I need to know everything about Tavi. Make notes about that procedure, everything, uh, whatever that you can find online. It has to be a really comprehensive notes which covers every single thing, including the procedural steps, the complications, how to handle them. Whatever you can find about Tavi, create a comprehensive notes for me.
TAVI TAVR transcatheter aortic valve implantation comprehensive procedure steps complications 2024 2025
"transcatheter aortic valve implantation" TAVI complications management
https://eurointervention.pcronline.com/article/complications…
TAVI (Transcatheter Aortic Valve Implantation) - Comprehensive Notes
1. BACKGROUND & HISTORY
- First-in-human TAVI performed by Alain Cribier in 2002 in an inoperable patient with severe aortic stenosis (AS)
- FDA approvals:
- 2011: Prohibitive surgical risk (STS predicted 30-day mortality >50%)
- 2012: High surgical risk (STS >10% or ≥2 frailty indices)
- 2016: Intermediate risk (STS 4%-8%)
- 2019: Low risk (STS ≤4%)
- TAVI surpassed SAVR as the most common procedure for isolated AS in the USA in 2016
- Over 70,000 TAVI procedures performed in the USA annually
- Over 95% performed via the transfemoral route
- A Heart Team approach is mandated - both a cardiac surgeon and interventional cardiologist must evaluate and perform the procedure together (CMS mandate 2023: minimum 20 procedures/year per centre)
2. PATHOPHYSIOLOGY - AORTIC STENOSIS (INDICATION FOR TAVI)
- Severe AS is defined echocardiographically by:
- Aortic valve area (AVA) < 1.0 cm²
- Mean gradient > 40 mmHg
- Peak aortic jet velocity > 4 m/s
- Symptomatic AS carries 50% mortality at 1 year without intervention
- Classic triad of symptoms: Angina, Syncope, Dyspnoea (heart failure) - median survival after onset: 5 years, 3 years, 2 years respectively
3. INDICATIONS FOR TAVI
Established Indications
- Symptomatic severe AS with any surgical risk, including low risk
- Age ≥ 80 years with no transfemoral contraindication - TAVI preferred over SAVR
- Age 65-80 - shared decision making; either TAVI or SAVR acceptable
- Age < 65 or life expectancy > 20 years - SAVR recommended (limited long-term TAVI data)
- Predicted post-TAVI survival > 12 months with acceptable quality of life (high/prohibitive risk)
Special Indications (per Sabiston)
- Bioprosthetic aortic valve degeneration (Valve-in-Valve TAVI) - FDA approved 2015
- Heavily calcified ("porcelain") ascending aorta
- Prior chest radiation
- Re-sternotomy cases
- Bicuspid aortic valve disease (off-label, selected patients)
- Aortic insufficiency (pure AI - off-label)
- Concomitant percutaneous coronary intervention in intermediate-risk patients with non-complex CAD
AHA/ACC 2020 Guidelines Summary (Class of Recommendation)
| COR | Recommendation |
|---|---|
| I (A) | < 65 years or life expectancy > 20 years → SAVR |
| I (A) | Age 65-80, no anatomic contraindication to TF-TAVI → either SAVR or TAVI after shared decision-making |
| I (A) | > 80 years or life expectancy < 10 years, no TF contraindication → TAVI preferred |
| I (A) | Any age with high/prohibitive surgical risk, predicted survival > 12 months → TAVI |
| I (C-EO) | Predicted survival < 12 months or minimal QoL improvement → palliative care |
| 2b (C-EO) | Critically ill with severe AS → balloon aortic valvuloplasty as bridge |
4. CONTRAINDICATIONS
Absolute Contraindications
- Expected survival < 12 months even after TAVI
- No improvement in quality of life expected
- Anatomy unsuitable for any access route
- Active infective endocarditis of the aortic valve
Relative Contraindications for Transfemoral Route
- Significant peripheral vascular disease (small/tortuous iliofemoral vessels)
- Previous femoral artery surgery with scarring
Contraindications Specific to Transapical TAVI
- Recent MI within 3 months
- Severe pulmonary dysfunction
- Presence of an LV apical thrombus
Anatomical Factors Favouring SAVR Over TAVI
- Bicuspid aortic valve with complex anatomy (especially with prominent calcified raphe)
- Heavy LVOT calcification
- Coronary ostia very close to the annulus
- Need for concomitant procedure (e.g. ascending aortic replacement)
5. VALVE DEVICES
Types of Valves
A. Balloon-Expandable Valve (BEV)
- Prototype: Edwards SAPIEN series (SAPIEN, SAPIEN XT, SAPIEN 3, SAPIEN 3 Ultra)
- Bioprosthetic valve crimped onto a balloon catheter
- Advanced across the aortic annulus; balloon inflated to expand and lock the prosthesis into the native annulus
- More precise positioning
- Less paravalvular regurgitation with newer-generation valves
B. Self-Expanding Valve (SEV)
- Prototype: Medtronic CoreValve, CoreValve Evolut R, Evolut PRO, Evolut FX
- Tissue valve sewn into a self-expanding nitinol frame
- Crimped within delivery catheter, advanced across the valve, then catheter withdrawn - allows the frame to expand
- Can be repositioned or recaptured before full deployment (with newer designs)
- Higher rates of pacemaker implantation than BEV historically
Key Valve Sizing Principle
- CT-based aortic annulus measurement is the gold standard (ECG-gated, IV contrast, <1 mm slices)
- Valve is selected to achieve a 0-20% oversizing relative to the annulus
- Under-sizing → paravalvular leak; over-sizing → annular rupture risk
6. PREPROCEDURAL WORKUP & PATIENT SELECTION
Multidisciplinary Heart Team
CT Angiography (TAVI Protocol CT)
- Aortic annulus: size (for valve sizing), shape (circular vs elliptical), calcification
- LVOT: calcification (risk of rupture), significant septal hypertrophy (risk of malalignment)
- Coronary ostia distance from the annular plane (risk of coronary obstruction)
- Ascending aorta: aneurysm, calcification (porcelain aorta)
- Aortic arch: calcium burden (stroke risk)
- Iliofemoral vessels: diameter (minimum ~5.0-6.0 mm for most sheaths), calcification, tortuosity
- Aortic valve: valve morphology (tricuspid vs bicuspid), calcification pattern
Frailty Assessment (Sabiston Table)
- Frailty > 2/5 score → no clear advantage for either TAVI or SAVR
Echocardiography (TTE/TEE)
- Confirm diagnosis of severe AS
- Assess LV function (EF), wall motion, MR, other valvular disease
- Annulus dimensions (supplemental to CT)
Pre-procedure Cardiac Catheterisation
- Coronary angiography to assess CAD (PCI may be performed first or concurrent)
Conduction System Evaluation
- Baseline ECG mandatory
- Pre-existing QRS > 120 ms, any AV block, fascicular block → higher risk of requiring permanent pacemaker
Haematological & Renal Workup
- Renal function (contrast nephropathy risk)
- Group & crossmatch
- Coagulation studies
7. ACCESS ROUTES
A. Transfemoral (TF) - Most Common (~95% of all TAVI in USA)
- Percutaneous retrograde access via the common femoral artery (CFA)
- Preferred due to lowest complication rates
- Requires adequate CFA/iliac diameter, limited calcification, acceptable tortuosity
- Can be performed under conscious sedation ("minimalist approach") at many centres
- Vascular closure with suture-based devices (ProGlide, MANTA)
B. Transapical (TA)
- Small left anterolateral mini-thoracotomy to expose the LV apex
- Device advanced directly into the LV between purse-string sutures (pledget-reinforced)
- Antegrade approach to the aortic valve
- Advantage: avoids crossing diseased aortic arch (reduces calcium embolism risk)
- Requires general anaesthesia
- Now < 1% of TAVI in USA due to increased morbidity
- Contraindicated if: LV apical thrombus, recent MI < 3 months, severe pulmonary dysfunction
C. Transaortic (TAo) - Direct Aortic
- Surgical access to the ascending aorta via partial sternotomy or right anterior mini-thoracotomy
- Used when femoral access is unfeasible
D. Transaxillary / Transsubclavian
- Access via the subclavian/axillary artery
- Used when femoral access is prohibited
- ~4% of TAVI in USA as part of "alternative access"
E. Transcarotid
- Direct carotid artery cut-down; primarily left carotid
- Alternative when axillary/femoral not suitable
F. Transcaval
- Transcaval puncture from the IVC to the descending aorta; rare, specialised centres
8. PROCEDURAL STEPS
Pre-procedural Setup
- Setting: Hybrid operating room or cardiac catheterisation lab (CCL) with:
- State-of-the-art fluoroscopy/angiography
- Echocardiography capability (TTE and TEE)
- Emergency supplies including CPB perfusionist access and cardiac surgeon standby
- Monitoring lines placed:
- Large-bore IV access (×2)
- Arterial line (radial artery) - for continuous BP, rapid pacing response monitoring
- Central venous line if comorbidities indicate
- External defibrillation pads connected before start
- Temporary pacing lead:
- Placed via femoral vein (or IJ/subclavian) into the right ventricle
- Ensures reliable rapid pacing before and during valve deployment
- For transapical cases: sewn directly to epicardium
- Anaesthesia:
- General anaesthesia (GA) with TEE for transapical/alternative access
- Conscious sedation ("minimalist approach") increasingly used for transfemoral TAVI
- TEE introduced after GA induction to confirm anatomy and assess post-deployment result
- Heparin anticoagulation (target ACT > 250-300 sec) initiated
Step-by-Step Procedure (Transfemoral as Prototype)
- Percutaneous puncture of the common femoral artery
- "Pre-close" with 2x ProGlide suture-based closure devices (deployed before the large sheath)
- Also access the contralateral femoral artery for placement of a pigtail catheter (angiography, haemodynamic monitoring, side-access for emergencies)
- Femoral vein access for temporary pacing wire
- Baseline aortic gradient measured
- Fluoroscopic co-planar angulation optimised (LAO/RAO + cranial/caudal) to achieve a perpendicular view of the aortic valve plane
- Stiff-tipped guidewire (e.g. Amplatz Extra Stiff) introduced via the aortic sheath
- Catheter advanced retrograde across the stenotic aortic valve
- Guidewire placed deep into the LV apex for stability throughout the procedure
- A balloon catheter is advanced over the guidewire to the aortic valve
- Rapid RV pacing at 180 beats/min initiated to reduce cardiac output (prevents balloon ejection during inflation)
- Balloon inflated to dilate the stenotic native aortic valve, creating space for the prosthesis
- Balloon deflated; pacing stopped; haemodynamics allowed to recover
- Fluoroscopic assessment of the calcification pattern (identifies optimal deployment position)
- Note: Pre-dilation with BAV is not always required with newer-generation valves - direct implantation increasingly used
- Selected prosthetic valve is crimped onto the delivery system in a sterile field
- For BEV (e.g. SAPIEN 3): valve crimped onto the balloon catheter using a dedicated crimper
- For SEV (e.g. CoreValve): valve loaded within the delivery catheter housing
- Delivery system advanced over the stiff guidewire, through the aortic sheath, retrograde across the native aortic valve
- Positioned within the native aortic annulus under combined fluoroscopic and echocardiographic (TEE or TTE) guidance
