Explain anatomy and conduction system of heart including heart valves being anaesthesia pg
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Barash Clinical Anesthesia (9th edition) and Gray's Anatomy for Students. Let me compile a thorough, well-structured answer.
Anatomy and Conduction System of the Heart - Anaesthesia PG
Sources: Barash, Cullen & Stoelting's Clinical Anesthesia 9e (Chapter 12: Cardiac Anatomy and Physiology); Gray's Anatomy for Students; Fuster & Hurst's The Heart 15e
1. GROSS ANATOMY
The Heart as a Pump
The heart is a phasic, electrically self-actuated, variable-speed hydraulic pump composed of two dual-component elastic muscular chambers (right and left), each with an atrium and ventricle. Both sides simultaneously eject equal quantities of blood into the pulmonary and systemic circulations.
- Barash Clinical Anesthesia, p. 842
The Cardiac Skeleton
The cartilaginous skeleton is located at the "base" (superior aspect) of the heart and forms its structural foundation. It consists of:
- Valve annuli (mitral, tricuspid, aortic, pulmonic)
- Aortic and pulmonary arterial roots
- Central fibrous body
- Left and right fibrous trigones
Three functions of the cardiac skeleton:
- Support the macroscopically avascular valve leaflets
- Resist forces of developed pressure and blood flow
- Provide sites of insertion for superficial subepicardial muscle
The skeleton also acts as an electrical insulator between atria and ventricles - critical for sequential atrial-then-ventricular contraction.
- Barash, p. 842-843
Myocardial Structure
The ventricular walls consist of three muscle layers:
- Deep sinospiral - interdigitating
- Superficial sinospiral
- Superficial bulbospiral
- LV wall thickness: ~10 mm (ellipsoidal shape, high-pressure systemic pump)
- RV wall thickness: ~5 mm (crescent-shaped, lower-pressure pulmonary pump)
- Subendocardial and subepicardial LV fibers follow orthogonal, oblique, helical routes - the orientation reverses at the LV midpoint, resembling a flattened "figure of eight"
An interstitial collagen network with interwoven elastin provides structural support, flexibility, and elasticity.
Right vs Left Ventricle
| Feature | Right Ventricle | Left Ventricle |
|---|---|---|
| Shape | Crescent-shaped | Ellipsoidal |
| Wall thickness | ~5 mm | ~10 mm |
| Function | Low-pressure pulmonary circuit | High-pressure systemic circuit |
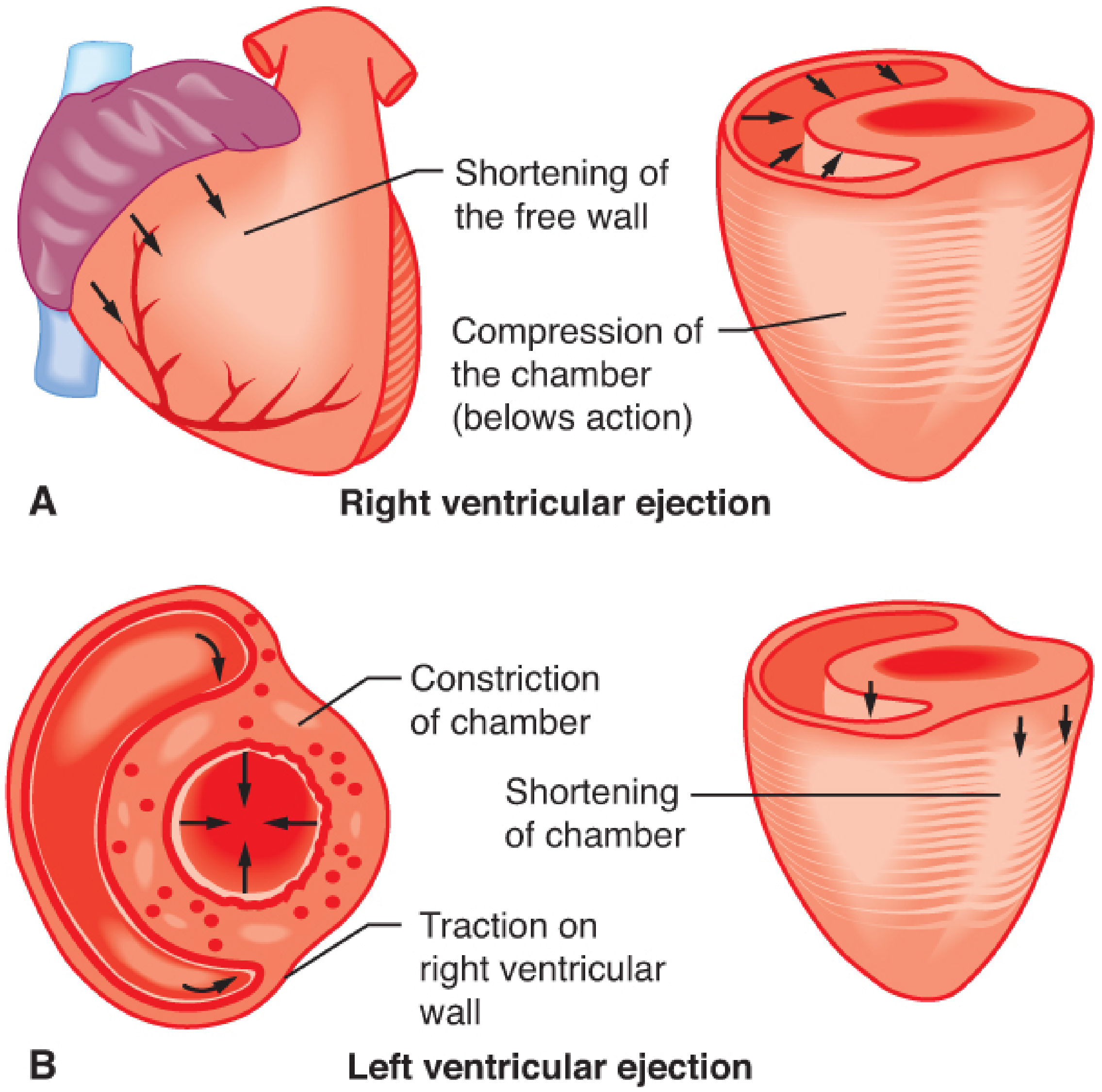
| Contraction pattern | Peristaltic "bellows" action | Circumferential squeeze + shortening |
| Pressure-volume work | 1x | 5-7x greater than RV |
The RV moves toward the septum using a "bellows-like" action, with the septum and LV providing a "splint." LV contraction contributes significantly to RV systolic function. The thinner RV is more vulnerable to acute afterload increases but accommodates excess volume more easily than the LV.
2. HEART VALVES
Two pairs of valves ensure unidirectional blood flow.
Semilunar Valves (Outlet Valves)
Aortic Valve
- Trileaflet structure at the LV outlet
- Leaflets named by relationship to coronary ostia: right coronary, left coronary, and non-coronary (posterior) cusps
- Opens passively with LV ejection; closes when ejection ceases
- Proximal aortic root contains sinuses of Valsalva above each leaflet - these facilitate hydraulic vortices (eddy currents) that:
- Prevent leaflets from adhering to the aortic wall
- Prevent coronary ostia occlusion during systole
- Keep leaflets mobile during early diastole for rapid closure
- Effective orifice area during peak ejection nearly equals cross-sectional annular area
Pulmonic Valve
- Trileaflet at the RV outlet
- Leaflets named by anatomic position: right, left, and anterior
- The proximal pulmonary artery does NOT contain sinuses of Valsalva
- Operates at lower pressures (~25 mmHg systolic)
Atrioventricular Valves (Inlet Valves)
Mitral Valve
- Separates LA from LV; two leaflets - anterior and posterior
- Oval, saddle-shaped structure
- Anterior (aortic) leaflet: oval-shaped, occupies greater central annular diameter, forms the convex border at coaptation
- Posterior leaflet: crescent-shaped, extends further around the annular circumference
- Area of each leaflet is similar
- Leaflets join at anterolateral and posteromedial commissures
- Chordae tendineae from leaflets attach to anterolateral and posteromedial papillary muscles
- The posteromedial papillary muscle is particularly vulnerable to ischemia because it is often supplied by a single coronary artery (either RCA or LCCA, ratio 2:1), unlike the anterolateral papillary muscle which has dual supply from LAD and LCCA
Tricuspid Valve
- Separates RA from RV; three leaflets - anterior, posterior, and septal
- Larger annular diameter than mitral valve
- Chordae from the septal leaflet attach to the septomarginal trabecula and papillary muscles of the RV
Anaesthetic Relevance of Valves
- AV valve annuli become sites of abscess in infective endocarditis
- Mitral valve prolapse (myxomatous degeneration) is the most common valvular abnormality
- Aortic stenosis (calcific degenerative) is the most common acquired valve lesion in adults - creates fixed afterload, making these patients sensitive to vasodilation under anaesthesia
- Prosthetic valves require anticoagulation (mechanical) or carry risk of structural degeneration (bioprosthetic)
3. CARDIAC CONDUCTION SYSTEM
The conduction system initiates and coordinates contraction through a unidirectional pathway of excitation. Key components:
Components and Hierarchy
SA Node → Internodal Pathways → AV Node → Bundle of His →
Bundle Branches (R + L) → Purkinje Fibers → Ventricular Myocardium
Sinoatrial (SA) Node
- Primary pacemaker of the heart
- Located at the superior end of the crista terminalis, at the junction of the superior vena cava and right atrium
- This is also the junction between embryonic sinus venosus and atrium proper
- Intrinsic rate: 60-100 bpm
- Spontaneous depolarization initiates each cardiac cycle
- Blood supply: SA nodal artery (branch of RCA in ~55-60%, LCx in ~40-45%)
- Barash, p. 848; Gray's Anatomy for Students
Internodal Pathways
From the SA node, depolarization spreads through the RA via three pathways:
- Anterior internodal pathway (James)
- Middle internodal pathway (Wenckebach)
- Posterior internodal pathway (Thorel)
Bachmann's bundle (a branch of the anterior internodal pathway) transmits SA depolarization from the RA to the LA across the atrial septum, enabling simultaneous atrial contraction.
Note: Internodal pathways are clearly identified in the electrophysiology laboratory but are difficult to identify histologically - an important distinction from the AV node and His-Purkinje system.
Atrioventricular (AV) Node
