a patient present with lump beside the testicles. with pain
Reading File
Finding Sources
Finding Sources
Searching PubMed
scrotal lump epididymitis differential diagnosis
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Now I have comprehensive textbook content. Let me compile a thorough clinical response.
Painful Lump Beside the Testicle - Clinical Approach
A lump beside (paratesticular/extratesticular) the testicle with pain narrows the differential significantly compared to intratesticular lumps. This is a classic presentation requiring systematic evaluation to rule out emergencies (torsion) from manageable conditions.
Differential Diagnosis
1. Epididymitis / Epididymo-orchitis (MOST COMMON)
The most common intrascrotal inflammatory disease. The epididymis lies along the posterior aspect of the testis, so an inflamed epididymis presents as a lump beside/behind the testicle.
Key features:
- Scrotal pain of gradual onset (distinguishes it from torsion's sudden onset)
- Pain may initially reside in the lower abdomen or flank (vas deferens inflammation)
- Tenderness starts localized to the epididymis, then spreads to the ipsilateral testis
- Scrotum may become edematous and erythematous
- Testis in normal anatomic position, with an intact cremasteric reflex
- Fever is uncommon but possible
- Urethral discharge only in ~10% of sexually acquired cases
Causes by age:
| Age Group | Common Organisms |
|---|---|
| <35 years (sexually active) | Chlamydia trachomatis, N. gonorrhoeae |
| >35 years | Urinary pathogens (E. coli, Klebsiella) |
| All ages | Enteric organisms in anal-insertive partners |
| Rare | M. tuberculosis, Behcet syndrome, amiodarone |
2. Testicular Torsion (EMERGENCY - Must Exclude First)
- Sudden-onset severe pain - the key differentiator
- Testicle often elevated/transverse lie ("bell clapper" deformity)
- Absent cremasteric reflex - highly suggestive
- No fever, no urinary symptoms
- Peak ages: neonates and puberty
- Surgical emergency - viability depends on time from onset
⚠️ No single history or physical finding reliably distinguishes torsion from epididymitis. When in doubt, urgent scrotal Doppler ultrasound is essential.
3. Torsion of Appendix Testis (Most Common Cause of Acute Scrotum Overall - 40-60%)
- Small appendage (embryological remnant) on the upper pole of the testis twists
- Pain onset can be abrupt but usually less severe than cord torsion
- Classic "blue dot sign" - bluish tender nodule visible through scrotal skin in thin patients
- Cremasteric reflex intact
- Managed conservatively with NSAIDs, scrotal support
4. Epididymal Cyst / Spermatocele
- Usually painless (pain if large, tense, or infected)
- Smooth, transilluminable cyst at the head of the epididymis
- Spermatocele contains milky fluid with spermatozoa
