Recent management of pul embolism
Reading File
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND management
Searching the Web
pulmonary embolism management guidelines 2024 2025 ESC AHA anticoagulation thrombolysis
Reading File
Reading Article
PMID: 41712677
Reading Web Page
https://www.chestphysician.org/navigating-pe-treatment-what-…
Reading File
Loading Image
I now have comprehensive, current information to write a thorough answer. Let me compile it.
Recent Management of Pulmonary Embolism
The most current guidance comes from the landmark 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline (Creager et al., Circulation 2026; PMID 41712677), the first de novo multi-society PE guideline for adults. Its key innovation is a new clinical category system replacing older binary "massive/submassive" terminology.
1. Initial Triage - The First Branch Point
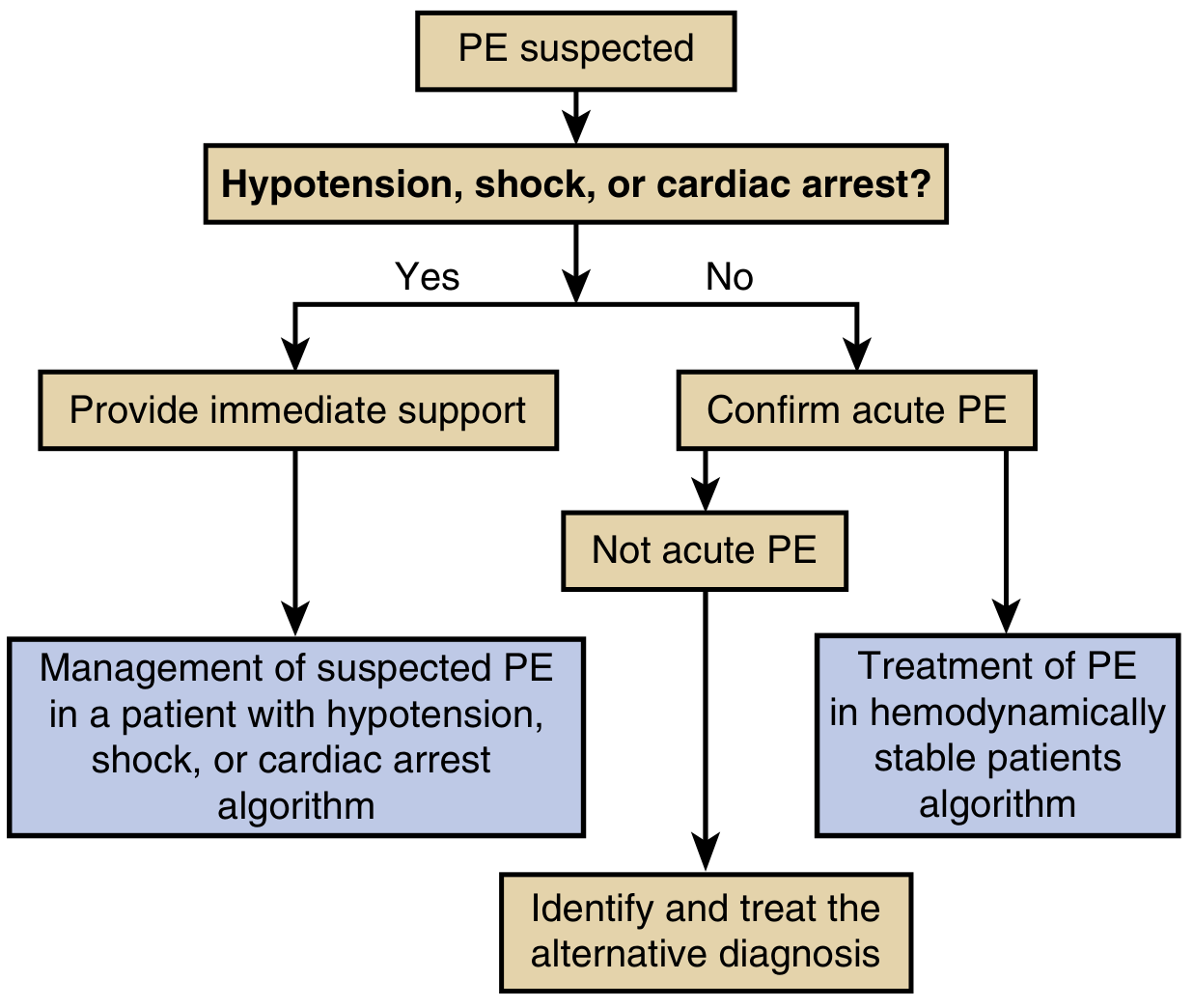
Murray & Nadel's Textbook of Respiratory Medicine
The first question is whether the patient has hypotension, shock, or cardiac arrest. This determines the entire management pathway:
- Hemodynamically unstable - immediate supportive care + empirical treatment path
- Hemodynamically stable - confirm diagnosis, then risk-stratify
For unstable patients with suspected PE and no time for imaging, bedside ultrasonography is used to assess for RV failure, clot-in-transit, or DVT. Clinicians must sometimes treat empirically without diagnostic confirmation. Avoid intubation if possible (induction agents can cause hemodynamic collapse); prefer CPAP/HFNO. If intubation is unavoidable, use etomidate to preserve sympathetic tone.