- Optimal position: prosthesis straddling the annulus, approximately 50% below the annular plane (varies by valve type)
- Pigtail in the non-coronary cusp (NCC) used as fluoroscopic landmark
- Final angulation checked for perpendicularity to the valve plane
- For BEV: Rapid RV pacing reinitiated → balloon inflated under pacing → valve expanded and locked into position → balloon deflated, pacing stopped
- For SEV: Valve deployed by gradual withdrawal of outer sheath, allowing self-expansion; pacing used at critical deployment phases
- Modern SEVs (Evolut R, PRO) allow repositioning and recapture before full deployment if positioning is suboptimal
- Aortography from contralateral pigtail to assess for:
- Paravalvular leak (PVL) - location and severity
- Coronary perfusion (ostial patency)
- Prosthesis position
- TEE/TTE assessment to confirm:
- Valve function and leaflet motion
- Transvalvular gradient (should be low, < 10 mmHg mean)
- Degree of paravalvular regurgitation
- LV function
- Pericardial effusion
- ECG monitoring for new conduction abnormalities (LBBB, CHB)
- If PVL is significant (moderate-severe) → post-dilation with balloon can be performed
- Temporary pacing wire left in situ until conduction stability confirmed
- Arterial sheath removed; pre-close sutures deployed for haemostasis
- Femoral access site checked by fluoroscopy/angiography; additional manual compression or surgical repair if needed
- Heparin reversed with protamine if needed (for bleeding control)
- Patient transferred to coronary care unit or high-dependency unit
- Continuous invasive arterial pressure monitoring ≥2 hours post-procedure
- ECG monitoring for conduction abnormalities
- Sedation/anaesthesia reversed as early as possible ("fast-track" protocol)
- Aggressive treatment of post-procedure hypotension (tamponade, bleeding must be excluded first)
9. ANAESTHESIA CONSIDERATIONS (Miller's Anesthesia 10e)
General Anaesthesia (GA)
- Required for transapical and most alternative-access procedures
- Standard ASA monitors + arterial line + large-bore IV
- TEE introduced after induction - confirms anatomy, guides positioning, assesses result
- External defibrillation pads placed before procedure (VF risk from catheter manipulation/rapid pacing)
- Neuromuscular block maintained during critical steps
Minimalist / Conscious Sedation Approach (Transfemoral)
- Replacing GA at many centres for uncomplicated TF-TAVI
- Benefits: faster recovery, earlier mobilisation, shorter hospital stay
- TEE replaced by TTE or pure fluoroscopic guidance at some centres
- Need for bail-out conversion to GA must be anticipated (LMA or ETT available)
Rapid Ventricular Pacing
- Heart paced at 180 beats/min (sometimes up to 220 bpm) to transiently suppress cardiac output
- Used during:
- BAV (balloon valvuloplasty)
- BEV deployment
- Phases of SEV deployment requiring stillness
- Haemodynamic collapse expected during pacing - arterial line waveform used to confirm effectiveness
- Duration should be minimised; watch for VF on reinstatement of native rhythm
CPB Availability
- CPB perfusionist and cardiac surgeon must be immediately available throughout the procedure
- CPB set up and ready to run within minutes
10. COMPLICATIONS - CLASSIFICATION & MANAGEMENT
A. VASCULAR COMPLICATIONS
Access Site Haemorrhage
- Most common complication in early TAVI era
- Causes: repeated arterial punctures, sheath tear of femoral artery, inadvertent subcutaneous dissection
- Minor: managed with prolonged manual compression, balloon tamponade
- Major (arterial rupture):
- Immediate recognition (sudden BP drop, groin haematoma)
- Emergency aortography from contralateral access site
- Introduce soft aortic occlusion balloon - inflate to control bleeding
- Protamine given to reverse heparin
- Balloon inflation at low pressure for 10 minutes often seals small leaks
- Large tears/ruptures → covered stent deployment or emergency surgical repair
- Abort procedure and reschedule if haemorrhage is too significant to proceed safely
Iliac/Aortic Dissection or Perforation
- Recognised on fluoroscopy/angiography
- Managed with endovascular stenting or surgical repair
B. STROKE / NEUROLOGICAL EVENTS
- Incidence: 2-3% (clinical stroke); subclinical MRI lesions are much more common (up to 80%)
- Risk factors: heavy aortic arch calcification, previous stroke, atrial fibrillation, heavy native valve calcium
- Mechanism: Embolisation of calcium debris, air emboli, or thrombus during valve manipulation
- Prevention:
- Meticulous de-airing of all catheters and delivery systems
- Maintain ACT > 250-300 sec (adequate anticoagulation)
- Minimise catheter manipulations in the aortic arch
- Embolic protection devices (EPD) - e.g. Sentinel (Claret Medical): two filters placed in brachiocephalic and left carotid arteries to capture emboli; recent meta-analyses (PMID 41121677) show benefit in reducing stroke/lesion burden
- Management:
- Stroke usually diagnosed post-procedure
- Immediate neurological assessment; CT head
- Acute stroke protocol activation (thrombolysis/thrombectomy if appropriate)
- Neurology consultation
C. PARAVALVULAR REGURGITATION (PVL)
- Incidence (older generation valves): 30-50% mild, 10-15% moderate-severe; newer generation valves have substantially lower rates
- Cause: incomplete apposition of the prosthesis to the native annulus due to calcification, undersizing, or malpositioning
- Mild PVL: clinically acceptable; monitor
- Moderate-Severe PVL: associated with increased late mortality
- Intraoperative Management:
- Identify location (TEE - all views; aortography) - anterior/posterior/left/right circumferential
- Post-dilation: inflate balloon inside deployed valve (higher risk of annular injury, conduction issues)
- Valve-in-valve implantation if leak is large and position is correctable
- Surgical conversion in extreme cases
- Notes: Small annulus in women results in less PVL; oversizing increases risk of annular rupture
D. CONDUCTION DISTURBANCES / PACEMAKER REQUIREMENT
- Left Bundle Branch Block (LBBB): most common new conduction finding; 30-60% with SEV, lower with BEV
- Complete Heart Block (CHB): most serious; risk 10-25% with SEV, lower (5-10%) with BEV
- Predictors of pacemaker need:
- Pre-existing RBBB
- QRS duration > 120 ms
- Any degree of AV block pre-procedure
- Deep valve implantation (greater sub-annular depth)
- Heavy membranous septum calcification
- Prevention: GLUCO-TAVI trial (2026, PMID ref) investigated glucocorticoids to reduce PPM rates
- Management:
- Post-procedure ECG monitoring for 48-72 hours
- Temporary pacing wire kept in place until conduction stability confirmed
- Permanent pacemaker implanted if CHB persists or if symptomatic high-degree AV block
- Recent STS/ACC TVT Registry: PPM rate ~10.8%
E. ANNULAR RUPTURE
- Rare but catastrophic (0.5-1%)
- Mechanism: Oversizing the valve relative to the annulus, particularly with heavy LVOT/annular calcification
- Presentation: sudden haemodynamic collapse, haemopericardium, haemothorax
- Risk factors: LVOT calcification, small annulus, oversized valve selection
- Management:
- Immediate recognition (sudden haemodynamic collapse during deployment)
- Emergency pericardiocentesis for tamponade
- CPB initiation
- Emergency surgical repair (may require full aortic root surgery)
- Very high mortality
F. CORONARY OBSTRUCTION
- Incidence: ~0.7-1.0% overall; higher in valve-in-valve procedures
- Mechanism: Native valve leaflet or prosthesis frame displacing/blocking coronary ostium
- Risk factors: Short distance from annulus to coronary ostia (< 10-12 mm), heavy leaflet calcification, bulky native leaflet tissue (especially in bioprosthetic ViV-TAVI), female sex (shorter coronary heights)
- Presentation: Sudden ST elevation, ventricular failure, haemodynamic collapse immediately after valve deployment
- Prevention:
- CT pre-planning to measure coronary heights
- BASILICA technique (Bioprosthetic or native Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction) - electrosurgical laceration of valve leaflet prior to TAVI
- "Chimney stent" technique - pre-positioning coronary guide wire/stent to rescue coronary if obstruction occurs
- Management:
- Wire and balloon into affected coronary immediately
- Emergency PCI (balloon dilation, stenting)
- If not re-openable → CPB and surgical coronary revascularisation
G. VALVE EMBOLISATION / MALPOSITIONING
- Valve migrates too far into the aorta or ventricle after deployment
- Causes: Undersizing, insufficient pacing during deployment, significant septal hypertrophy (causes positional instability), valve not properly seated
- Aortic embolisation (valve migrates up into ascending aorta):
- Can sometimes be retrieved and repositioned
- May require surgical removal
- Ventricular embolisation (valve migrates into LV):
- Snaring and retrieval possible but technically challenging
- Emergency surgery may be required
H. CARDIAC TAMPONADE
- Incidence: ~1-2%
- Causes: Annular rupture, LV perforation by guidewire/temporary pacing wire, catheter perforation
- Presentation: Beck's triad (hypotension, muffled heart sounds, JVD), haemodynamic collapse; confirmed by echocardiography
- Management:
- Immediate echocardiographic confirmation
- Emergency pericardiocentesis (drain and leave catheter in situ)
- If due to annular rupture or major perforation → CPB and surgical repair
I. LEAFLET THROMBOSIS
- Subclinical bioprosthetic leaflet thrombosis (HALT) on CT: ~10-15% at 30-90 days
- Clinical leaflet thrombosis: ~0.5% but associated with stroke and valve dysfunction
- Higher rates in TAVI versus SAVR (likely due to different haemodynamic environment)
- Presentation: Elevated gradients on echo follow-up; may present with TIA/stroke
- Management:
- Anticoagulation (warfarin, DOACs) - usually resolves leaflet thrombus
- Monitor with CT/echo
- Post-TAVI, Goldman-Cecil: 3 months aspirin alone preferred over DAPT in patients without indication for anticoagulation
J. ACUTE KIDNEY INJURY (AKI)
- Contrast nephropathy from CT + procedural contrast
- New-onset dialysis requirement: < 0.5% (Sabiston TVT Registry data)
- Prevention: Hydration, minimise contrast dose, N-acetylcysteine in some centres, consider CO2 angiography
K. BLEEDING
- Major access site bleeding and retroperitoneal haematoma
- Managed with blood transfusion, reversal of anticoagulation, endovascular or surgical repair
L. INFECTIVE ENDOCARDITIS (IE) POST-TAVI
- Rare but serious late complication
- Systematic review (PMID 41529748, 2026): Invasive vs conservative management - mortality significantly lower with surgery in those who are surgical candidates
- Pathogens: Staphylococcus, Enterococcus, Streptococcus
- Management: Prolonged IV antibiotics; surgical/transcatheter re-intervention in selected cases
11. COMPARISON: TAVI vs. SAVR
| Feature | TAVI | SAVR |
|---|---|---|
| Approach | Minimally invasive / percutaneous | Open heart surgery with CPB |
| 30-day mortality (STS/ACC registry) | ~2.6% | Higher in high-risk patients |
| Stroke rates | Lower (transfemoral) | Higher in high-risk |
