Surfactant is essential for respiration why?
Reading File
Finding Sources
Searching PubMed
pulmonary surfactant surface tension alveolar stability
Reading File
Reading File
Reading File
Loading Image
Here is a thorough explanation of why surfactant is essential for respiration, drawn from authoritative physiology and pulmonary medicine textbooks.
Why Surfactant is Essential for Respiration
1. The Problem: Surface Tension in Alveoli
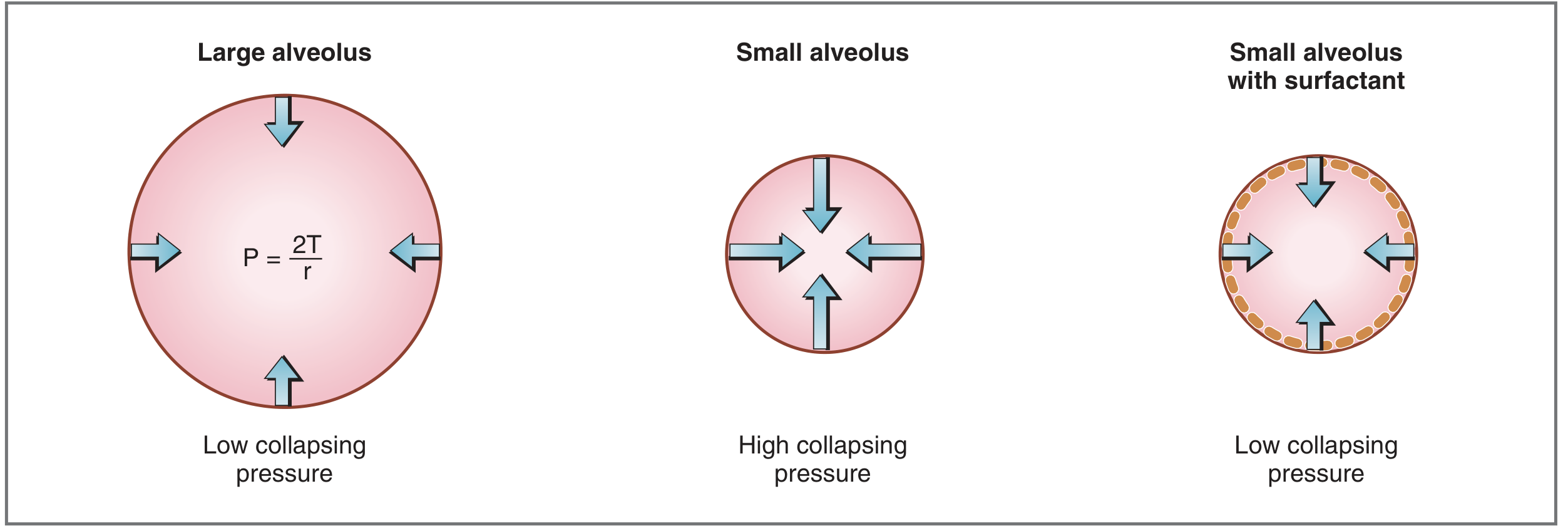
The inner surface of every alveolus is coated with a thin layer of fluid. Liquid molecules attract each other, creating surface tension - a force that acts to minimize the surface area, which in a spherical alveolus means a force that tries to collapse it.
The Law of Laplace describes this relationship:
P = 2T / r
Where P = collapsing pressure, T = surface tension, r = radius of the alveolus.
This means:
- Large alveoli - bigger radius, lower collapsing pressure - relatively stable
- Small alveoli - smaller radius, higher collapsing pressure - prone to collapse (atelectasis)
Without something to counteract this, every small alveolus would collapse after each breath, making re-inflation require enormous force and making gas exchange impossible.
2. What Surfactant Is
Surfactant is a mixture of lipids and proteins secreted into the alveolar space by type II alveolar cells (AT2 cells). Its key components are:
- Dipalmitoylphosphatidylcholine (DPPC) - the most important component, comprising ~50-60% of surfactant lipid
- Unsaturated phosphatidylcholine, phosphatidylglycerol
- Four surfactant-associated proteins (SP-A, SP-B, SP-C, SP-D)
DPPC is amphipathic - it has a hydrophilic (water-loving) head and a hydrophobic (water-repelling) tail. DPPC molecules align themselves at the alveolar air-liquid interface, with hydrophobic portions attracted to each other and hydrophilic portions repelled from each other. This intermolecular arrangement disrupts the attractive forces between water molecules that were responsible for high surface tension. The result: surface tension and collapsing pressure are dramatically reduced.
