Inferior wall mi
Reading File
Finding Sources
Finding Sources
Searching PubMed
"inferior wall myocardial infarction"[MeSH Terms] AND management
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from authoritative sources. Let me compile a thorough, well-structured answer.
Inferior Wall Myocardial Infarction
Anatomy and Culprit Vessel
The inferior wall of the left ventricle is supplied primarily by the right coronary artery (RCA) in right-dominant individuals (~85% of people). In left-dominant systems, the left circumflex (LCx) is responsible. Inferior MI results from occlusion of one of these vessels, most commonly the RCA.
Key anatomic point: The posteromedial papillary muscle receives its blood supply from a single coronary artery (usually the RCA), making it uniquely vulnerable in inferior MI - this explains the higher rate of papillary muscle rupture/mitral regurgitation compared to anterior MI.
ECG Diagnosis
Diagnostic criteria: ST-segment elevation in leads II, III, and aVF
| Location | ECG Findings |
|---|---|
| Inferior | ST elevation in II, III, aVF |
| Inferolateral | ST elevation in II, III, aVF + V5 and V6 |
| Inferior + RV | ST elevation in II, III, aVF + V1 (or right-sided leads V4R-V6R) |
Tintinalli's Emergency Medicine, p. 378
Key ECG Clues for the Culprit Vessel
- ST elevation greater in lead III than lead II + ST depression in I and aVL = RCA occlusion (90% sensitive, 71% specific)
- ST elevation greater in lead II than lead III, with isoelectric or elevated ST in aVL = LCx occlusion (often "electrically occult" on 12-lead)
- ST elevation in V1 in the setting of inferior STEMI suggests concomitant RV infarction
- Reciprocal ST depression in V1-V3 in inferior MI can reflect: reciprocal change, posterior extension, or simultaneous anterior ischemia
Rosen's Emergency Medicine, p. 1005-1006
Inferior MI ECG with Reciprocal Changes
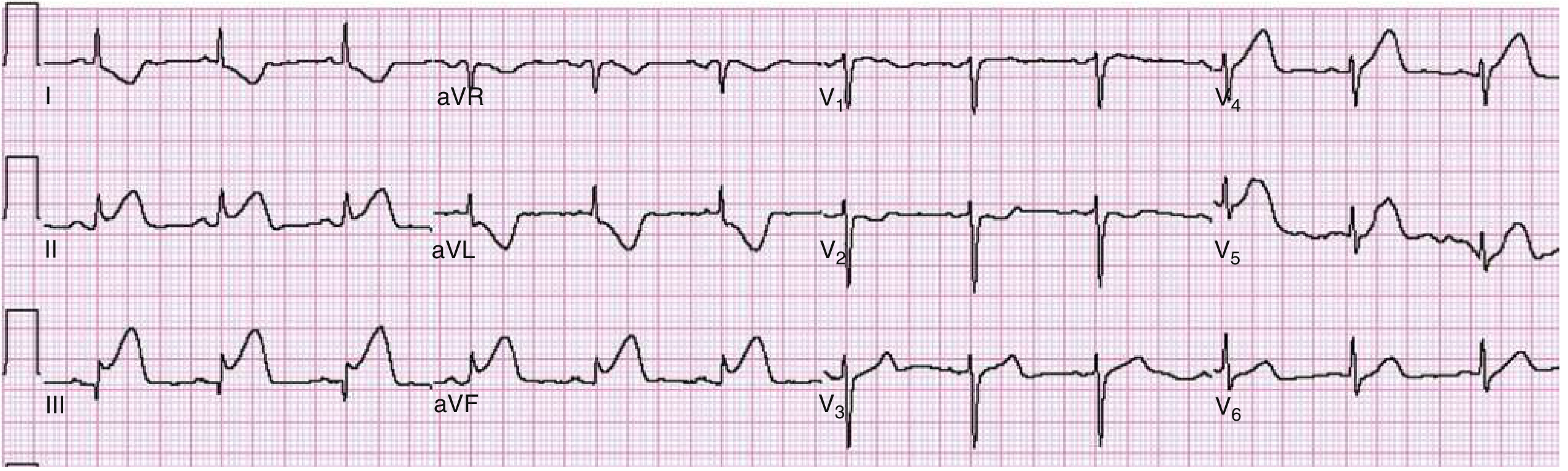
Fig: Inferior acute MI. ST elevation in leads II, III, and aVF with marked reciprocal ST depression in leads I, aVL, and anterior precordial leads.
Right Ventricular Infarction
Approximately 30% of inferior wall MIs involve the right ventricle - a major complication that fundamentally changes management. It results from proximal RCA occlusion before the acute marginal branch.
