Lymphatic drainage of testicular tumors
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Excellent - I now have all the core information needed. Here is the complete answer:
Lymphatic Drainage of Testicular Tumors
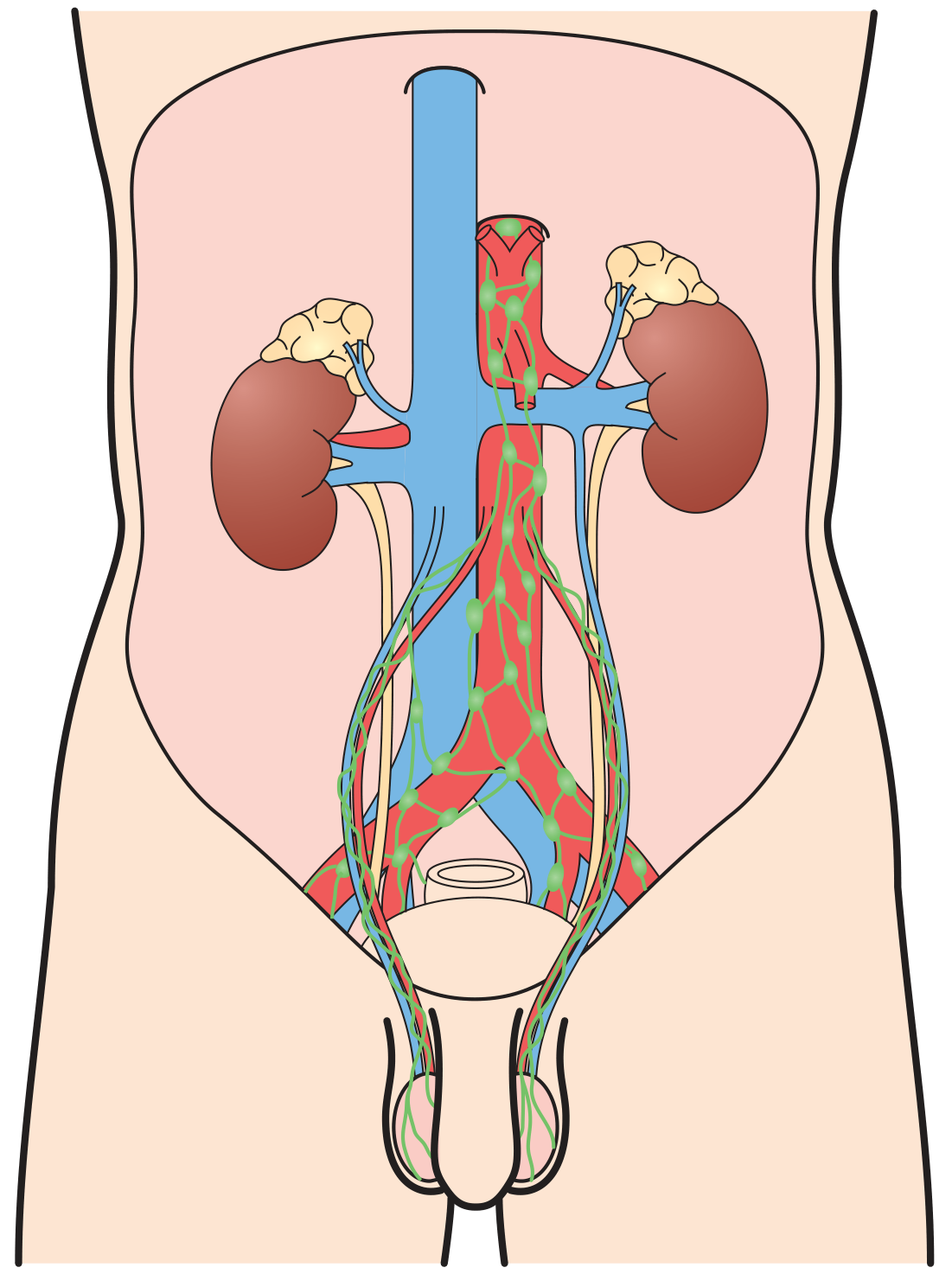
Embryological basis
The testes originate in the retroperitoneum from the urogenital ridge near L1-L2 and descend into the scrotum during fetal development, carrying their blood supply and lymphatics with them. This is why testicular lymphatics drain upward to the retroperitoneum, not to the inguinal nodes (which drain the scrotum and perineum).
Primary Drainage: Retroperitoneal Nodes
The retroperitoneum is the initial site of metastatic spread in 70-80% of patients with germ cell tumors (GCT). The route varies by side:
| Side | Primary Landing Zone | Secondary Nodes |
|---|---|---|
| Right testis | Interaortocaval nodes (inferior to renal vessels) | Paracaval and para-aortic nodes |
| Left testis | Para-aortic (PA) nodes | Interaortocaval nodes |
The pattern of retroperitoneal spread is right to left. This means:
- Right-sided tumors commonly spread contralaterally to the left PA nodes
- Left-sided tumors rarely cross to the right, unless disease is bulky
Stepwise Spread Beyond the Retroperitoneum
Once retroperitoneal nodes are involved, spread continues predictably:
- Retroperitoneal lymphatics drain into the cisterna chyli (behind the right renal artery and right crus of the diaphragm)
- From there via the thoracic duct to the posterior mediastinum
- Then to the left supraclavicular fossa (Virchow's node)
When Inguinal Nodes ARE Involved
Inguinal node involvement is not the primary route but occurs in specific circumstances:
- Invasion of the scrotal skin or tunica vaginalis
- Invasion of the epididymis (which has its own lymphatic drainage)
- Prior scrotal or inguinal surgery (e.g., orchiopexy, scrotal orchidectomy) - which disrupts normal lymphatic channels and can redirect drainage to inguinal nodes
- Retrograde spread from bulky retroperitoneal disease causing distal iliac/inguinal node involvement
Caudal Retrograde Spread
More caudal deposits (distal iliac and inguinal nodes) usually reflect retrograde spread from large-volume retroperitoneal disease, or, rarely, aberrant testicular lymphatic drainage.
Hematogenous Exception: Choriocarcinoma
While virtually all GCT types disseminate primarily via lymphatics, choriocarcinoma is the exception - it has a strong propensity for hematogenous dissemination, with early spread to the lungs, liver, and brain.
Clinical Relevance: Staging and Surgery
- CS I: disease confined to testis; CS II: regional (retroperitoneal) nodes; CS III: non-regional or visceral metastasis
- CT of abdomen/pelvis (with contrast) is the standard staging tool; nodes ≥5-9 mm in the primary landing zone warrant suspicion
- RPLND (retroperitoneal lymph node dissection) templates are designed around these landing zones; bilateral templates cover all primary drainage sites while modified templates focus on side-specific landing zones
- Because of the right-to-left drainage pattern, a modified right-sided template must still include left-sided nodes in the interaortocaval zone
Sources: Campbell-Walsh-Wein Urology, p. 2251; Bailey and Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.