3. What Surfactant Does - Four Key Functions
| Function | Mechanism | Consequence if absent |
|---|---|---|
| Prevents alveolar collapse | Reduces surface tension, lowering collapsing pressure | Widespread atelectasis |
| Stabilizes alveoli of different sizes | Reduces T more in smaller alveoli (denser DPPC packing at low volumes) | Small alveoli collapse into large ones |
| Increases lung compliance | Less force needed to expand alveoli during inspiration | Greatly increased work of breathing |
| Prevents alveolar edema | Low surface tension means less fluid drawn into alveoli | Fluid accumulation impairs gas exchange |
4. Why Alveolar Stability is Especially Critical
Without surfactant, not only do small alveoli collapse, but by the Law of Laplace, air from small high-pressure alveoli would be forced into large low-pressure alveoli - causing uneven ventilation. Surfactant compensates for this because DPPC molecules pack more tightly as radius decreases, so surface tension falls even further as an alveolus shrinks. This makes the collapsing pressure roughly equal across alveoli of different sizes, keeping them all open.
5. Clinical Consequences of Surfactant Deficiency
Neonatal Respiratory Distress Syndrome (NRDS / Hyaline Membrane Disease)
- Surfactant synthesis by AT2 cells begins around gestational week 24 and is reliably present by week 35
- Premature infants born before week 35 may lack surfactant
- Consequences:
- High alveolar surface tension → widespread atelectasis
- Collapsed alveoli are not ventilated → shunting → hypoxemia
- Decreased lung compliance → massive increase in work of breathing
- Retention of fluid in the lungs (immature ENaC channels fail to absorb fluid normally)
- Treatment: exogenous surfactant replacement therapy (intratracheal instillation)
Adult Respiratory Distress Syndrome (ARDS)
- Surfactant is inactivated by inflammatory mediators, proteins, and cell damage
- Results in the same physiological consequences as neonatal deficiency: diffuse atelectasis, shunting, stiff lungs, hypoxemia
Pulmonary Alveolar Proteinosis (PAP)
- Overproduction or dysregulated clearance of surfactant proteins
- Alveoli fill with surfactant material, impairing gas exchange
Summary
Surfactant is essential because without it:
- Small alveoli collapse due to unopposed surface tension (Laplace's Law)
- Lungs become stiff, requiring enormous inspiratory effort
- Ventilation-perfusion mismatch (shunting) causes hypoxemia
- Gas exchange becomes impossible in collapsed units
In essence, surfactant is what allows normal quiet breathing to be effortless and effective.
Sources: Costanzo Physiology 7th Edition, p. 210; Ganong's Review of Medical Physiology 26th Edition, p. 632; Murray & Nadel's Textbook of Respiratory Medicine
Search for recent research on surfactant replacement therapy in ARDS
Foetal haemoglobin more affinity for oxygen why?
Searching PubMed
surfactant replacement therapy ARDS
Finding Sources
Searching PubMed
surfactant therapy adult \"acute respiratory distress syndrome\"
Finding Sources
Finding Sources
Reading Article
PMID: 41407316
Reading Article
PMID: 37497603
Finding Sources
Finding Sources
Reading Article
PMID: 38684519
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have everything I need from the textbooks already. Here are both comprehensive answers:
Part 1: Recent Research on Surfactant Replacement Therapy in ARDS
Background: Why Adult ARDS is Different from Neonatal RDS
In ARDS, surfactant dysfunction arises from a different mechanism than neonatal deficiency. Rather than absence of production, ARDS causes inactivation of existing surfactant by:
- Plasma proteins leaking into alveoli (fibrinogen, albumin compete with DPPC)
- Inflammatory mediators from recruited neutrophils and macrophages
- Destruction of type II alveolar cells (AT2) that produce surfactant
- Oxidative stress damaging surfactant lipids and proteins
This distinction is key - it explains why simply replacing surfactant in adults has been harder than in neonates.