Diagnosis
- Right-sided precordial leads: ST elevation ≥1 mm in V4R-V6R (>90% sensitive and specific)
- ST elevation in standard V1 in the setting of inferior STEMI
- Clinically: elevated JVP + hypotension (Kussmaul triad, also called the Bezold-Jarisch reflex pattern)
- Nitrate-induced hypotension is a classic clue
Goldman-Cecil Medicine; Tintinalli's Emergency Medicine
Hemodynamic Mechanism
RV infarction reduces RV end-systolic pressure and cardiac output. The RV becomes a passive conduit; blood flow through the pulmonary circuit depends on LV contraction bulging the interventricular septum. Any reduction in preload (diuretics, nitrates, volume depletion) or loss of AV synchrony (atrial infarction, heart block) causes severe hemodynamic collapse.
Management of RV Infarction
- Volume loading - IV normal saline to maintain preload (first-line)
- Avoid nitrates - they reduce preload and will cause precipitous hypotension
- Avoid diuretics
- If 1-2 L NS doesn't improve output: inotropic support (dobutamine)
- Restore AV synchrony - AV sequential pacing is superior to ventricular pacing alone if high-degree block develops
- Early reperfusion (PCI) is the most effective treatment
- If concurrent LV failure: nitroprusside (reduce afterload) or intra-aortic balloon pump
Tintinalli's Emergency Medicine, p. 392
Bradycardia and AV Block
Inferior MI is the most common cause of bradycardia and AV block in the acute MI setting. Mechanisms:
- Vagal/parasympathetic activation (Bezold-Jarisch reflex) - most common, usually transient
- Ischemia of the AV nodal artery (a branch of RCA in most patients)
| Feature | Inferior MI | Anterior MI |
|---|---|---|
| Level of block | At AV node | Subnodal (infranodal) |
| Escape rhythm | Narrow QRS, 40-60 bpm | Wide QRS, slow, unreliable |
| Course | Often transient, resolves in days | More permanent, worse prognosis |
| Mechanism | Vagotonia or AV nodal ischemia | Extensive septal/His-Purkinje damage |
Fuster and Hurst's The Heart, 15th ed.
Complications
Papillary Muscle Rupture
- More common with inferior MI than anterior MI
- Usually occurs 3-5 days post-AMI
- Posteromedial papillary muscle (single blood supply from RCA) is more vulnerable than anterolateral (dual supply)
- Presents with: acute dyspnea, pulmonary edema, new holosystolic murmur (MR)
- Even with a small MI, rupture can occur
- Treatment: surgical
Pericarditis
- Pericardial friction rubs are more common with inferior and RV infarction because the right ventricle lies directly beneath the chest wall
- Treatment: aspirin 650 mg q4-6h, or colchicine 0.6 mg BID
- Avoid ibuprofen (impairs aspirin's antiplatelet effect, promotes scar thinning)
Posterior Extension
- Inferior MI frequently extends to the posterior wall ("inferobasal" by modern consensus)
- Look for: tall R waves in V1-V2, horizontal ST depression + upright T waves in V1-V2
- Confirm with posterior leads V7-V9 (ST elevation ≥0.5 mm)
- Associated with larger infarct zone, lower ejection fraction, higher mortality
Rosen's Emergency Medicine, p. 1006
Clinical Presentation Pearls
- Bradycardia is more common with inferior MI (vagal activation) - unlike anterior MI, where bradycardia/new heart block is an ominous sign
- Inferior MI can present with prominent nausea and vomiting (vagal response), sometimes mimicking GI pathology
- ST elevation in inferior leads can be mimicked by pericarditis, early repolarization, and RV strain - clinical context is essential
- Inferior MI generally carries a better prognosis than anterior MI due to smaller territory at risk, unless complicated by RV infarction
Summary Table
| Feature | Details |
|---|---|
| Culprit vessel | RCA (right dominant), less often LCx |
| ECG leads | ST elevation in II, III, aVF |
| Reciprocal changes | ST depression in I, aVL (± V1-V3) |
| RV involvement | ~30%; diagnose with V4R elevation |
| AV block | Common, often transient; AV nodal level |
| Key complication | RV infarction, papillary muscle rupture (MR) |
| Avoid in RV MI | Nitrates, diuretics |
| Treat RV MI | Volume loading, pacing, inotropes, early PCI |
Sources:
- Tintinalli's Emergency Medicine, Chapter 49
- Rosen's Emergency Medicine, Chapter 64
- Goldman-Cecil Medicine, Chapter 58
- Fuster and Hurst's The Heart, Chapter 38
This is a shared conversation. Sign in to Orris to start your own chat.