2. New AHA/ACC Clinical Category System (2026)
The 2026 guideline replaces "massive/submassive/low-risk" with 5 lettered categories based on integrated clinical, biomarker, and imaging data:
| Category | Description | Key Features |
|---|---|---|
| A | Incidental PE | Asymptomatic, found incidentally |
| B | Low clinical severity | Symptomatic, low PESI/sPESI score |
| C1/C2/C3 | Elevated clinical severity, no shock | Rising RV strain markers, escalating severity |
| D1/D2 | Incipient cardiopulmonary failure | Borderline hemodynamics, threatened decompensation |
| E1/E2 | Overt cardiopulmonary failure | Active shock (E1) or cardiac arrest/refractory shock (E2) |
3. Risk Stratification Tools
sPESI (Simplified Pulmonary Embolism Severity Index) - one point each for:
- Age > 80 years
- History of cancer
- Chronic cardiopulmonary disease
- Pulse ≥ 110 bpm
- SBP < 100 mmHg
- SpO2 < 90%
A score of 0 = low mortality risk. Any score ≥ 1 = high risk.
Cardiac biomarkers (troponin, BNP/NT-proBNP) are incorporated into the category system. For categories C-D (elevated severity without shock), RV imaging is strongly recommended (LOE A) for short-term risk stratification.
4. Anticoagulation - The Foundation of Treatment
Preferred agents
| Situation | Preferred anticoagulant |
|---|---|
| Categories A & B (low risk) | DOAC (apixaban or rivaroxaban preferred over VKA) - including in obesity, mild-moderate CKD, brain tumors |
| Categories C, D, E (higher risk) | LMWH (preferred over UFH for initial treatment) |
| Systemic thrombolysis planned | UFH (rapid reversal possible) |
| Renal failure, pregnancy, reversal needed | UFH or LMWH per clinical context |
DOACs (apixaban, rivaroxaban, dabigatran, edoxaban) are first-line over warfarin in most patients due to predictable dosing, no INR monitoring, and fewer drug interactions.
IVC filter - routine placement should NOT be performed in therapeutically anticoagulated patients (harm; LOE A). Reserved for absolute contraindications to anticoagulation.
