD, ESRD |
| Microvascular (nerves) | Peripheral neuropathy, autonomic neuropathy |
| Acute metabolic | Diabetic ketoacidosis (DKA), hypoglycemia |
The DCCT (Diabetes Control and Complications Trial) demonstrated that intensive insulin therapy to achieve near-normal glycemia significantly reduces the risk of retinopathy, nephropathy, and neuropathy in T1DM. The benefit persists long after the trial (metabolic memory, shown in the follow-up EDIC study).
Sources: Cellular and Molecular Immunology (Abbas et al.), Goldman-Cecil Medicine International Edition, Lippincott Illustrated Reviews: Pharmacology, Harrison's Principles of Internal Medicine 22e (2025), Tietz Textbook of Laboratory Medicine 7e.
This is a shared conversation. Sign in to Orris to start your own chat.