| Pacemaker need | Higher (5-25% depending on valve type) | Lower |
| Paravalvular leak | Higher (though much lower with newer valves) | Rare |
| Leaflet thrombosis | Higher | Lower |
| Hospital stay | Significantly shorter | Longer |
| Return to activity | Faster | Slower |
| AF risk | Lower | Higher |
| Long-term durability | Still under study (5-10yr data emerging) | Well established |
| Preferred age | >65-80 (especially >80) | <65 or life expectancy >20 years |
- PARTNER series (PARTNER 1, 2, 3) - landmark RCTs establishing TAVI from high risk to low risk
- Evolut Low Risk trial - SEV vs SAVR in low-risk patients: noninferior at 24 months
- PARTNER 3 - BEV vs SAVR in low-risk: TAVI superior at 1 year (composite of death, stroke, rehospitalisation)
- 5-year Evolut LR data (2023): HR 0.74 (95% CI 0.54-1.00) for death/disabling stroke with SEV-TAVI vs SAVR
12. VALVE-IN-VALVE (ViV) TAVI
- Treatment of failed bioprosthetic aortic valves using TAVI inside a degenerated surgical or transcatheter bioprosthesis
- FDA approved in 2015
- Volume has increased sharply over 5 years
- Key consideration: smaller effective orifice area (risk of patient-prosthesis mismatch - PPM)
- Higher risk of coronary obstruction than native-valve TAVI
- BASILICA technique increasingly used in ViV procedures
- Meta-analysis (PMID 39976067, 2025, >20,000 patients): TAVI-in-failed-bioprosthesis vs surgery outcomes
13. TAVI IN BICUSPID AORTIC VALVE (BAV)
- Excluded from landmark RCTs
- Challenges: asymmetric calcification, eccentric valve opening, raphe - leads to eccentric/underexpanded prosthesis
- Higher risk: PVL, annular rupture, pacemaker
- Still considered in selected patients unsuitable for SAVR, particularly those without prominent calcified raphe
- Off-label indication
14. POST-PROCEDURAL MANAGEMENT
Immediate (First 24-48 hours)
- ICU/CCU monitoring
- Continuous ECG (pacemaker threshold checks if temporary wire in situ)
- Invasive BP monitoring ≥2 hours
- Treat hypotension aggressively (exclude tamponade/bleeding first, then give fluids/vasopressors)
- Monitor potassium and blood gases (especially if sedation/hypoventilation)
- Echocardiogram at 24-48 hours
Antithrombotic Therapy (Post-TAVI)
- No indication for anticoagulation: Aspirin 75-100 mg monotherapy for 3 months (Goldman-Cecil 2024); DAPT (aspirin + clopidogrel) no longer preferred - non-inferior but not superior with more bleeding
- AF or another anticoagulation indication: Anticoagulate (NOAC/warfarin); aspirin can be added
- After 3 months: Lifelong aspirin monotherapy unless anticoagulation indicated
Follow-up Echocardiography
- Discharge echo
- 30-day follow-up echo
- Annual thereafter to monitor:
- Valve gradients (structural deterioration)
- PVL progression
- LV function recovery
- Leaflet thickening (HALT)
Endocarditis Prophylaxis
- Dental/procedural prophylaxis as per guidelines (bioprosthetic valve in aortic position)
Activity
- Mobilise early (often same-day or next-day for TF-TAVI)
- Driving typically allowed at 2-4 weeks
- Return to normal activity much faster than SAVR
15. OUTCOMES DATA
| Parameter | Value (STS/ACC TVT Registry) |
|---|---|
| 30-day mortality | ~2.6% |
| 30-day stroke | ~2.3% |
| Permanent pacemaker at 30 days | ~10.8% |
| New-onset dialysis | <0.5% |
| Procedural success | >95% in appropriately selected patients |
- Mortality at 1 year for high-risk patients reduced from 51% (medical Rx) to 31% with TAVI (Goldman-Cecil)
- Women: higher vascular/bleeding complications but lower 1-year mortality than men in multiple trials
16. FUTURE DIRECTIONS & SPECIAL TOPICS
Asymptomatic AS
- Randomised trial of TAVI vs conventional care in asymptomatic AS patients (results expected ~2024-2025)
Redo TAVI (TAVI-in-TAVI)
- Growing clinical scenario as first-generation TAVI valves degenerate
- Major procedural complications (valve embolisation, annular rupture, open conversion) are rare
- Coronary obstruction rates: 0-2% in selected cohorts (lower than expected)
- PPM rates < 10% (Annals of Cardiothoracic Surgery 2025 review)
- TAVI explant surgery is increasingly discussed as an alternative for younger patients
Aortic Insufficiency (Pure AI)
- TAVI is challenging in pure AI (no calcium to anchor valve)
- Dedicated self-expanding devices being developed/studied
- Off-label use increasing
TAVI and Coronary Interventions
- EuroIntervention 2026 state-of-the-art paper: TAVI + coronary interventions - timing (staged vs concomitant), technical considerations, access management
- Systematic review (PMID 39054901): PCI strategies in AS patients undergoing TAVI
Embolic Protection
- Sentinel Cerebral Protection System: Captures emboli from brachiocephalic + left carotid arteries during TAVI
- Updated meta-analysis (PMID 41121677, 2025): Supports use, particularly in high-risk neurological anatomy
Glucocorticoids to Reduce PPM
- GLUCO-TAVI randomised trial (EuroIntervention 2026): Investigating whether peri-procedural steroids reduce permanent pacemaker implantation rates post-TAVI
17. QUICK-REFERENCE COMPLICATION SUMMARY TABLE
| Complication | Incidence | Key Prevention | First-line Management |
|---|---|---|---|
| Vascular/access site injury | 10-15% (all grades) | Careful CT sizing, closure device technique | Balloon tamponade, covered stent, surgery |
| Stroke | 2-3% | De-airing, adequate ACT, EPD | Neurology, thrombolysis/thrombectomy |
| Paravalvular leak (mod-severe) | <5% (new generation) | CT sizing, optimal positioning | Post-dilation, valve-in-valve |
| Pacemaker requirement | 10.8% (all-comers) | ECG screening, valve depth control | Temporary then permanent pacemaker |
| Coronary obstruction | ~1% | CT planning, BASILICA, chimney stent | Emergency PCI, surgery if needed |
| Annular rupture | 0.5-1% | Avoid oversizing, LVOT Ca² screening | CPB, emergency surgery |
| Valve embolisation | Rare | Correct sizing, adequate pacing | Snare retrieval, surgery |
| Tamponade | ~1-2% | Careful wire handling | Pericardiocentesis, CPB if annular tear |
| Leaflet thrombosis | 0.5% clinical | Adequate anticoagulation protocol | Anticoagulation |
| AKI | ~5% | Hydration, minimise contrast | Supportive, dialysis if needed |
Search for latest clinical images and anatomical diagrams of TAVI techniques
TAVI TAVR anatomical diagrams clinical images access routes valve deployment 2024 2025
TAVI - Clinical Images & Anatomical Diagrams
1. TAVI Valve Devices: Balloon-Expandable vs Self-Expanding
Balloon-Expandable Valve (BEV) - Edwards SAPIEN type

Self-Expanding Valve (SEV) - Medtronic CoreValve type

2. Access Route Anatomy: Transapical vs Transfemoral
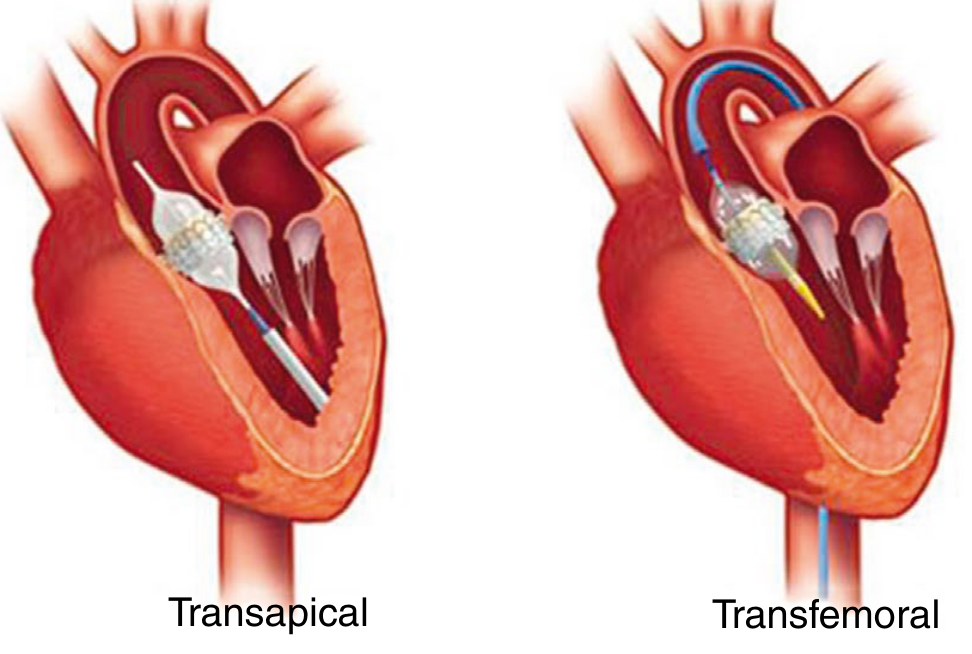
- Transapical: Device enters the LV between purse-string sutures; antegrade passage avoids the diseased aortic arch and reduces calcium embolism risk
- Transfemoral: Retrograde passage across the stenotic native valve; requires adequate iliofemoral vessel diameter (typically ≥5.5-6 mm for current sheaths)
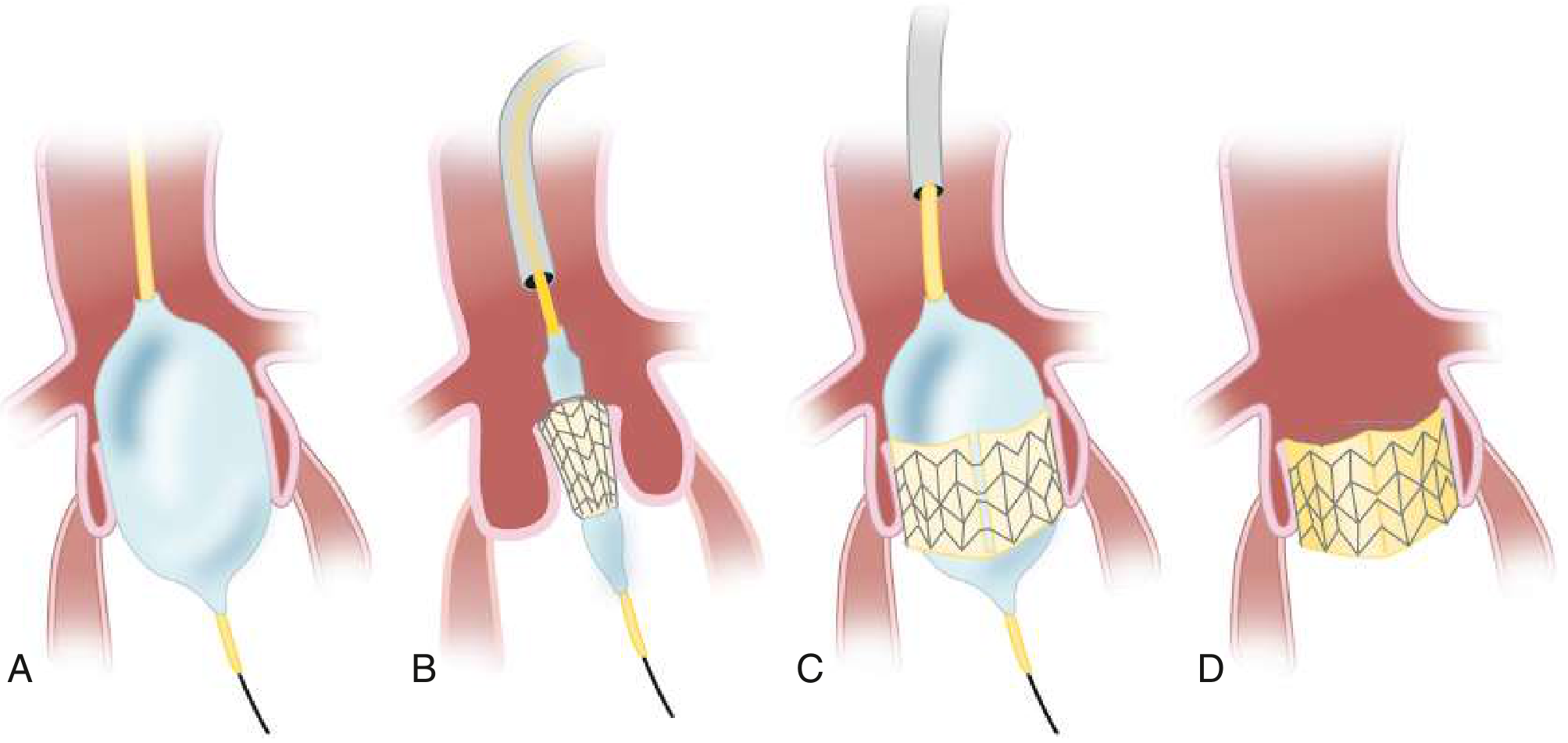
3. Step-by-Step Balloon-Expandable Valve Deployment
| Panel | Step | What's Happening |
|---|---|---|
| A | Balloon aortic valvuloplasty (BAV) | Balloon catheter inflated across the calcified native aortic valve to create space; rapid RV pacing (180 bpm) active |
| B | Valve positioning | Crimped bioprosthetic valve on balloon catheter advanced across the annulus on a guidewire; positioned straddling the annular plane |
| C | Valve deployment | Balloon inflated under rapid pacing; valve expands and locks into the native annulus, pushing aside diseased leaflets |
| D | Completion | Balloon deflated and withdrawn; new bioprosthetic valve seated in position; guidewire removed |
4. TAVI vs SAVR Decision Algorithm (AHA/ACC 2020 Guidelines)
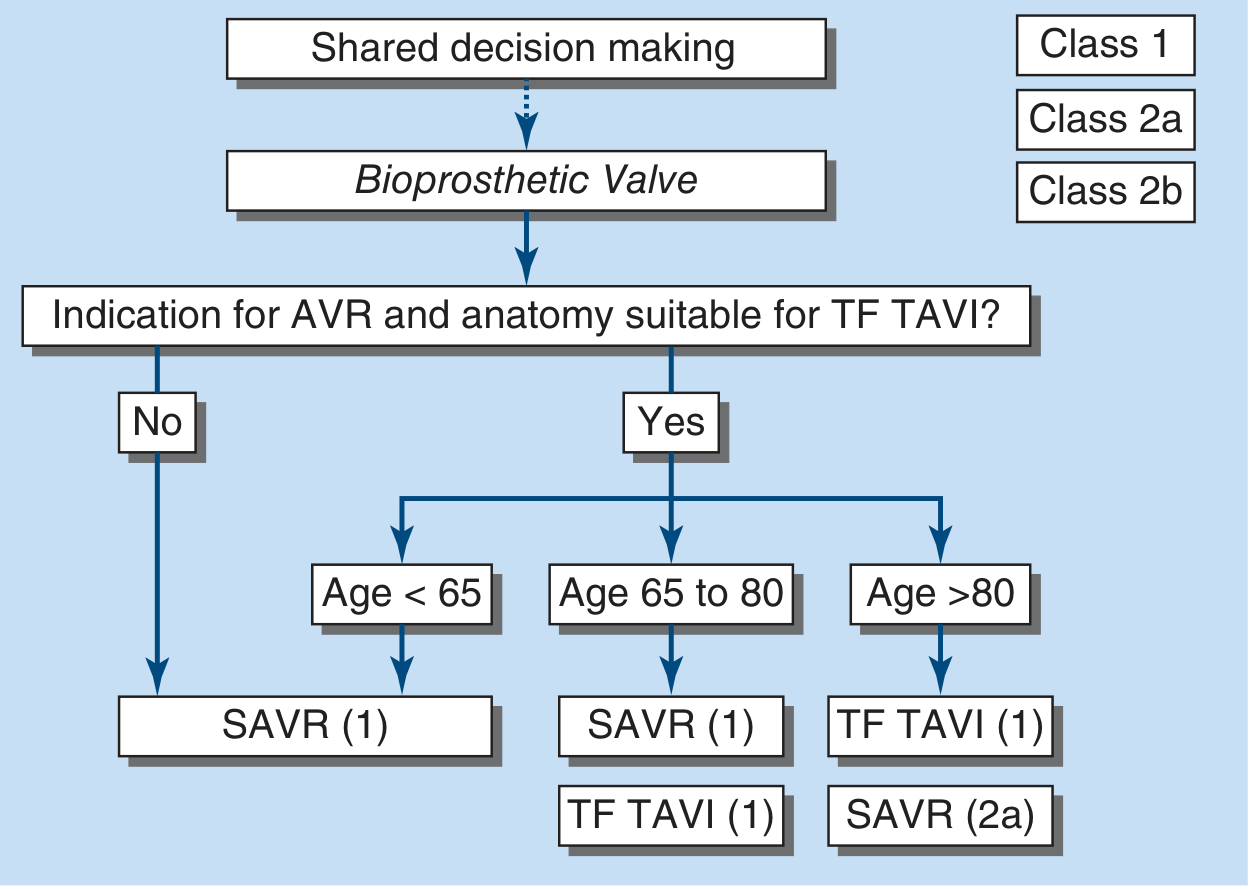
- Anatomy not suitable for transfemoral access → SAVR (Class 1) regardless of age
- Age < 65 → SAVR preferred (Class 1; limited long-term TAVI data in young patients)
- Age 65-80 → Either SAVR or TF-TAVI are both Class 1; shared decision-making
- Age > 80 → TF-TAVI preferred (Class 1); SAVR is Class 2a
5. ESC/EACTS vs AHA/ACC Guideline Comparison
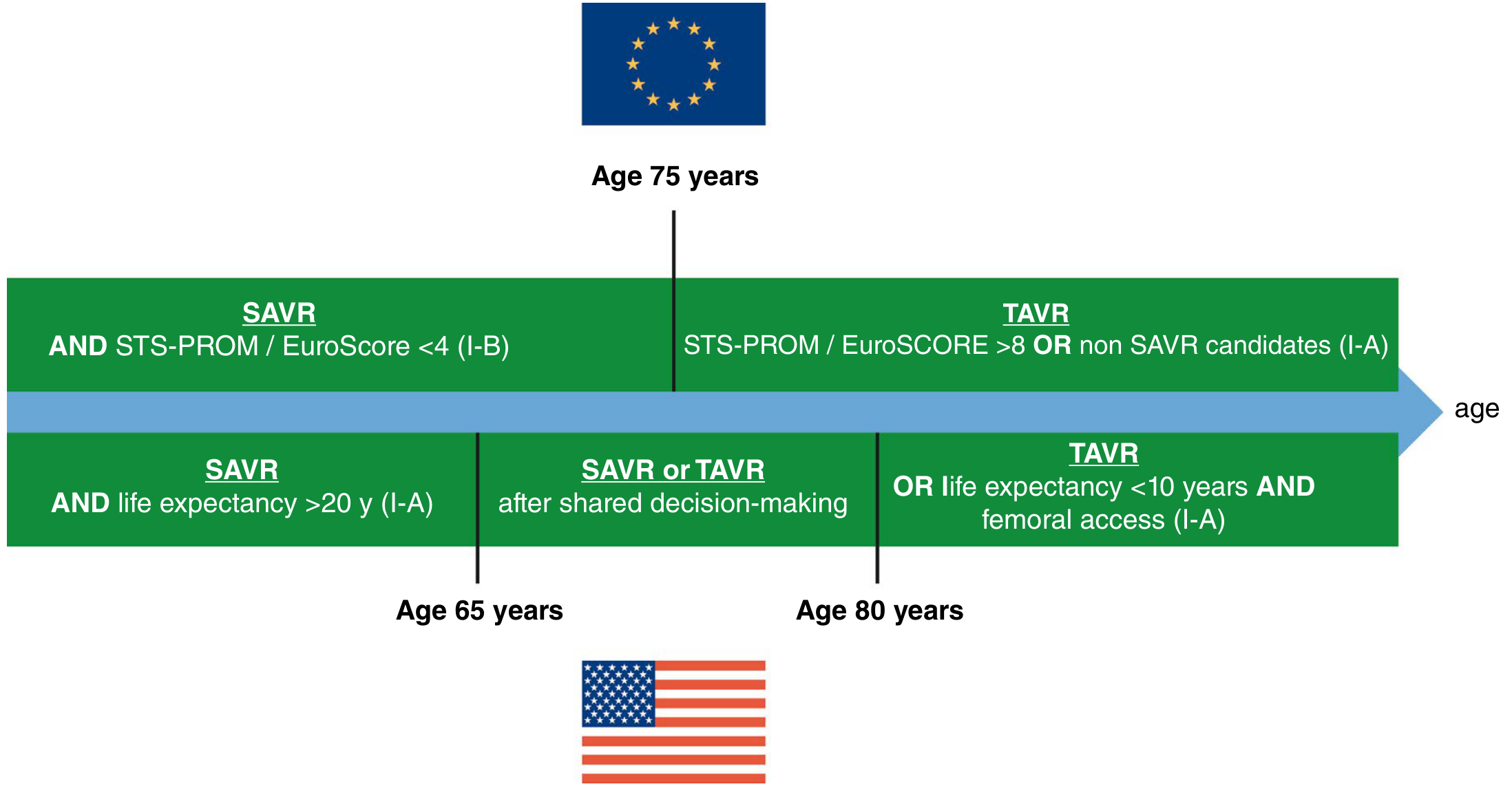
| ESC/EACTS 2021 | AHA/ACC 2020 | |
|---|---|---|
| Low-risk / young cut-off | Age < 75 + EuroSCORE < 4 → SAVR | Life expectancy > 20 yrs OR age < 65 → SAVR |
| High-risk cut-off | Age > 75 + EuroSCORE > 8 → TAVR | Age > 80 OR life expectancy < 10 yrs → TAVR |
| Middle zone | Age 65-80 shared decision | Similar grey zone |
6. Outcomes Data: SE-TAVR vs SAVR (Evolut Low Risk Trial - 4 Year Data)
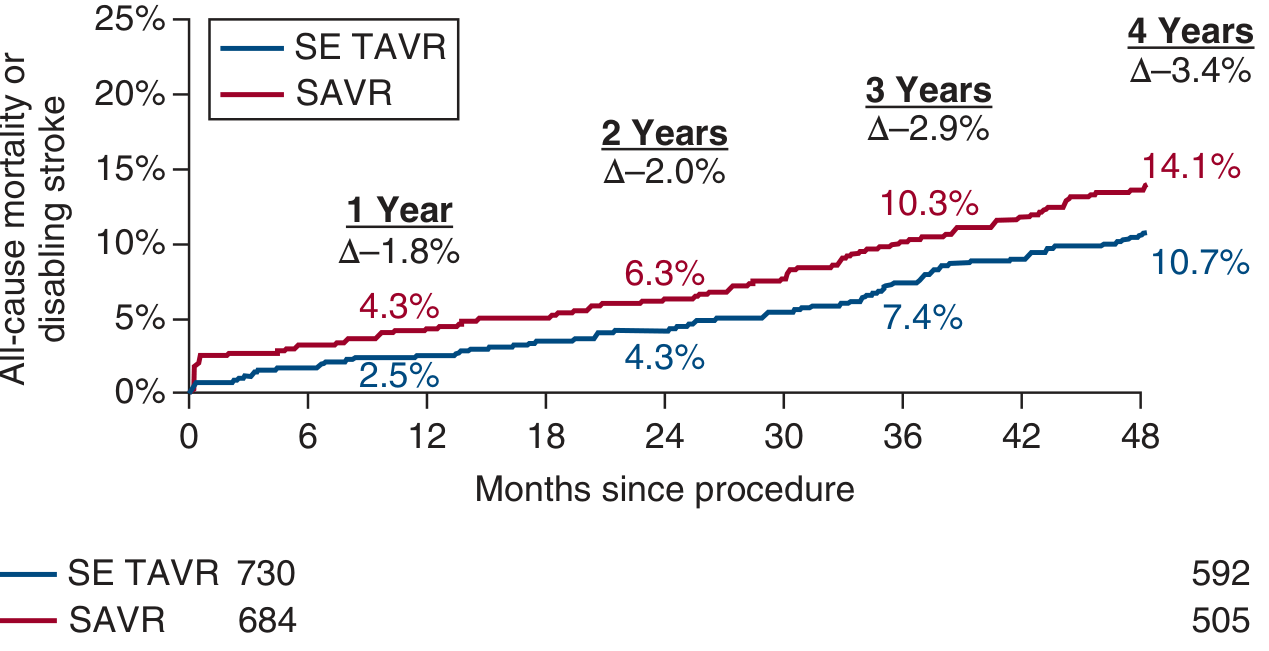
- SE-TAVR (blue) consistently lower event rate from ~6 months onward
- 4-year absolute risk reduction: 3.4% in favour of TAVR
- HR = 0.74 (95% CI 0.54-1.00), log-rank p = 0.05 - noninferior and marginally superior
- This is the Evolut Low Risk 4-year data from Forrest et al., J Am Coll Cardiol 2023
Summary of What the Images Show
| Image | Source | Clinical Value |
|---|---|---|
| BEV device (SAPIEN-type) | Harrison's 22e | Understand valve anatomy before deploying |
| SEV device (CoreValve-type) | Harrison's 22e | Understand nitinol frame, supra-annular position |
| Transapical vs Transfemoral anatomy | Sabiston Surgery | Access route selection, anatomical orientation |
| 4-step deployment sequence | Goldman-Cecil Medicine | Step-by-step procedural understanding |
| AHA/ACC decision algorithm | Harrison's 22e (AHA/ACC 2020) | Clinical decision-making |
| ESC vs AHA guideline comparison | Sabiston Surgery | International practice variation |
| Evolut LR 4-year Kaplan-Meier | Harrison's 22e (Forrest 2023) | Outcomes evidence in low-risk patients |
Create a comprehensive PDF guide combining the notes and clinical images
ls /home/daytona/workspace/ 2>/dev/null && mkdir -p /home/daytona/workspace/tavi-guide && echo "ready"
cd /home/daytona/workspace/tavi-guide && python3 -c " import urllib.request, os imgs = { 'transapical_transfemoral.png': 'https://cdn.orris.care/cdss_images/e79d76dafaec886da1a3ce29eb5fe20689fc07106a3435f44bf6c13a786f437d.png', 'deployment_steps.png': 'https://cdn.orris.care/cdss_images/1a6e8608e34391fd07a2522de81a5712b6deffc6e555667dbc7c1cd1bd35b099.png', 'bev_valve.png': 'https://cdn.orris.care/cdss_images/534e0337eae28805a6365e6c2bc2ea97b6b596357ef47b15b8e15f76c5f8fbe4.png', 'sev_valve.png': 'https://cdn.orris.care/cdss_images/fe112fcdf883a5906dacfc58383242a3584d66f8a666f36250fd3723b6171723.png', 'decision_algorithm.png': 'https://cdn.orris.care/cdss_images/859b29460b07cfcc53b3ad63eb30d8bdfb6a979f4c70f80fabd6c0d6e501c47e.png', 'guideline_comparison.png': 'https://cdn.orris.care/cdss_images/2a031a6799b61d6e59f0cf1b7ffb0eab9b5474e8dffbc0ff8d45034651b2ca97.png', 'kaplan_meier.png': 'https://cdn.orris.care/cdss_images/90c6d2dbca22c3aa94b7f85ec5d017c5dd4a66b56116294fef6a16de1bbdfe51.png', } for fname, url in imgs.items(): urllib.request.urlretrieve(url, fname) sz = os.path.getsize(fname) print(f'{fname}: {sz} bytes') print('All images downloaded') "