- Located near the opening of the coronary sinus, close to the attachment of the septal cusp of the tricuspid valve, within the atrioventricular septum (Koch's triangle)
- Functions:
- Slows conduction (~0.1 sec delay) - allows atrial contraction to complete before ventricular contraction (atrial "kick")
- Acts as a gatekeeper - limits ventricular rate during atrial tachyarrhythmias
- Acts as secondary pacemaker (intrinsic rate 40-60 bpm) if SA node fails
- Blood supply: AV nodal artery (from RCA in ~90% = right dominant circulation)
- The cartilaginous skeleton electrically insulates atria from ventricles, so AV node + His bundle are the ONLY normal pathway for atrial impulses to reach ventricles
- Barash, p. 848; Gray's Anatomy
Bundle of His (Atrioventricular Bundle)
- Direct continuation of AV node
- Pierces the fibrous skeleton of the heart to enter the interventricular septum
- Travels along the lower border of the membranous part of the interventricular septum
- Divides into right and left bundle branches at the muscular interventricular septum
- Blood supply: Dual - LAD + RCA (most protected segment of conduction system)
Bundle Branches
Right Bundle Branch (RBB):
- Continues on the right side of the interventricular septum toward the apex of RV
- Enters the septomarginal trabecula (moderator band) to reach the base of the anterior papillary muscle
- Relatively thin, susceptible to block
Left Bundle Branch (LBB):
- Passes to the left side of the muscular interventricular septum
- Descends toward the apex of the LV
- Divides into:
- Left anterior fascicle (LAF) - supplies anterosuperior LV wall
- Left posterior fascicle (LPF) - supplies posteroinferior LV wall (thicker, dual blood supply = more resistant to block)
- Sometimes a septal fascicle
Purkinje Fibers (Subendocardial Conduction Plexus)
- Located within the inner one-third of the ventricular walls
- Extremely rapid conduction velocity (~4 m/s, vs 0.05 m/s in AV node)
- Establishes a unidirectional wave of excitation from papillary muscles and apex toward the arterial outflow tracts
- Large branches insulated from myocardium by connective tissue - reduces inappropriate stimulation
- Intrinsic rate: 20-40 bpm (tertiary pacemaker)
- Barash, p. 848-849; Gray's Anatomy for Students
Conduction Velocities Summary
| Structure | Conduction Velocity | Intrinsic Rate |
|---|---|---|
| SA node | Slow | 60-100 bpm |
| Atrial muscle | 1.0 m/s | - |
| AV node | 0.05 m/s (slowest) | 40-60 bpm |
| Bundle of His | 1.0 m/s | - |
| Bundle branches | 2.0 m/s | - |
| Purkinje fibers | 4.0 m/s (fastest) | 20-40 bpm |
| Ventricular muscle | 0.5 m/s | - |
4. ANAESTHETIC IMPLICATIONS OF CONDUCTION SYSTEM
Artificial Pacing and Dyssynchrony
- Epicardial RV pacing during cardiac surgery bypasses the normal His-Purkinje system
- Produces dyssynchronous LV activation → uncoordinated contraction → may decrease LV EF
- Chronic RV apical pacing causes detrimental changes in LV geometry and function
- Basis for Cardiac Resynchronization Therapy (CRT) in HFrEF with LBBB
- Barash, p. 849
Accessory Pathways
- Pathologic direct connections (e.g., bundle of Kent in Wolff-Parkinson-White syndrome) bypass the AV node between atria and ventricles
- Precipitate reentrant supraventricular tachyarrhythmias