What Recent Research Shows
1. The Core Problem: Past Trials Were Inconclusive
A major 2026 review [Lee KG et al., J Appl Physiol, PMID: 41407316] titled "Surfactant therapy for the treatment of acute respiratory distress syndrome: time to revisit?" provides the most current synthesis:
- Exogenous surfactant has not shown consistent mortality benefit in adult ARDS in past clinical trials
- However, the review argues past trial failures may reflect methodological flaws, not a lack of biological efficacy
- Key shortcomings identified:
- Wrong formulations - early trials used protein-free synthetic surfactants that lacked SP-B and SP-C (needed for resistance to inactivation)
- Inadequate dosing - insufficient phospholipid dose to overcome inhibition by plasma proteins
- Wrong delivery route - aerosol delivery failed to reach collapsed alveoli; intratracheal bolus is superior
- Heterogeneous patient populations - ARDS is not one disease; patients were not stratified by surfactant dysfunction severity
- The review concludes: "Advances in surfactant research suggest a potential role for exogenous surfactant therapy for adult patients with ARDS" - calling for new, better-designed trials
2. New Synthetic Surfactants Show Promise in Animal Models
A 2024 study [Mikolka P et al., Lung, PMID: 38684519] tested the synthetic surfactant CHF5633 (containing analogues of SP-B and SP-C) in a severe adult rabbit ARDS model:
- Results: Both CHF5633 and natural surfactant (Poractant alfa/Curosurf) produced comparable:
- Improvements in oxygenation (P/F ratio)
- Reduction in lung injury score
- Reduction in pro-inflammatory cytokines
- Decreased lung edema
- Why this matters: CHF5633 is a synthetic surfactant with modified peptide analogues designed to resist inactivation in the inflammatory ARDS environment - a key limitation of older preparations
- Conclusion: Clinical trials with newer-generation surfactants are warranted
3. Surfactant in COVID-19 ARDS
A 2023 narrative review [Khudadah K et al., Biosci Rep, PMID: 37497603] examined surfactant therapy specifically for COVID-19-associated ARDS:
- Rationale: SARS-CoV-2 spike protein directly targets AT2 cells, destroying the cells that make surfactant - causing a pattern resembling neonatal RDS more closely than classic ARDS
- Post-mortem findings: Desquamated AT2 cells with hyaline membrane formation
- Clinical findings from two trials: Inhaled/intratracheal surfactant produced marked improvement in respiratory parameters (oxygenation, compliance) but not mortality
- Surfactant also proposed as a drug delivery vehicle (liposomal carrier) for antiviral agents directly to alveoli
- Conclusion: Larger comparative trials needed on formulation and delivery method
4. Inhaled PEG-ADM: A Novel Surfactant-Related Approach (2025 RCT)
A 2025 Phase II multicenter RCT [Karagiannidis C et al., Crit Care, PMID: 41131549] tested inhaled PEG-ADM (adrenomedullin), a vasoprotective peptide that also modulates surfactant function, in ARDS patients. This represents one of the newer biological approaches to protecting alveolar function in ARDS beyond traditional surfactant replacement.
Summary Table
| Area | Current Status |
|---|---|
| Neonatal RDS | Surfactant replacement = standard of care, proven effective |
| Adult ARDS (overall) | Past trials inconclusive; new trials warranted with better formulations |
| COVID-19 ARDS | Respiratory improvement shown; mortality benefit not yet proven |
| Synthetic surfactants (CHF5633) | Promising in animal models; human trials pending |
| Key problem | Inactivation by plasma proteins; inadequate delivery in past trials |
| Future direction | Newer protein-containing surfactants + intratracheal bolus + targeted patient selection |
Key sources: Lee KG et al. (2026) [PMID: 41407316]; Mikolka P et al. (2024) [PMID: 38684519]; Khudadah K et al. (2023) [PMID: 37497603]
Part 2: Why Fetal Haemoglobin (HbF) Has Higher Oxygen Affinity
The Core Answer in One Sentence
HbF binds oxygen more avidly than adult HbA because its gamma (γ) chains interact much more weakly with 2,3-bisphosphoglycerate (2,3-BPG) - the molecule that normally reduces hemoglobin's affinity for oxygen.
Step-by-Step Explanation
Step 1: Structure of HbF vs HbA
| Hemoglobin | Globin chains | Who has it |
|---|---|---|
| HbA (adult) | α₂β₂ | Normal adults (>97%) |
| HbF (fetal) | α₂γ₂ | Fetus; <1% in normal adults |
The critical difference is the γ (gamma) chain in HbF replacing the β (beta) chain in HbA. This single structural difference has a profound physiological consequence.
Step 2: The Role of 2,3-BPG (2,3-Bisphosphoglycerate)
2,3-BPG is a negatively charged molecule produced in red blood cells by the Rapoport-Luebering shunt. It acts as a "brake" on oxygen binding:
- 2,3-BPG fits into the central cavity of deoxyhemoglobin and binds to the β chains
- This stabilizes the taut (T) conformation of hemoglobin (the low-affinity form)
- Result: hemoglobin releases oxygen more readily to tissues (rightward shift of ODC)
- Without 2,3-BPG, hemoglobin stays in the relaxed (R) conformation and holds oxygen tightly
Step 3: Why HbF Ignores 2,3-BPG
The γ chain of HbF has a serine residue at position 143, whereas the β chain of HbA has a histidine at the same position. Histidine is positively charged - it forms a salt bridge with the negatively charged 2,3-BPG. Serine is neutral - it cannot form this bond.