~/tavi-guide/build_tavi_pdf.py
"""
TAVI Comprehensive Guide - PDF Builder
Uses ReportLab for professional layout with embedded clinical images.
"""
import os
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import cm, mm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Image, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.platypus.flowables import BalancedColumns
from reportlab.graphics.shapes import Drawing, Rect, String
from reportlab.pdfbase import pdfmetrics
from reportlab.pdfbase.ttfonts import TTFont
# ── Page setup ────────────────────────────────────────────────────────────────
W, H = A4
MARGIN = 2 * cm
DOC_PATH = "/home/daytona/workspace/tavi-guide/TAVI_Comprehensive_Guide.pdf"
IMG_DIR = "/home/daytona/workspace/tavi-guide"
doc = SimpleDocTemplate(
DOC_PATH,
pagesize=A4,
leftMargin=MARGIN, rightMargin=MARGIN,
topMargin=2.2*cm, bottomMargin=2*cm,
title="TAVI Comprehensive Clinical Guide",
author="Orris Medical AI",
subject="Transcatheter Aortic Valve Implantation",
)
# ── Colour palette ─────────────────────────────────────────────────────────────
NAVY = colors.HexColor("#1a2c5b")
TEAL = colors.HexColor("#0e7490")
LIGHT_BG = colors.HexColor("#f0f7fa")
WARN_BG = colors.HexColor("#fff7ed")
WARN_BDR = colors.HexColor("#ea580c")
GREEN_BG = colors.HexColor("#f0fdf4")
GREEN_BDR = colors.HexColor("#16a34a")
RED_BG = colors.HexColor("#fef2f2")
RED_BDR = colors.HexColor("#dc2626")
MID_GREY = colors.HexColor("#64748b")
LIGHT_GREY= colors.HexColor("#e2e8f0")
WHITE = colors.white
# ── Styles ─────────────────────────────────────────────────────────────────────
base = getSampleStyleSheet()
def S(name, **kw):
p = ParagraphStyle(name, **kw)
return p
COVER_TITLE = S("CoverTitle",
fontSize=34, leading=42, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_CENTER, spaceAfter=6)
COVER_SUB = S("CoverSub",
fontSize=16, leading=22, textColor=colors.HexColor("#bfdbfe"),
fontName="Helvetica", alignment=TA_CENTER, spaceAfter=4)
COVER_NOTE = S("CoverNote",
fontSize=10, leading=14, textColor=colors.HexColor("#93c5fd"),
fontName="Helvetica", alignment=TA_CENTER)
H1 = S("H1",
fontSize=18, leading=24, textColor=WHITE,
fontName="Helvetica-Bold", spaceBefore=0, spaceAfter=6,
backColor=NAVY, leftPadding=10, rightPadding=10,
borderPadding=(6, 10, 6, 10))
H2 = S("H2",
fontSize=13, leading=18, textColor=NAVY,
fontName="Helvetica-Bold", spaceBefore=14, spaceAfter=4,
borderPadding=(4, 0, 2, 0))
H3 = S("H3",
fontSize=11, leading=15, textColor=TEAL,
fontName="Helvetica-Bold", spaceBefore=10, spaceAfter=3)
BODY = S("Body",
fontSize=9.5, leading=14, textColor=colors.HexColor("#1e293b"),
fontName="Helvetica", spaceBefore=2, spaceAfter=2,
alignment=TA_JUSTIFY)
BULLET = S("Bullet",
fontSize=9.5, leading=14, textColor=colors.HexColor("#1e293b"),
fontName="Helvetica", leftIndent=14, firstLineIndent=-10,
spaceBefore=1, spaceAfter=1)
SUB_BULLET = S("SubBullet",
fontSize=9, leading=13, textColor=colors.HexColor("#334155"),
fontName="Helvetica", leftIndent=26, firstLineIndent=-10,
spaceBefore=1, spaceAfter=1)
CAPTION = S("Caption",
fontSize=8.5, leading=12, textColor=MID_GREY,
fontName="Helvetica-Oblique", alignment=TA_CENTER,
spaceBefore=4, spaceAfter=8)
BOX_TITLE = S("BoxTitle",
fontSize=10, leading=14, textColor=WHITE,
fontName="Helvetica-Bold")
BOX_BODY = S("BoxBody",
fontSize=9, leading=13, textColor=colors.HexColor("#1e293b"),
fontName="Helvetica", spaceBefore=1, spaceAfter=1)
FOOTER_STYLE = S("Footer",
fontSize=7.5, leading=10, textColor=MID_GREY,
fontName="Helvetica", alignment=TA_CENTER)
# ── Helper builders ────────────────────────────────────────────────────────────
def section_header(text, num=None):
label = f"{num}. {text}" if num else text
return [
Spacer(1, 8),
Table(
[[Paragraph(label, H1)]],
colWidths=[W - 2*MARGIN],
style=TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("ROUNDEDCORNERS", [5]),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
])
),
Spacer(1, 6),
]
def sub_header(text):
return [Paragraph(text, H2), HRFlowable(width="100%", thickness=1.2, color=TEAL, spaceAfter=4)]
def h3(text):
return Paragraph(text, H3)
def body(text):
return Paragraph(text, BODY)
def bullet(text, level=1):
style = BULLET if level == 1 else SUB_BULLET
marker = "•" if level == 1 else "–"
return Paragraph(f"{marker} {text}", style)
def caption(text):
return Paragraph(text, CAPTION)
def spacer(h=6):
return Spacer(1, h)
def hr(color=LIGHT_GREY):
return HRFlowable(width="100%", thickness=0.5, color=color, spaceAfter=4)
def img(fname, width_cm=14, caption_text=None):
path = os.path.join(IMG_DIR, fname)
items = [Image(path, width=width_cm*cm, kind='proportional')]
if caption_text:
items.append(caption(caption_text))
return items
def info_box(title, items, bg=LIGHT_BG, border=TEAL, title_bg=TEAL):
content_rows = [[Paragraph(f"• {i}", BOX_BODY)] for i in items]
header_row = [[Paragraph(title, BOX_TITLE)]]
all_rows = header_row + content_rows
col_w = W - 2*MARGIN - 0.4*cm
t = Table(all_rows, colWidths=[col_w])
style = TableStyle([
("BACKGROUND", (0,0), (-1,0), title_bg),
("BACKGROUND", (0,1), (-1,-1), bg),
("TEXTCOLOR", (0,0), (-1,0), WHITE),
("BOX", (0,0), (-1,-1), 1, border),
("INNERGRID", (0,1), (-1,-1), 0.3, LIGHT_GREY),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("ROUNDEDCORNERS",[4]),
])
t.setStyle(style)
return [t, spacer(6)]
def two_col_table(headers, rows, col_widths=None):
page_w = W - 2*MARGIN
if not col_widths:
col_widths = [page_w/len(headers)] * len(headers)
hdr_row = [Paragraph(f"<b>{h}</b>", S("TH", fontSize=8.5, leading=12,
fontName="Helvetica-Bold", textColor=WHITE)) for h in headers]
data_rows = []
for row in rows:
data_rows.append([Paragraph(str(c), S("TD", fontSize=8.5, leading=12,
fontName="Helvetica", textColor=colors.HexColor("#1e293b")))
for c in row])
all_data = [hdr_row] + data_rows
t = Table(all_data, colWidths=col_widths)
style = TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("ROWBACKGROUNDS",(0,1), (-1,-1), [WHITE, LIGHT_BG]),
("BOX", (0,0), (-1,-1), 0.8, NAVY),
("INNERGRID", (0,0), (-1,-1), 0.3, LIGHT_GREY),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
("VALIGN", (0,0), (-1,-1), "TOP"),
])
t.setStyle(style)
return [t, spacer(8)]
# ── Page callbacks ─────────────────────────────────────────────────────────────
def on_page(canvas, doc):
canvas.saveState()
pg = doc.page
# Header bar
canvas.setFillColor(NAVY)
canvas.rect(0, H - 1.1*cm, W, 1.1*cm, fill=1, stroke=0)
canvas.setFillColor(WHITE)
canvas.setFont("Helvetica-Bold", 8)
canvas.drawString(MARGIN, H - 0.72*cm, "TAVI – Comprehensive Clinical Guide")
canvas.setFont("Helvetica", 8)
canvas.drawRightString(W - MARGIN, H - 0.72*cm, "Orris Medical AI | July 2026")
# Footer
canvas.setFillColor(LIGHT_GREY)
canvas.rect(0, 0, W, 1.3*cm, fill=1, stroke=0)
canvas.setFillColor(MID_GREY)
canvas.setFont("Helvetica", 7.5)
canvas.drawCentredString(W/2, 0.5*cm,
f"Page {pg} | Sources: Harrison's 22E, Braunwald's Heart Disease, Sabiston Surgery, Goldman-Cecil, Miller's Anesthesia, Bailey & Love")
canvas.restoreState()
def on_first_page(canvas, doc):
# Solid navy cover background
canvas.setFillColor(NAVY)
canvas.rect(0, 0, W, H, fill=1, stroke=0)
# Accent stripe
canvas.setFillColor(TEAL)
canvas.rect(0, H*0.52, W, 6, fill=1, stroke=0)
canvas.restoreState()
# ── Build story ────────────────────────────────────────────────────────────────
story = []
# ═══════════════════════════════════════════════════════════════════════════════
# COVER PAGE
# ═══════════════════════════════════════════════════════════════════════════════
def cover_page():
items = []
items.append(Spacer(1, 5.5*cm))
# Title block on navy background (already set by on_first_page)
title_data = [[
Paragraph("TAVI", S("CT", fontSize=52, leading=58, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_CENTER))
]]
title_t = Table(title_data, colWidths=[W - 2*MARGIN])
title_t.setStyle(TableStyle([("BACKGROUND",(0,0),(-1,-1),colors.transparent)]))
items.append(title_t)
items.append(spacer(6))
items.append(Paragraph("Transcatheter Aortic Valve Implantation", COVER_TITLE))
items.append(spacer(10))
items.append(Paragraph("Comprehensive Clinical Reference Guide", COVER_SUB))
items.append(spacer(6))
items.append(Paragraph("Procedure · Indications · Devices · Complications · Management", COVER_SUB))
items.append(spacer(30))
items.append(hr(colors.HexColor("#3b82f6")))
items.append(spacer(10))
items.append(Paragraph(
"Sources: Harrison's Principles of Internal Medicine 22E (2025) · Braunwald's Heart Disease · "
"Sabiston Textbook of Surgery · Goldman-Cecil Medicine · Miller's Anesthesia 10e · Bailey & Love's Surgery 28e · EuroIntervention",
COVER_NOTE))
items.append(spacer(6))
items.append(Paragraph("Compiled by Orris Medical AI · July 2026", COVER_NOTE))
items.append(PageBreak())
return items
story += cover_page()
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 1 – BACKGROUND & HISTORY
# ═══════════════════════════════════════════════════════════════════════════════
story += section_header("Background & History", 1)
story += sub_header("Origins and Evolution")
story += [
body("TAVI (also called TAVR – Transcatheter Aortic Valve Replacement) was first performed in humans by "
"<b>Alain Cribier</b> in <b>2002</b>, treating an inoperable patient with severe calcific aortic stenosis. "
"The technology has since evolved from an experimental last-resort procedure into the most commonly "
"performed aortic valve intervention in the United States."),
spacer(4),
]
story += info_box("FDA Approval Timeline", [
"2002 – First-in-human TAVI (Alain Cribier)",
"2011 – FDA approval: Prohibitive surgical risk (STS predicted 30-day mortality >50%)",
"2012 – FDA approval: High surgical risk (STS >10% or ≥2 frailty indices)",
"2016 – FDA approval: Intermediate surgical risk (STS 4%–8%); TAVI volume surpasses SAVR in USA",
"2019 – FDA approval: Low surgical risk (STS ≤4%) – PARTNER 3 & Evolut Low Risk trials",
"2025 – FDA approval for asymptomatic severe aortic stenosis (landmark regulatory expansion)",
"2025 – Medtronic Evolut systems gain expanded redo-TAVR indication",
])
story += [
body("<b>Current volume:</b> Over 70,000 TAVI procedures performed annually in the USA. "
"Over 95% use the transfemoral (TF) approach. CMS mandates a minimum of 20 procedures/year "
"per accredited TAVI centre (2023 rule)."),
spacer(6),
]
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 2 – INDICATIONS & DECISION MAKING
# ═══════════════════════════════════════════════════════════════════════════════
story += section_header("Indications & Decision-Making", 2)
story += sub_header("Severe Aortic Stenosis – Echocardiographic Definition")
story += two_col_table(
["Parameter", "Threshold for Severe AS"],
[
["Aortic valve area (AVA)", "< 1.0 cm²"],
["Mean gradient", "> 40 mmHg"],
["Peak aortic jet velocity", "> 4 m/s"],
["Indexed AVA", "< 0.6 cm²/m²"],
],
col_widths=[(W-2*MARGIN)*0.55, (W-2*MARGIN)*0.45]
)
story += sub_header("AHA/ACC 2020 Guideline Recommendations")
story += two_col_table(
["COR", "LOE", "Recommendation"],
[