- Anaesthetic consideration: avoid agents that slow AV conduction (digoxin, verapamil) in WPW - can increase anterograde conduction down accessory pathway
Blood Supply to Conduction System
| Structure | Primary Supply | Clinical Risk |
|---|---|---|
| SA node | RCA (55-60%) or LCx (40-45%) | Inferior MI → sinus bradycardia |
| AV node | RCA (90%) | RCA occlusion → AV block |
| Bundle of His | Dual LAD + RCA | Protected |
| RBB | LAD (septal perforators) | LAD occlusion → RBBB |
| LBB - ant. fascicle | LAD | LAD occlusion → LAHB |
| LBB - post. fascicle | LAD + RCA (dual) | Resistant to block |
Impact of Anaesthetic Agents on Conduction
- Volatile agents (sevoflurane, isoflurane): prolong AV nodal conduction (PR interval), may enhance vagal tone
- Propofol: can cause bradycardia; rare reports of bundle branch block at high doses
- Dexmedetomidine: sinus bradycardia, AV block via alpha-2 agonism
- Succinylcholine: transient sinus bradycardia (especially with repeat dosing), can cause junctional rhythms
- Neostigmine: increased vagal tone → bradycardia, AV block (always given with anticholinergic)
- Regional anaesthesia (high spinal/epidural): sympathetic blockade at T1-T4 → blocks cardioaccelerator fibres → bradycardia, risk of complete heart block if baseline conduction disease present
5. CORONARY BLOOD SUPPLY - QUICK SUMMARY FOR ANAESTHESIA
- Left Anterior Descending (LAD): anterior LV wall, apex, anterior 2/3 of IVS, anterolateral papillary muscle (partial)
- Left Circumflex (LCx): lateral and posterolateral LV wall, anterolateral papillary muscle (partial)
- Right Coronary Artery (RCA): RV free wall, inferior LV wall, posterior 1/3 IVS (right dominant), SA node, AV node, posteromedial papillary muscle
Right dominance (RCA supplies posterior descending artery - PDA): ~80% of population
Left dominance (LCx supplies PDA): ~20%
Left dominance (LCx supplies PDA): ~20%
LV coronary flow occurs almost entirely during diastole because extravascular compressive forces occlude intramural vessels during systole. Tachycardia reduces diastolic time and can compromise subendocardial perfusion - especially dangerous in the presence of coronary artery stenosis or LV hypertrophy.
Key Anaesthesia Exam Points
- The cardiac skeleton electrically isolates atria from ventricles - AV node is the only normal conduction pathway between them.
- SA node is at the SVC-RA junction (crista terminalis); AV node is near the coronary sinus ostium (Koch's triangle).
- The posteromedial papillary muscle has single coronary supply (RCA or LCx) - most vulnerable to ischemic mitral regurgitation.
- The aortic sinuses of Valsalva prevent coronary ostia occlusion during systole; the pulmonary artery has none.
- AV node delay (0.05 m/s) allows atrial "kick" to complete before ventricular systole - losing this in AF reduces CO by ~20-30%.
- RV pacing dyssynchrony reduces LV EF even without ischemia.
- AV nodal artery comes from RCA in ~90% - inferior MI (RCA territory) → heart block risk.
- LV O2 extraction is near-maximal at baseline (~75%) - increases in demand require proportional increases in coronary flow (not increased extraction).
Primary references:
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th edition, Chapter 12 (pp. 839-901)
- Gray's Anatomy for Students, 4th edition
- Fuster & Hurst's The Heart, 15th edition
This is a shared conversation. Sign in to Orris to start your own chat.