5. Advanced/Reperfusion Therapies
This is the most evolved area of the 2026 guideline. All reperfusion modalities are now placed in the same framework:
Systemic Thrombolysis (tPA 100 mg over 2 hours)
- Category E2 (cardiac arrest / refractory shock): systemic thrombolysis is the preferred reperfusion therapy over other options
- Categories A1 to C2 (no shock): systemic thrombolysis should NOT be used vs anticoagulation alone due to increased major bleeding and ICH risk (harm; LOE B-R)
- Category E1 (persistent hypotension with shock): systemic thrombolysis, CDT, MT, and surgical embolectomy are all given equal strength of recommendation
Catheter-Directed Thrombolysis (CDT) / Ultrasound-Facilitated CDT (USCDT)
- USCDT (EkoSonic/EKOS device) delivers low-dose tPA directly into thrombus
- The HI-PEITHO trial (2026, NEJM) evaluated USCDT vs anticoagulation alone and its results are shaping current intermediate-risk management
- For categories C2 to D2: whether CDT is superior to mechanical thrombectomy for reducing mortality or major bleeding is currently uncertain (COR 2b; LOE B-R)
Mechanical Thrombectomy (MT)
- Large-bore aspiration thrombectomy (FlowTriever, Indigo) removes thrombus without thrombolytics
- The PEERLESS RCT (Jaber et al., Circulation 2025) compared large-bore MT vs CDT for intermediate-risk PE - found MT noninferior/superior on select outcomes with lower bleeding risk
- Role in categories C2/C3 remains under refinement; reasonable for those at high bleeding risk
Surgical Embolectomy
- Reserved for massive PE with contraindication to thrombolytics, or failure of catheter-based therapy
- Considered at equal level to other reperfusion options in category E1
Clot-in-Transit
- For categories C3 to E2 with free-floating RA/RV clot-in-transit, advanced therapy vs anticoagulation alone is reasonable (COR 2a; LOE C-LD)
6. Pulmonary Embolism Response Team (PERT)
For patients with increased risk of adverse outcomes (categories C-E), PERT consultation is strongly recommended (LOE B-NR). PERT is a multidisciplinary team (pulmonology, cardiology, hematology, interventional radiology, cardiac surgery, vascular medicine) that:
- Expedites decision-making
- Selects appropriate reperfusion strategy
- Improves in-hospital outcomes per meta-analysis (Maqsood et al., 2025, PMID 40258457)
7. Duration of Anticoagulation
| Provoking factor | Recommended duration |
|---|---|
| Major transient (e.g., surgery, trauma) | 3 months |
| Minor transient (e.g., travel, OCP) | 3-6 months |
| Unprovoked first PE | ≥ 3 months, reassess; indefinite if low bleeding risk |
| Recurrent unprovoked PE | Indefinite |
| Active cancer | Extended (LMWH or DOAC - edoxaban, rivaroxaban preferred) |
| Antiphospholipid syndrome | Warfarin (DOACs inferior in high-risk APLS) |
8. Outpatient Management of Low-Risk PE
Patients in categories A and B who are hemodynamically stable, have adequate home support, and no serious comorbidities can be safely managed as outpatients or with early discharge (within 24-48 hours). The Hestia criteria and sPESI = 0 help identify candidates for home treatment.
9. Follow-Up and Long-Term Complications
- Early follow-up within 1 week of discharge is strongly recommended (LOE C-LD) to reinforce adherence, detect bleeding, and educate patients
- Screen for chronic thromboembolic pulmonary hypertension (CTEPH) at 3-6 months if persistent dyspnea. The SYSPPE study (2024) supports symptom-based screening protocols
- Post-PE syndrome (exercise intolerance, reduced quality of life) affects up to 50% - refer for pulmonary rehabilitation if indicated
Summary Algorithm
PE suspected
|
+--> Hemodynamic compromise? YES --> Immediate support, empiric treatment
| Systemic lysis if cardiac arrest (Cat E2)
| PERT activation
|
+--> NO --> Confirm by CTPA / V/Q scan
|
+--> Risk stratify (sPESI, troponin, RV imaging)
|
+--> Category A/B --> DOAC, consider outpatient
|
+--> Category C --> LMWH/DOAC + PERT assessment
| Consider advanced therapy if C3 + RV strain
|
+--> Category D --> LMWH, PERT, evaluate for CDT or MT
|
+--> Category E1 --> Any reperfusion + PERT (equal COR)
+--> Category E2 --> Systemic tPA preferred
Key recent developments to remember:
- The 2026 AHA/ACC guideline introduced the A-E clinical category system, replacing older terminology
- LMWH is now preferred over UFH for initial parenteral anticoagulation in intermediate/high-risk PE
- Large-bore mechanical thrombectomy (PEERLESS trial) has emerged as a genuine alternative to CDT with potentially lower bleeding risk
- PERT teams are now strongly recommended (not just suggested) for high-risk categories
- Systemic thrombolysis is restricted to categories D2/E only - do NOT use in intermediate-risk without shock
- Routine IVC filter placement is explicitly harmful in anticoagulated patients (LOE A)
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 1877-1885
- 2026 AHA/ACC PE Guideline, Circulation (Creager et al.)
- PEERLESS RCT - large-bore MT vs CDT (Jaber et al., Circulation 2025)
- 2025 ESVM Interventional VTE Guidelines (PMID 40587333)
This is a shared conversation. Sign in to Orris to start your own chat.