["I", "A", "Age < 65 or life expectancy > 20 years → SAVR recommended"],
["I", "A", "Age 65–80, no TF contraindication → SAVR or TF-TAVI after shared decision-making"],
["I", "A", "Age > 80 or life expectancy < 10 yrs, no TF contraindication → TF-TAVI preferred over SAVR"],
["I", "A", "Any age, high/prohibitive surgical risk, predicted survival > 12 months → TAVI"],
["I", "B-NR", "Asymptomatic AS with LVEF < 50% → follow same age-stratified recommendations"],
["I", "B-NR", "Asymptomatic AS with abnormal exercise test/very severe AS/rapid progression → SAVR preferred"],
["I", "C-EO", "Predicted survival < 12 months or minimal QoL benefit → palliative care"],
["2b", "C-EO", "Critically ill with severe AS → balloon valvuloplasty as bridge to TAVI/SAVR"],
],
col_widths=[(W-2*MARGIN)*0.07, (W-2*MARGIN)*0.08, (W-2*MARGIN)*0.85]
)
story += sub_header("TAVI vs SAVR Decision Algorithm (AHA/ACC 2020)")
story += img("decision_algorithm.png", 13,
"FIGURE 1 – AHA/ACC decision flowchart. If anatomy is unsuitable for TF-TAVI → SAVR regardless of age. "
"Age <65 → SAVR (Class 1). Age 65–80 → either SAVR or TF-TAVI (both Class 1). Age >80 → TF-TAVI preferred (Class 1). "
"(Source: Harrison's Principles of Internal Medicine 22E, 2025)")
story.append(spacer(4))
story += sub_header("ESC/EACTS (Europe) vs AHA/ACC (USA) Guideline Comparison")
story += img("guideline_comparison.png", 15,
"FIGURE 2 – Side-by-side ESC/EACTS (top, 75-year cut-off) vs AHA/ACC (bottom, 65/80-year cut-offs) guidelines. "
"Europe uses EuroSCORE <4 or >8; USA uses life expectancy and age thresholds. "
"(Source: Sabiston Textbook of Surgery / Coisne et al. JACC 2023)")
story += sub_header("Special Indications")
story += [
bullet("<b>Valve-in-Valve (ViV) TAVI:</b> Failed bioprosthetic aortic valves – FDA approved 2015; sharply increasing volumes"),
bullet("<b>Porcelain aorta:</b> Heavily calcified ascending aorta precludes safe aortic cross-clamping for SAVR"),
bullet("<b>Prior chest radiation:</b> Radiation-induced fibrosis increases SAVR morbidity"),
bullet("<b>Re-sternotomy:</b> High adhesion risk makes TAVI preferable"),
bullet("<b>Bicuspid aortic valve (BAV):</b> Off-label; selected cases only – avoid if prominent calcified raphe"),
bullet("<b>Pure aortic insufficiency (AI):</b> Off-label; dedicated devices in development"),
bullet("<b>TAVI + PCI:</b> Concurrent or staged percutaneous coronary intervention in intermediate-risk patients with non-complex CAD"),
spacer(8),
]
# Contraindications box
story += sub_header("Contraindications")
row_data = [
[Paragraph("<b>Absolute</b>", S("TH2", fontSize=9, fontName="Helvetica-Bold", textColor=NAVY)),
Paragraph("<b>Relative / Access-Specific</b>", S("TH2", fontSize=9, fontName="Helvetica-Bold", textColor=NAVY))],
[Paragraph("• Expected survival < 12 months after TAVI\n• No improvement in QoL expected\n"
"• Active infective endocarditis\n• No available access route", BOX_BODY),
Paragraph("• Significant iliofemoral disease (TF)\n• Iliofemoral diameter < 5.0–5.5 mm (TF)\n"
"• LV apical thrombus (transapical)\n• Recent MI < 3 months (transapical)\n"
"• Severe pulmonary dysfunction (transapical)\n• Heavily calcified LVOT (annular rupture risk)", BOX_BODY)],
]
ct = Table(row_data, colWidths=[(W-2*MARGIN)/2]*2)
ct.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), LIGHT_BG),
("BOX", (0,0), (-1,-1), 1, RED_BDR),
("INNERGRID", (0,0), (-1,-1), 0.5, LIGHT_GREY),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("VALIGN", (0,0), (-1,-1), "TOP"),
]))
story += [ct, spacer(6)]
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 3 – VALVE DEVICES
# ═══════════════════════════════════════════════════════════════════════════════
story += [PageBreak()]
story += section_header("Valve Devices", 3)
story += sub_header("Types of Prostheses")
story += [
body("All TAVI prostheses incorporate a <b>pericardial tissue bioprosthesis</b> mounted within a metallic frame. "
"Two main categories exist, differentiated by their deployment mechanism:"),
spacer(6),
]
# Side-by-side valve image table
valve_img_table = Table([
[Image(os.path.join(IMG_DIR, "bev_valve.png"), width=7.5*cm, kind='proportional'),
Image(os.path.join(IMG_DIR, "sev_valve.png"), width=7.5*cm, kind='proportional')],
[Paragraph("Balloon-Expandable Valve (BEV)\nEdwards SAPIEN series\nB=Balloon · V=Valve · N=Nose cone", CAPTION),
Paragraph("Self-Expanding Valve (SEV)\nMedtronic CoreValve / Evolut series\nNitinol mesh frame with tissue leaflets and pericardial skirt", CAPTION)],
], colWidths=[(W-2*MARGIN)/2]*2)
valve_img_table.setStyle(TableStyle([
("ALIGN", (0,0), (-1,-1), "CENTER"),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("BOX", (0,0), (-1,-1), 0.5, LIGHT_GREY),
("INNERGRID", (0,0), (-1,-1), 0.5, LIGHT_GREY),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
]))
story += [valve_img_table,
caption("FIGURE 3 – Left: Balloon-expandable TAVI valve (Edwards SAPIEN-type) on delivery catheter. "
"Right: Self-expanding valve (CoreValve-type) showing the large nitinol mesh frame. "
"(Source: Harrison's Principles of Internal Medicine 22E, 2025)"),
spacer(8)]
story += two_col_table(
["Feature", "Balloon-Expandable (BEV)", "Self-Expanding (SEV)"],
[
["Example devices", "Edwards SAPIEN 3, SAPIEN 3 Ultra", "Medtronic CoreValve, Evolut R/PRO/FX"],
["Frame material", "Cobalt-chromium/stainless steel", "Nitinol (nickel-titanium)"],
["Deployment", "Balloon inflation under rapid pacing", "Sheath withdrawal; self-expands"],
["Position", "Intra-annular", "Supra-annular (extends into ascending aorta)"],
["Repositionable", "No (once deployed)", "Yes – Evolut R/PRO/FX can be recaptured"],
["Paravalvular leak", "Low (especially SAPIEN 3 with outer skirt)", "Slightly higher historically"],
["Pacemaker need", "Lower (~5–10%)", "Higher (~15–25% with older designs)"],
["Valve area (EOA)", "Slightly smaller (intra-annular)", "Larger (supra-annular position)"],
],
col_widths=[(W-2*MARGIN)*0.25, (W-2*MARGIN)*0.375, (W-2*MARGIN)*0.375]
)
story += sub_header("Valve Sizing Principles")
story += [
bullet("<b>CT-based annular measurement</b> is the gold standard (ECG-gated, IV contrast, <1 mm slices)"),
bullet("Annulus dimensions measured in systole; both area-derived and perimeter-derived diameters used"),
bullet("Target <b>0–20% oversizing</b> relative to annulus area"),
bullet("Under-sizing → paravalvular leak (PVL)"),
bullet("Over-sizing → annular rupture risk (especially with LVOT calcification)"),
bullet("CT also assesses: coronary heights, LVOT calcium, aortic arch, iliofemoral vessels"),
spacer(8),
]
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 4 – PREPROCEDURAL WORKUP
# ═══════════════════════════════════════════════════════════════════════════════
story += section_header("Pre-Procedural Workup & Patient Selection", 4)
story += sub_header("Multidisciplinary Heart Team")
story += [
body("A formal <b>Heart Team</b> evaluation is mandatory (AHA/ACC, ESC/EACTS, and CMS requirements). "
"Both a <b>cardiac surgeon</b> and an <b>interventional cardiologist</b> must evaluate and perform the procedure."),
bullet("Interventional cardiologist"),
bullet("Cardiac surgeon"),
bullet("Cardiac anaesthesiologist"),
bullet("Imaging specialist (echocardiography + CT)"),
bullet("Intensivist / CCU physician"),
bullet("Specialty nursing and catheter lab staff"),
spacer(6),
]
story += sub_header("Pre-Procedural Investigations")
story += two_col_table(
["Investigation", "Purpose / Key Findings"],
[
["TAVI-protocol CT angiography (ECG-gated, IV contrast, <1 mm slices)",
"Annulus sizing; LVOT/coronary anatomy; calcium distribution; iliofemoral access assessment; aortic arch pathology"],
["Transthoracic echocardiography (TTE)",
"Confirm severe AS; assess LVEF, wall motion, MR severity, other valvular disease; annular dimensions"],
["Transesophageal echocardiography (TEE)",
"Used intra-procedurally for positioning guidance and immediate post-deployment assessment"],
["Coronary angiography",
"Assess CAD severity; plan concurrent or staged PCI if needed"],
["12-lead ECG",
"Baseline conduction: QRS duration, AV block, fascicular block (pacemaker risk predictors)"],
["Frailty assessment",
"Gait speed, grip strength, ADLs, serum albumin – score >2/5 indicates high frailty"],
["Blood tests",
"FBC, U&E (renal function, contrast nephropathy risk), coagulation, Group & Save, BNP/NT-proBNP"],
["Pulmonary function tests",
"Especially relevant if transapical approach considered"],
],
col_widths=[(W-2*MARGIN)*0.38, (W-2*MARGIN)*0.62]
)
story += sub_header("TAVI vs SAVR: Key Anatomical Preference Factors")
story += two_col_table(
["Factor", "Favours TAVI", "Favours SAVR"],
[
["Age", "> 80 years", "< 65 years"],
["Life expectancy", "< 10 years", "> 20 years"],
["Surgical risk", "High/prohibitive STS", "Low STS"],
["Conduction", "Pre-existing pacemaker", "No pre-existing block"],
["Aorta", "Porcelain aorta", "Normal aorta"],
["Sternum", "Re-sternotomy required", "Virgin sternum"],
["Chest radiation", "Prior RT to chest", "No prior RT"],
["Coronary access", "Simple anatomy post-TAVI", "Complex anatomy requiring CABG"],
["Valve anatomy", "Tricuspid valve", "Bicuspid/complex anatomy"],
["Frailty", "High frailty", "Normal physiological reserve"],
],
col_widths=[(W-2*MARGIN)*0.3, (W-2*MARGIN)*0.35, (W-2*MARGIN)*0.35]
)
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 5 – ACCESS ROUTES
# ═══════════════════════════════════════════════════════════════════════════════
story += [PageBreak()]
story += section_header("Access Routes", 5)
story += img("transapical_transfemoral.png", 15,
"FIGURE 4 – Anatomical illustration comparing Transapical (left) and Transfemoral (right) TAVI access routes. "
"Transapical: device enters the LV apex via mini-thoracotomy, anterograde passage. "
"Transfemoral: retrograde delivery from the femoral artery up the aorta. "
"(Source: Sabiston Textbook of Surgery)")
story.append(spacer(4))
story += sub_header("Access Route Summary")
story += two_col_table(
["Route", "Approach", "% of TAVI (USA)", "Key Advantage", "Key Limitation"],
[
["Transfemoral (TF)", "Retrograde via CFA", "~95%", "Lowest complication rate; sedation possible", "Requires adequate iliofemoral diameter/anatomy"],
["Transaxillary / Transsubclavian", "Retrograde via subclavian/axillary a.", "~3%", "Good alternative; often used when TF fails", "Requires vessel diameter ≥6 mm; ipsilateral arm ischaemia risk"],
["Transcarotid (TC)", "Retrograde via common carotid a.", "~1%", "Direct route; minimal tortuosity", "Cerebrovascular risk; bilateral carotid stenosis contraindication"],
["Transaortic (TAo)", "Direct ascending aorta via mini-sternotomy", "<1%", "Avoids peripheral vascular access", "Requires surgical chest access"],
["Transapical (TA)", "Anterograde via LV apex (mini-thoracotomy)", "<1%", "No aortic arch crossing; useful for aortic arch disease", "Higher morbidity; requires GA; LV injury risk"],
["Transcaval", "IVC-to-aorta transcaval puncture", "Rare", "No arterial cut-down needed", "Highly specialised; aortocaval fistula risk"],