The result: 2,3-BPG binds weakly to HbF compared to HbA.
Because 2,3-BPG cannot effectively stabilize the T (deoxy) conformation of HbF, HbF remains in the high-affinity R conformation and holds onto oxygen more tightly.
As Lippincott's Biochemistry states: "Because 2,3-BPG reduces the affinity of hemoglobin for oxygen, the weaker interaction between 2,3-BPG and HbF results in a higher oxygen affinity for HbF relative to HbA."
Step 4: Why This Matters Physiologically - The Placenta
The fetus lives in a relatively oxygen-poor environment (fetal PaO₂ is only ~30-35 mmHg). Oxygen must be transferred from maternal blood to fetal blood across the placenta. This is only possible because of a concentration (partial pressure) gradient - but that gradient is small.
HbF's higher oxygen affinity solves this problem:
- In the placenta: At the same PO₂, HbF picks up more oxygen than maternal HbA releases - creating a net transfer from mother to fetus
- The ODC curve: HbF's oxygen-dissociation curve is shifted to the LEFT compared to HbA - meaning HbF loads oxygen at lower partial pressures
- This allows the fetus to "steal" oxygen from maternal blood even though maternal blood is not highly oxygenated
"To aid oxygen transfer, the fetal hemoglobin oxygen dissociation curve is shifted to the left such that fetal hemoglobin has a greater affinity for oxygen than does maternal hemoglobin." - Morgan & Mikhail's Clinical Anesthesiology
Step 5: Transition After Birth
At birth, the situation reverses: now the problem is delivering oxygen to fetal tissues (not loading it). High oxygen affinity means HbF reluctantly releases oxygen. The body compensates:
- Levels of 2,3-DPG rise in neonatal red cells
- The resulting mild acidosis (Bohr effect) reduces oxygen affinity
- Over 1-2 months, γ chains are gradually replaced by β chains (HbF → HbA switch)
Summary
| Feature | HbA (Adult) | HbF (Fetal) |
|---|---|---|
| Globin chains | α₂β₂ | α₂γ₂ |
| 2,3-BPG binding | Strong (His-143 on β chain) | Weak (Ser-143 on γ chain) |
| Oxygen affinity | Normal | Higher |
| ODC curve | Normal | Shifted LEFT |
| P50 (PO₂ at 50% saturation) | ~27 mmHg | ~20 mmHg |
| Physiological purpose | O₂ delivery to tissues | O₂ loading from placenta |
Sources: Mulholland & Greenfield's Surgery, p. 5282; Lippincott's Biochemistry 8th Ed, p. 135; Morgan & Mikhail's Clinical Anesthesiology 7e, p. 1583
。
It looks like you sent just a punctuation mark. Did you mean to type something? Feel free to ask your next question!
Foetal haemoglobin more affinity for oxygen why? For 3 mark ans for university exam
Here is a concise 3-mark university answer:
Fetal Haemoglobin (HbF) - Higher Oxygen Affinity
1. Structural difference (γ chains instead of β chains)
HbF has the composition α₂γ₂, unlike adult HbA (α₂β₂). The γ (gamma) chains replace the β (beta) chains.
2. Weaker binding to 2,3-BPG
The γ chain has a serine at position 143, whereas the β chain has a histidine. Histidine is positively charged and forms a strong electrostatic bond with 2,3-bisphosphoglycerate (2,3-BPG). Serine is neutral and cannot bind 2,3-BPG effectively. Since 2,3-BPG normally stabilizes the low-affinity (T/deoxy) conformation of haemoglobin, its reduced binding to HbF means HbF stays in the high-affinity (R/oxy) conformation.
3. Physiological significance
HbF's oxygen-dissociation curve is shifted to the left (lower P50 ~20 mmHg vs ~27 mmHg for HbA). This allows HbF to load oxygen at the low PO₂ of the placenta (~30-35 mmHg), facilitating oxygen transfer from maternal blood to the fetus.
One-line summary for exams: HbF has higher O₂ affinity because its γ chains bind 2,3-BPG poorly, keeping it in the relaxed (high-affinity) conformation, which left-shifts its ODC curve and enables placental O₂ uptake.
This is a shared conversation. Sign in to Orris to start your own chat.