],
col_widths=[(W-2*MARGIN)*0.18, (W-2*MARGIN)*0.2, (W-2*MARGIN)*0.12, (W-2*MARGIN)*0.25, (W-2*MARGIN)*0.25]
)
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 6 – PROCEDURAL STEPS
# ═══════════════════════════════════════════════════════════════════════════════
story += section_header("Procedural Steps (Transfemoral Approach)", 6)
story += sub_header("Procedure Environment & Monitoring Setup")
story += [
bullet("<b>Setting:</b> Hybrid operating room or cardiac catheterisation lab with state-of-the-art fluoroscopy, echocardiography, and emergency CPB capability"),
bullet("<b>Required personnel:</b> Interventional cardiologist, cardiac surgeon, cardiac anaesthesiologist, scrub nurse, cath lab technician, echo cardiographer, CPB perfusionist on standby"),
bullet("<b>Monitoring:</b> Radial arterial line (continuous BP), large-bore IV ×2, external defibrillation pads"),
bullet("<b>CPB:</b> Perfusionist and cardiac surgeon must be immediately available – CPB set up and primed before procedure begins"),
bullet("<b>Anticoagulation:</b> Heparin to achieve ACT > 250–300 sec initiated after vascular access"),
spacer(6),
]
story += sub_header("Anaesthesia Options")
story += two_col_table(
["Approach", "When Used", "Monitoring", "Key Considerations"],
[
["General Anaesthesia (GA)", "Transapical; alternative access; complex cases or failed sedation",
"ETT/LMA, TEE, art line, CVP", "TEE guides positioning and assesses result; allows full rescue manoeuvres"],
["Conscious Sedation ('Minimalist')", "Uncomplicated TF-TAVI – majority of cases at modern centres",
"Art line, TTE or fluoroscopy-only guidance", "Faster recovery; earlier mobilisation; shorter stay; must plan GA bail-out"],
],
col_widths=[(W-2*MARGIN)*0.2, (W-2*MARGIN)*0.28, (W-2*MARGIN)*0.22, (W-2*MARGIN)*0.3]
)
story += sub_header("Step-by-Step Procedure")
steps = [
("Step 1 – Vascular Access",
"Percutaneous puncture of common femoral artery (CFA) under ultrasound guidance. "
"Two ProGlide pre-close sutures deployed before inserting the large sheath. "
"Contralateral femoral artery accessed for pigtail catheter. "
"Femoral vein access for temporary RV pacing wire."),
("Step 2 – Baseline Haemodynamics",
"Simultaneous LV and aortic pressure measurement. Baseline gradient documented. "
"Optimal fluoroscopic angulation determined (LAO/RAO + cranial/caudal) "
"to view aortic valve plane perpendicularly ('co-planar' view)."),
("Step 3 – Guidewire Crossing",
"Stiff guidewire (e.g. Amplatz Extra Stiff) advanced retrograde across the stenotic native aortic valve "
"using a straight or angled catheter. Guidewire tip positioned deep in the LV apex for stability. "
"Entire subsequent procedure performed over this guidewire."),
("Step 4 – Balloon Aortic Valvuloplasty (BAV)",
"Balloon catheter advanced across the native aortic valve. "
"Rapid RV pacing initiated at <b>180 beats/min</b> (reduces cardiac output, prevents balloon ejection). "
"Balloon inflated to dilate stenotic native valve and create space. Deflated; pacing stopped. "
"<i>Note: Pre-dilation is increasingly omitted with newer-generation valves (direct implantation).</i>"),
("Step 5 – Valve Crimping & Loading",
"Selected prosthetic valve crimped onto delivery system in sterile field. "
"BEV (e.g. SAPIEN 3): crimped onto balloon catheter with dedicated crimper. "
"SEV (e.g. Evolut PRO): loaded within the outer sheath of the delivery catheter. "
"Size verified; integrity confirmed."),
("Step 6 – Valve Delivery & Positioning",
"Delivery system advanced over the stiff guidewire, through the large sheath, and retrograde "
"across the native aortic valve under continuous <b>fluoroscopy + echocardiographic (TEE/TTE)</b> guidance. "
"Optimal position: prosthesis straddling annulus, ~50% below annular plane. "
"Pigtail in non-coronary cusp (NCC) used as fluoroscopic landmark. "
"Fine-tune angulation for perpendicularity to valve plane."),
("Step 7 – Valve Deployment",
"<b>BEV:</b> Rapid pacing reinitiated → balloon inflated (valve expands and locks) → balloon deflated → pacing stopped.<br/>"
"<b>SEV:</b> Outer sheath gradually withdrawn, allowing self-expansion. Pacing used at critical phases. "
"Modern SEVs (Evolut R/PRO/FX) allow <b>repositioning and recapture</b> before full deployment."),
("Step 8 – Immediate Assessment",
"<b>Aortography:</b> from contralateral pigtail – assess PVL location/severity, coronary perfusion, prosthesis position.<br/>"
"<b>TEE/TTE:</b> confirm valve function, mean gradient (target <10 mmHg), PVL degree, LV function, pericardial effusion.<br/>"
"<b>ECG:</b> watch for new LBBB, AV block.<br/>"
"If moderate-severe PVL → post-dilation with balloon inside deployed valve."),
("Step 9 – Haemostasis & Closure",
"Temporary pacing wire retained until conduction stability confirmed. "
"Arterial sheath removed; pre-close sutures deployed; fluoroscopic check of femoral site. "
"Additional manual compression, balloon tamponade, or vascular surgical repair if needed. "
"Protamine given to reverse heparin if significant bleeding."),
("Step 10 – Recovery",
"Transfer to CCU/HDU. Continuous invasive BP monitoring ≥2 hours. ECG monitoring 48–72 hours. "
"Sedation/anaesthesia reversed early ('fast-track'). Aggressive treatment of hypotension "
"(exclude tamponade/bleeding first → fluids/vasopressors). Early mobilisation."),
]
for title, desc in steps:
step_data = [[
Paragraph(f"<b>{title}</b>", S("StepT", fontSize=9.5, fontName="Helvetica-Bold",
textColor=WHITE, leading=13)),
Paragraph(desc, S("StepD", fontSize=9, fontName="Helvetica",
textColor=colors.HexColor("#1e293b"), leading=13, alignment=TA_JUSTIFY)),
]]
t = Table(step_data, colWidths=[4.5*cm, W - 2*MARGIN - 4.5*cm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (0,-1), TEAL),
("BACKGROUND", (1,0), (1,-1), LIGHT_BG),
("BOX", (0,0), (-1,-1), 0.5, TEAL),
("TOPPADDING", (0,0), (-1,-1), 7),
("BOTTOMPADDING", (0,0), (-1,-1), 7),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("VALIGN", (0,0), (-1,-1), "TOP"),
]))
story += [t, spacer(4)]
story.append(spacer(6))
story += img("deployment_steps.png", 14.5,
"FIGURE 5 – Four-step BEV deployment sequence: A) Balloon dilation of native stenotic valve (BAV). "
"B) Crimped stented valve inserted over guidewire into aortic annulus. C) Balloon inflation deploys the prosthesis. "
"D) Balloon deflated and removed; new bioprosthetic valve seated in position. "
"(Source: Goldman-Cecil Medicine, International Edition)")
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 7 – COMPLICATIONS
# ═══════════════════════════════════════════════════════════════════════════════
story += [PageBreak()]
story += section_header("Complications – Classification & Management", 7)
story += sub_header("Complication Overview")
story += two_col_table(
["Complication", "Incidence", "Key Prevention", "First-Line Management"],
[
["Vascular access injury", "10–15% (all grades)", "CT planning, closure device technique", "Balloon tamponade, covered stent, surgery"],
["Stroke", "2–3% clinical", "De-airing, ACT >250–300 sec, embolic protection device", "Neuro consult, thrombolysis/thrombectomy"],
["Paravalvular leak (mod-severe)", "<5% (new-gen valves)", "Accurate CT sizing, optimal positioning", "Post-dilation, valve-in-valve"],
["Permanent pacemaker", "~10.8% (all-comers)", "ECG screening pre-op, valve depth control", "Temporary pacing wire → PPM if persistent CHB"],
["Coronary obstruction", "~0.7–1.0%", "CT coronary height measurement, BASILICA, chimney stent", "Emergency PCI; surgery if not re-openable"],
["Annular rupture", "0.5–1%", "Avoid oversizing; screen LVOT calcium", "CPB + emergency surgical repair"],
["Valve embolisation", "Rare (<1%)", "Correct sizing, adequate pacing, operator experience", "Snare retrieval; emergency surgery"],
["Cardiac tamponade", "~1–2%", "Careful wire/pacing lead handling", "Pericardiocentesis; CPB if annular tear"],
["Leaflet thrombosis (clinical)", "~0.5%", "Post-TAVI anticoagulation protocol", "Anticoagulation (warfarin/NOAC)"],
["Acute kidney injury", "~5% (mild)", "IV hydration, minimise contrast", "Supportive; dialysis if needed (<0.5%)"],
["Infective endocarditis", "<1% late", "Antibiotic prophylaxis; aseptic technique", "Prolonged IV antibiotics; surgery in selected cases"],
],
col_widths=[(W-2*MARGIN)*0.22, (W-2*MARGIN)*0.13, (W-2*MARGIN)*0.33, (W-2*MARGIN)*0.32]
)
story += sub_header("Vascular Complications – Detailed Management")
story += [
h3("Access Site Haemorrhage"),
bullet("<b>Minor:</b> Prolonged manual compression; balloon tamponade from inside the vessel"),
bullet("<b>Major (arterial rupture):</b>"),
bullet("1. Immediate recognition (sudden BP drop, groin haematoma expansion)", 2),
bullet("2. Emergency aortography from contralateral femoral access", 2),
bullet("3. Introduce soft aortic occlusion balloon – inflate at low pressure to control bleeding", 2),
bullet("4. Administer protamine to reverse heparin", 2),
bullet("5. Balloon inflation for 10 minutes often seals small tears", 2),
bullet("6. Large tears → covered stent deployment (e.g. covered Viabahn/BeGraft) or surgical repair", 2),
bullet("7. If haemorrhage is uncontrollable → abort procedure, achieve haemostasis, reschedule", 2),
spacer(4),
h3("Retroperitoneal Haematoma"),
bullet("Presents with ipsilateral flank/back pain, falling Hb, haemodynamic compromise"),
bullet("CT abdomen/pelvis for diagnosis; conservative management if stable; covered stent or surgical exploration if expanding"),
spacer(8),
]
story += sub_header("Stroke – Detailed Management")
story += [
body("<b>Incidence:</b> 2–3% clinical stroke; subclinical MRI lesions present in up to 80% (silent emboli)."),
bullet("<b>Mechanism:</b> Calcium debris, air emboli, thrombus dislodged during catheter manipulation in aortic arch"),
bullet("<b>Risk factors:</b> Heavy aortic arch calcification, atrial fibrillation, prior stroke, heavy native valve calcium"),
h3("Prevention"),
bullet("Maintain ACT > 250–300 sec throughout procedure"),
bullet("Meticulous de-airing of all catheters and delivery systems"),
bullet("Minimise catheter manipulations within the aortic arch"),
bullet("<b>Sentinel Cerebral Protection Device</b> (Claret Medical): dual filters in brachiocephalic and left carotid arteries – captures emboli during TAVI; updated meta-analysis (Braite et al., Catheter Cardiovasc Interv 2025, PMID 41121677) supports use in high-risk cases"),
h3("Management of Acute Stroke Post-TAVI"),
bullet("Immediate neurological assessment; NIHSS scoring"),
bullet("Urgent non-contrast CT head (exclude haemorrhage)"),
bullet("Activate acute stroke pathway; neurology consultation"),
bullet("Consider thrombolysis (IV alteplase) or mechanical thrombectomy depending on CT findings and time window"),
bullet("Antiplatelet/anticoagulation adjustments per neurologist guidance"),
spacer(6),
]
story += sub_header("Paravalvular Regurgitation (PVL)")
story += [
body("<b>Mechanism:</b> Incomplete apposition of prosthesis to native annulus due to calcification, "
"under-sizing, or malpositioning. Eccentric calcium prevents full frame expansion."),
bullet("Mild PVL: clinically acceptable; monitor with serial echocardiography"),
bullet("Moderate-severe PVL: associated with increased late mortality; intervention required"),
h3("Intraoperative Management of Significant PVL"),
bullet("1. Precisely localise: TEE (multiple views) + aortography – determine circumferential vs localised"),
bullet("2. <b>Post-dilation:</b> Inflate balloon inside deployed valve (risk: worsening conduction, annular injury)"),
bullet("3. <b>Valve-in-valve implantation:</b> Second TAVI valve deployed inside first if position correctable"),
bullet("4. Surgical conversion in extreme cases"),
spacer(6),
]
story += sub_header("Conduction Disturbances & Pacemaker")
story += [
bullet("<b>New LBBB:</b> Most common finding; 30–60% with SEV, lower with BEV"),
bullet("<b>Complete Heart Block (CHB):</b> Most serious; 15–25% with SEV, 5–10% with BEV"),
h3("Predictors of Pacemaker Requirement"),
bullet("Pre-existing RBBB (highest risk)"),
bullet("QRS > 120 ms pre-procedure"),
bullet("Any degree of AV block pre-procedure"),
bullet("Deep valve implantation depth (more sub-annular)"),
bullet("Heavy membranous septum calcification"),
h3("Management"),
bullet("Keep temporary pacing wire until conduction stability confirmed (48–72 hours post-procedure)"),
bullet("ECG monitoring for minimum 48–72 hours"),
bullet("Permanent pacemaker (PPM) if: CHB persists, symptomatic high-degree AV block, new LBBB + PR prolongation"),
bullet("GLUCO-TAVI randomised trial (EuroIntervention 2026): investigating peri-procedural glucocorticoids to reduce PPM rates"),
spacer(6),
]
story += sub_header("Coronary Obstruction")
story += [
body("<b>Incidence:</b> ~0.7–1.0% (higher in valve-in-valve TAVI). Presents with sudden ST elevation and "
"haemodynamic collapse immediately after deployment."),
bullet("<b>Mechanism:</b> Native valve leaflet or prosthesis frame displaces/occludes coronary ostium"),
bullet("<b>Risk factors:</b> Coronary ostia height < 10–12 mm above annulus; heavy leaflet calcification; female sex (shorter coronary heights); ViV procedures"),
h3("Prevention Strategies"),
bullet("CT pre-planning: measure sinus of Valsalva dimensions and coronary ostial heights"),
bullet("<b>BASILICA technique:</b> Electrosurgical laceration of native leaflet before TAVI to prevent leaflet-induced obstruction"),
bullet("<b>Chimney stent ('coronary snorkelling'):</b> Pre-position coronary guidewire/balloon/stent as rescue standby"),
h3("Management"),
bullet("Immediately wire affected coronary artery (pre-positioned wire allows instant access)"),
bullet("Balloon angioplasty ± stenting via chimney technique"),
bullet("If not re-openable percutaneously → emergency CPB and surgical coronary revascularisation"),
spacer(6),
]
story += sub_header("Annular Rupture")
story += [
body("<b>Incidence:</b> 0.5–1%; <b>Mortality: very high</b> – most catastrophic intraprocedural complication."),
bullet("<b>Mechanism:</b> Oversized valve fractures the annular/LVOT complex, particularly with heavy calcification"),
bullet("<b>Presentation:</b> Sudden haemodynamic collapse during or immediately after deployment; haemopericardium/haemothorax on imaging"),
h3("Management (time-critical)"),
bullet("1. Immediate recognition – sudden, profound haemodynamic collapse"),
bullet("2. Emergency pericardiocentesis if tamponade"),
bullet("3. Initiate CPB immediately"),
bullet("4. Emergency surgical repair – may require full aortic root surgery or Bentall procedure"),
bullet("5. Preventive: careful CT sizing, avoid oversizing, avoid TAVI if severe LVOT calcification with small annulus"),
spacer(6),
]
story += sub_header("Leaflet Thrombosis")
story += [
bullet("Subclinical HALT (Hypo-Attenuating Leaflet Thickening) on CT: ~10–15% at 30–90 days"),
bullet("Clinical leaflet thrombosis: ~0.5% – associated with stroke and elevated gradients on follow-up echo"),
bullet("Higher rates than SAVR (different haemodynamic environment, absence of native leaflets)"),
bullet("<b>Management:</b> Anticoagulation (warfarin target INR 2–3, or DOAC) – usually resolves thrombus within weeks"),
bullet("Monitor with CT or echo at follow-up; no intervention needed if responding to anticoagulation"),
spacer(8),
]
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 8 – OUTCOMES DATA
# ═══════════════════════════════════════════════════════════════════════════════
story += [PageBreak()]
story += section_header("Outcomes Data & Trial Evidence", 8)
story += sub_header("STS/ACC TVT Registry Benchmarks (All-Comers, All Risk Profiles)")
story += two_col_table(
["Outcome Parameter", "Rate"],
[
["30-day mortality", "~2.6%"],
["30-day stroke", "~2.3%"],
["Permanent pacemaker at 30 days", "~10.8%"],
["New-onset dialysis", "< 0.5%"],
["Overall procedural success", "> 95%"],
["1-year mortality reduction (vs medical Rx in high-risk)", "51% → 31% (45% relative reduction)"],
],
col_widths=[(W-2*MARGIN)*0.65, (W-2*MARGIN)*0.35]
)
story += sub_header("Landmark Clinical Trials")
story += two_col_table(
["Trial", "Population", "Key Result"],
[
["PARTNER 1A", "High surgical risk", "TAVI non-inferior to SAVR at 1 year; landmark trial establishing TAVI"],
["PARTNER 1B", "Inoperable patients", "TAVI superior to standard Rx (balloon valvuloplasty); 20% absolute mortality reduction at 1 year"],
["PARTNER 2", "Intermediate risk", "TAVI non-inferior to SAVR; similar 2-year outcomes"],
["PARTNER 3", "Low risk (avg STS 1.9%)", "TAVI superior to SAVR at 1 year: composite death/stroke/rehospitalisation (8.5% vs 15.1%)"],
["Evolut Low Risk", "Low risk (SEV)", "TAVI non-inferior to SAVR at 24 months for composite death/disabling stroke"],
["Evolut Low Risk – 4yr (Forrest 2023)", "Low risk (SEV)", "HR 0.74 (95% CI 0.54–1.00) SE-TAVR vs SAVR; absolute risk reduction 3.4% at 4 years"],
["NOTION", "All-comers", "TAVI non-inferior to SAVR in all-comers (not just high risk)"],
],
col_widths=[(W-2*MARGIN)*0.22, (W-2*MARGIN)*0.25, (W-2*MARGIN)*0.53]
)
story += sub_header("Evolut Low Risk Trial – 4-Year Kaplan-Meier (SE-TAVR vs SAVR)")
story += img("kaplan_meier.png", 14,
"FIGURE 6 – Cumulative incidence of all-cause mortality or disabling stroke: SE-TAVR (blue, n=730) vs SAVR (red, n=684) "
"in low surgical risk patients. SE-TAVR shows consistently lower event rates from ~6 months onward. "
"4-year absolute risk reduction: 3.4% (10.7% vs 14.1%). HR=0.74 (95% CI 0.54–1.00), log-rank p=0.05. "
"(Source: Forrest et al. J Am Coll Cardiol 2023; reproduced in Harrison's 22E, 2025)")
story += sub_header("TAVI vs SAVR: Head-to-Head Comparison")
story += two_col_table(
["Feature", "TAVI", "SAVR"],
[
["Approach", "Minimally invasive / percutaneous", "Open heart surgery with cardiopulmonary bypass"],
["Periprocedural stroke", "Lower (transfemoral)", "Higher (aortic manipulation, CPB)"],
["Pacemaker requirement", "Higher (5–25%)", "Lower (1–3%)"],
["Paravalvular leak", "Higher (though much lower new-gen)", "Rare"],
["Leaflet thrombosis", "Higher", "Lower"],
["Periprocedural AF", "Lower", "Higher"],
["Major bleeding", "Lower", "Higher"],
["Hospital stay", "Significantly shorter (1–3 days)", "5–7 days"],
["Return to activity", "Faster (days to weeks)", "Weeks to months"],
["Long-term durability", "Promising at 5–10 yrs; under study", "Well established (20+ yr data)"],
["Preferred age", "Age > 65–80 (especially > 80)", "Age < 65 / life expectancy > 20 yrs"],
["Re-intervention options", "Redo TAVI (ViV) or TAVI explant", "Redo SAVR or TAVI"],
],
col_widths=[(W-2*MARGIN)*0.3, (W-2*MARGIN)*0.35, (W-2*MARGIN)*0.35]
)
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 9 – POST-PROCEDURAL MANAGEMENT
# ═══════════════════════════════════════════════════════════════════════════════
story += [PageBreak()]
story += section_header("Post-Procedural Management", 9)
story += sub_header("Immediate Post-Procedure Care (First 24–72 Hours)")
story += [
bullet("<b>Setting:</b> CCU or monitored HDU"),
bullet("<b>Continuous ECG monitoring</b> for minimum 48–72 hours (conduction disturbance, new CHB)"),
bullet("<b>Invasive BP monitoring</b> ≥ 2 hours post-procedure; watch for hypotension"),
bullet("<b>Hypotension protocol:</b> First exclude tamponade and access-site bleeding → then IV fluids/vasopressors"),
bullet("<b>Blood gas monitoring:</b> K⁺ level (pacing threshold affected by hypokalaemia), oxygenation"),
bullet("Temporary pacing wire: retain until conduction stability confirmed; test threshold daily"),
bullet("<b>Echocardiogram</b> at 24–48 hours: gradient, PVL, LV function, effusion"),
bullet("<b>Early mobilisation:</b> most TF-TAVI patients ambulant day 1–2"),
spacer(6),
]
story += sub_header("Antithrombotic Therapy Post-TAVI")
story += two_col_table(
["Clinical Scenario", "Recommended Regimen", "Duration"],
[
["No indication for anticoagulation (standard)", "Aspirin 75–100 mg monotherapy", "3 months, then lifelong aspirin"],
["DAPT (aspirin + clopidogrel)", "No longer preferred over aspirin monotherapy – similar outcomes with more bleeding (POPULAR-TAVI trial)", "Avoid routine use"],
["AF or other anticoagulation indication", "Therapeutic anticoagulation (NOAC preferred over warfarin); aspirin can be added", "Indefinite"],
["Leaflet thrombosis (HALT)", "Anticoagulation (warfarin INR 2–3 or DOAC)", "Until resolution on CT/echo (usually 3–6 months)"],
["Valve-in-Valve TAVI", "Anticoagulation for 3 months (higher thrombosis risk)", "3 months minimum"],
],
col_widths=[(W-2*MARGIN)*0.3, (W-2*MARGIN)*0.45, (W-2*MARGIN)*0.25]
)
story += sub_header("Follow-Up Schedule")
story += two_col_table(
["Timepoint", "Assessment"],
[
["Discharge", "Clinical review; ECG; TTE (gradient, PVL, LVEF, pericardial effusion)"],
["30 days", "Clinical review; ECG; TTE; access site check; renal function"],
["3 months", "Review antithrombotic therapy; TTE; ECG"],
["6 months", "TTE (structural valve deterioration screening); clinical review"],
["12 months (and annually thereafter)", "TTE – gradients, leaflet morphology (HALT), PVL, LV remodelling; ECG; clinical review"],
["If elevated gradients on echo", "Consider CT to evaluate HALT vs structural deterioration; review anticoagulation"],
],
col_widths=[(W-2*MARGIN)*0.25, (W-2*MARGIN)*0.75]
)
story += sub_header("Endocarditis Prophylaxis")
story += [
body("Bioprosthetic valve in aortic position – standard antibiotic prophylaxis recommended for all dental "
"procedures and at-risk interventions as per current AHA/ESC infective endocarditis guidelines. "
"High-risk pathogens post-TAVI include <i>Staphylococcus aureus</i>, <i>Enterococcus spp.</i>, and <i>Streptococcus viridans</i>."),
spacer(8),
]
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 10 – SPECIAL TOPICS
# ═══════════════════════════════════════════════════════════════════════════════
story += section_header("Special Topics & Future Directions", 10)
story += sub_header("Valve-in-Valve (ViV) TAVI")
story += [
bullet("FDA approved 2015 for degenerated bioprosthetic aortic valves"),
bullet("Sharply increasing volumes as first-generation TAVI valves approach structural deterioration"),
bullet("<b>Key challenges:</b> Smaller effective orifice area (PPM risk); higher coronary obstruction risk; higher leaflet thrombosis"),
bullet("BASILICA technique routinely considered in ViV procedures to prevent coronary obstruction"),
bullet("Meta-analysis (Comentale et al. J Cardiovasc Med 2025, PMID 39976067, >20,000 patients): TAVI-in-failed-bioprosthesis comparable to redo surgery"),
bullet("Redo TAVI (TAVI-in-TAVI) complications: valve embolisation, annular rupture, conversion to open surgery are rare; PPM rate <10%"),
bullet("TAVI explant surgery increasingly discussed for younger patients requiring re-intervention"),
spacer(6),
]
story += sub_header("TAVI in Bicuspid Aortic Valve (BAV)")
story += [
bullet("Excluded from landmark RCTs – off-label use"),
bullet("Challenges: asymmetric calcification, eccentric opening, calcified raphe → eccentric/underexpanded prosthesis"),
bullet("Higher risk of PVL, annular rupture, and pacemaker requirement"),
bullet("Reserve for patients unsuitable for SAVR; avoid if prominent calcified raphe and excessive leaflet calcium"),
spacer(6),
]
story += sub_header("Asymptomatic Severe Aortic Stenosis")
story += [
bullet("FDA approved TAVI for asymptomatic severe AS in 2025 (landmark regulatory expansion)"),
bullet("Randomised trial data expected ~2024–2025 (RECOVERY-2, AVATAR, EVOLVED trials)"),
bullet("Traditional management: watchful waiting until symptoms develop"),
spacer(6),
]
story += sub_header("TAVI and Coronary Interventions")
story += [
bullet("PCI timing: staged pre-TAVI PCI for significant CAD is most common approach"),
bullet("Concomitant PCI + TAVI: feasible in same session for simple lesions"),
bullet("Post-TAVI coronary access can be challenging, especially with SEV supra-annular valves (Evolut)"),
bullet("Left main cannulation success: ~77% for Evolut R/PRO; ~100% for BEV (SAPIEN) – due to intra-annular position"),
bullet("Commissure alignment systems developed to improve coronary access post-SEV"),
bullet("EuroIntervention 2026 State-of-the-Art: technical considerations and clinical scenarios for TAVI + coronary interventions"),
spacer(6),
]
story += sub_header("Embolic Protection Devices (EPD)")
story += [
bullet("Sentinel Cerebral Protection System (Claret Medical): dual filters capture emboli from brachiocephalic + left carotid arteries"),
bullet("Brain lesions on MRI commonly seen post-TAVI (silent emboli) even without clinical stroke"),
bullet("Updated meta-analysis (Braite et al. Catheter Cardiovasc Interv 2025, PMID 41121677): EPD reduces stroke/lesion burden, particularly in high-risk neurological anatomy"),
bullet("Not yet universally adopted; consideration especially in patients with prior stroke, heavy aortic arch calcium"),
spacer(6),
]
story += sub_header("Pacemaker Reduction Strategies")
story += [
bullet("GLUCO-TAVI randomised trial (EuroIntervention, May 2026): investigating whether peri-procedural glucocorticoids reduce PPM requirement – results awaited"),
bullet("High implant techniques (more supra-annular positioning) reduce pacemaker rates with SEV"),
bullet("Cusp overlap technique on fluoroscopy reduces SEV depth and PPM rates"),
spacer(6),
]
story += sub_header("Pure Aortic Insufficiency (AI)")
story += [
bullet("Challenging: no calcification to anchor the valve → higher embolisation risk"),
bullet("Off-label use of existing valves; dedicated devices (e.g. JenaValve, Tendyne) in development/use in selected centres"),
bullet("Higher technical difficulty; reserved for high/prohibitive surgical risk patients"),
spacer(8),
]
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 11 – QUICK REFERENCE
# ═══════════════════════════════════════════════════════════════════════════════
story += [PageBreak()]
story += section_header("Quick Reference Summary", 11)
story += sub_header("Key Numbers to Remember")
story += two_col_table(
["Parameter", "Value"],
[
["Severe AS: valve area", "< 1.0 cm²"],
["Severe AS: mean gradient", "> 40 mmHg"],
["Severe AS: peak jet velocity", "> 4 m/s"],
["Symptomatic AS 1-year mortality (untreated)", "~50%"],
["TAVI procedural success rate", "> 95%"],
["30-day mortality (TVT registry)", "~2.6%"],
["30-day stroke", "~2.3%"],
["Pacemaker rate (all-comers)", "~10.8%"],
["New-onset dialysis", "< 0.5%"],
["Annual TAVI volume (USA)", "> 70,000/year"],
["Minimum centre volume (CMS)", "20 procedures/year"],
["Rapid pacing rate during deployment", "180 beats/min"],
["Target ACT during TAVI", "> 250–300 seconds"],
["Coronary height threshold (obstruction risk)", "< 10–12 mm from annular plane"],
["Valvuloplasty balloon inflation time", "< 5–10 seconds (minimise ischaemia)"],
["PPM threshold (coronary ostia – TAVI planning)", "Minimum ~5.0–5.5 mm iliofemoral diameter for TF access"],
],
col_widths=[(W-2*MARGIN)*0.6, (W-2*MARGIN)*0.4]
)
story += sub_header("Mnemonics & Memory Aids")
story += [
h3("TAVI Complications – 'PAVE-CS'"),
bullet("<b>P</b> – Paravalvular leak"),
bullet("<b>A</b> – AV conduction block / Pacemaker"),
bullet("<b>V</b> – Vascular access complications"),
bullet("<b>E</b> – Embolic stroke"),
bullet("<b>C</b> – Coronary obstruction"),
bullet("<b>S</b> – Structural complications (annular rupture, valve embolisation, tamponade)"),
spacer(8),
h3("Annular Rupture Risk Factors – 'COSOH'"),
bullet("<b>C</b> – Calcification of LVOT (heavy)"),
bullet("<b>O</b> – Oversizing (valve too large for annulus)"),
bullet("<b>S</b> – Small annulus"),
bullet("<b>O</b> – Operator selection error"),
bullet("<b>H</b> – Heavy post-dilation after initial deployment"),
spacer(8),
]
story += sub_header("References")
refs = [
"Harrison's Principles of Internal Medicine, 22nd Edition (2025). McGraw Hill Medical.",
"Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 2-Vol Set. Elsevier.",
"Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. Elsevier.",
"Goldman-Cecil Medicine, International Edition, 2-Volume Set. Elsevier.",
"Miller's Anesthesia, 2-Volume Set, 10th Edition. Elsevier.",
"Bailey and Love's Short Practice of Surgery, 28th Edition. CRC Press.",
"Otto CM et al. 2020 AHA/ACC Guideline for Management of Patients with Valvular Heart Disease. J Am Coll Cardiol. 2021;77:e25–e197.",
"Forrest JK et al. 4-Year Outcomes of Patients with Aortic Stenosis in the EVOLUT Low Risk Trial. J Am Coll Cardiol. 2023;82:2163.",
"Coisne A, Lancellotti P et al. ACC/AHA and ESC/EACTS Guidelines for Valvular Heart Diseases: JACC Guideline Comparison. JACC. 2023;82(8):721–734.",
"Zou Q, Wei Z, Sun S. Complications in TAVR: A Comprehensive Analysis and Management Strategies. Curr Probl Cardiol. 2024 (PMID 38437930).",
"Braite M et al. Sentinel Cerebral Protection System in TAVI: Updated Meta-Analysis. Catheter Cardiovasc Interv. 2025 (PMID 41121677).",
"Comentale G et al. TAVI vs surgery for failed bioprosthesis: meta-analysis of >20,000 patients. J Cardiovasc Med. 2025 (PMID 39976067).",
"Theofilis P et al. Invasive vs conservative management in IE after TAVI: systematic review. Curr Probl Cardiol. 2026 (PMID 41529748).",
"Dalby M et al. Complications of transcatheter aortic valve implantation: avoidance and management. EuroIntervention.",
"Lee GS, Tang G et al. The current state of redo TAVR and limitations. Ann Cardiothorac Surg. 2025;14(2):98–111.",
"Aquino Bruno H et al. TAVI and coronary interventions: indications, technical considerations, and clinical scenarios. EuroIntervention. 2026.",
"Fuertes-Kenneally L et al. GLUCO-TAVI randomised trial. EuroIntervention. 2026.",
"J Clin Med 2025;14(5):1651 – Access options for transcatheter aortic valve replacement.",
]
for i, r in enumerate(refs, 1):
story.append(Paragraph(f"{i}. {r}", S("Ref", fontSize=8, leading=12,
fontName="Helvetica", textColor=MID_GREY, spaceAfter=2, leftIndent=14, firstLineIndent=-14)))
story.append(spacer(12))
story.append(hr(TEAL))
story.append(Paragraph(
"This guide was compiled by Orris Medical AI from peer-reviewed textbooks and clinical literature. "
"It is intended as an educational reference only and does not replace clinical judgement, "
"local protocols, or direct patient assessment. Always verify drug dosages and management decisions "
"against current guidelines and institutional standards.",
S("Disclaimer", fontSize=7.5, leading=11, textColor=MID_GREY,
fontName="Helvetica-Oblique", alignment=TA_CENTER, spaceBefore=6)
))
# ── Build ──────────────────────────────────────────────────────────────────────
doc.build(story, onFirstPage=on_first_page, onLaterPages=on_page)
print(f"PDF built: {DOC_PATH}")
cd /home/daytona/workspace/tavi-guide && python3 build_tavi_pdf.py 2>&1
~/tavi-guide/build_tavi_pdf.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/tavi-guide/build_tavi_pdf.py'
cd /home/daytona/workspace/tavi-guide && python3 build_tavi_pdf.py 2>&1
~/tavi-guide/build_tavi_pdf.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/tavi-guide/build_tavi_pdf.py'
~/tavi-guide/build_tavi_pdf.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/tavi-guide/build_tavi_pdf.py'
cd /home/daytona/workspace/tavi-guide && python3 build_tavi_pdf.py 2>&1
cd /home/daytona/workspace/tavi-guide && python3 -c " from pypdf import PdfReader r = PdfReader('TAVI_Comprehensive_Guide.pdf') print(f'Pages: {len(r.pages)}') print(f'File size: {__import__(\"os\").path.getsize(\"TAVI_Comprehensive_Guide.pdf\") / 1024:.1f} KB') print(f'Title: {r.metadata.title}') print(f'Author: {r.metadata.author}') "
TAVI Comprehensive Guide
PDF Document · PDF
| Section | Content |
|---|---|
| Cover page | Navy/teal professional cover with full title and source attribution |
| 1. Background & History | FDA approval timeline from 2002 → 2025; volume statistics |
| 2. Indications & Decision-Making | AHA/ACC 2020 + ESC/EACTS guidelines; decision algorithm diagram; SAVR vs TAVI selection table; contraindications |
| 3. Valve Devices | Side-by-side BEV vs SEV device photos (from Harrison's 22E); feature comparison table; valve sizing principles |
| 4. Pre-Procedural Workup | Heart team composition; all investigations; TAVI vs SAVR anatomical preference factors |
| 5. Access Routes | Transapical vs Transfemoral anatomy diagram; all 6 routes compared in table |
| 6. Procedural Steps | All 10 steps in colour-coded step blocks; 4-step deployment diagram (Goldman-Cecil) |
| 7. Complications | Master complication table; detailed management of vascular injury, stroke, PVL, pacemaker, coronary obstruction, annular rupture, tamponade, leaflet thrombosis |
| 8. Outcomes Data | TVT Registry benchmarks; all landmark trials (PARTNER 1/2/3, Evolut LR); Kaplan-Meier curve (Evolut 4-year data) |
| 9. Post-Procedural Management | ICU care protocol; antithrombotic therapy table; follow-up schedule; endocarditis prophylaxis |
| 10. Special Topics | ViV TAVI; BAV; asymptomatic AS (2025 FDA approval); coronary access post-TAVI; EPDs; GLUCO-TAVI; pure AI |
| 11. Quick Reference | Key numbers; PAVE-CS mnemonic for complications; full 18-source reference list |