- Managed conservatively unless symptomatic
5. Varicocele
- Dilated pampiniform plexus veins - feels like "bag of worms"
- 90% on the left side (due to left gonadal vein draining into left renal vein at a right angle)
- Dull aching pain, often worse on standing or Valsalva
- Important cause of male infertility
6. Hernia / Hydrocele
- Inguinal hernia can present as a paratesticular lump
- Hydrocele: fluid collection around the testis - transilluminates
- Can become painful if incarcerated (hernia) or infected
7. Other (Less Common)
- Paratesticular tumor (e.g., rhabdomyosarcoma in young males, lipoma, adenomatoid tumor) - usually painless but pain if large or hemorrhagic
- Hematocele - blood in tunica vaginalis (trauma history)
- Orchitis - mumps, vasculitis (HSP in children)
Clinical Examination
| Finding | Significance |
|---|---|
| Tender, enlarged posterior/lateral lump | Epididymitis |
| Absent cremasteric reflex | Testicular torsion |
| "Blue dot" upper pole | Appendix testis torsion |
| Bag-of-worms feel, worse standing | Varicocele |
| Transilluminates | Hydrocele/cyst |
| Thickened/nodular epididymis + systemic illness | TB epididymitis |
| Prehn's sign (pain relief on lifting) | Classically epididymitis, but LOW reliability |
Investigations
Urgent (if torsion cannot be excluded):
- Scrotal Doppler ultrasound - gold standard; shows absent/reduced blood flow in torsion, increased flow in epididymitis
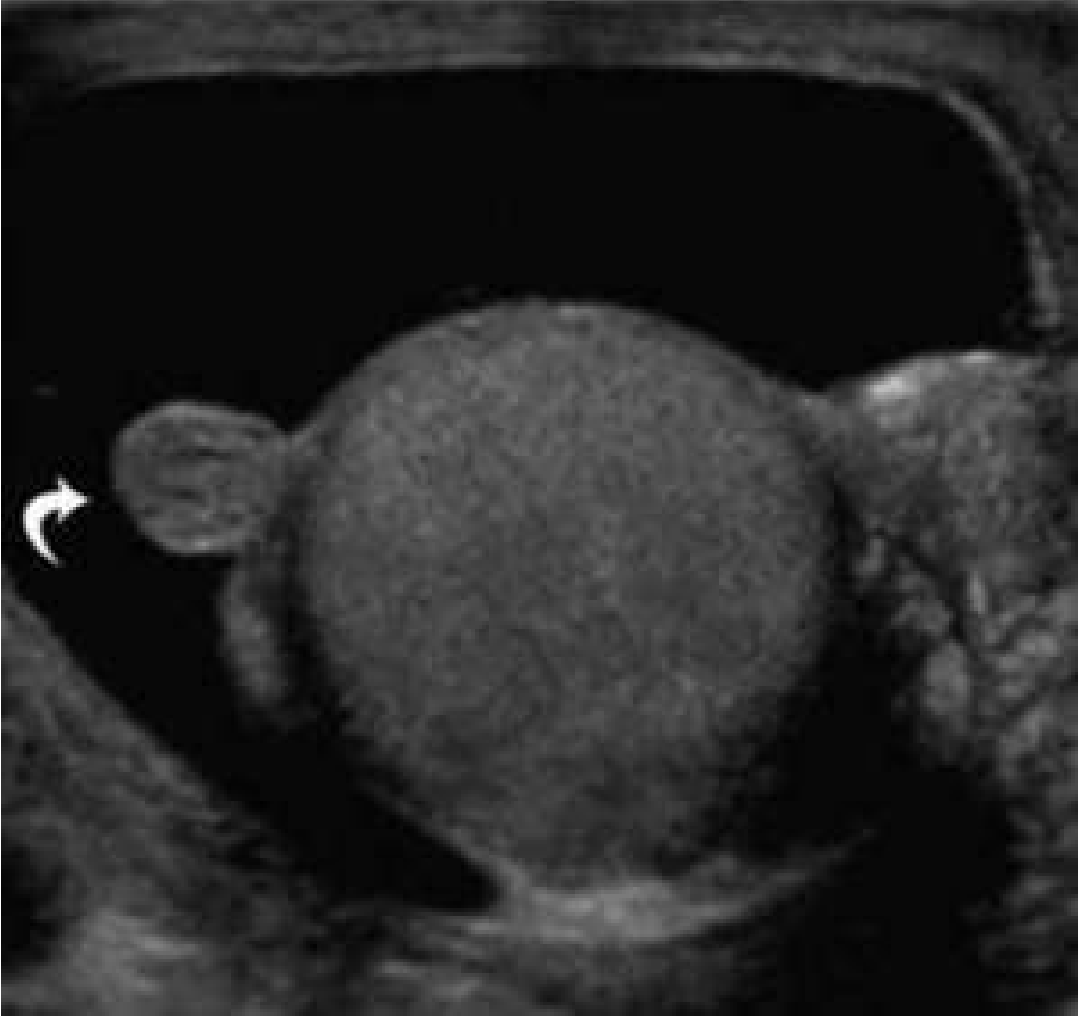
Below image from Rosen's Emergency Medicine shows a hyperechoic paratesticular mass adjacent to the testis with reactive hydrocele - typical appearance of appendage pathology:
Routine:
- Urinalysis + urine culture (pyuria suggests epididymitis)
- Urethral swab / first-void PCR for Chlamydia and Gonorrhoeae (if STI risk)
- FBC (leukocytosis = nonspecific but supports infection)
- Serum tumor markers (AFP, b-hCG, LDH) if malignancy suspected
Management
Epididymitis Treatment (from Rosen's Emergency Medicine)
| Scenario | Treatment |
|---|---|
| Sexually acquired | Ceftriaxone 500 mg IM once + Doxycycline 100 mg PO BD for 10-14 days |
| Enteric organisms (>35y, no STI risk) | Levofloxacin 500 mg PO daily for 10 days |
| Uncertain/mixed risk | Ceftriaxone 500 mg IM once + Levofloxacin 500 mg PO daily for 10 days |
Supportive measures for all: scrotal elevation, ice packs, NSAIDs for pain
If Torsion Cannot Be Excluded
- Immediate surgical exploration - do not wait for investigations
- Time to detorsion is critical: >99% salvage within 6 hours, drops sharply after 12 hours
Key Clinical Rule
"If in doubt - rule out torsion first." A painless lump is more likely to be a benign cyst, spermatocele, or varicocele. A painful lump that came on suddenly must be treated as torsion until proven otherwise. A painful lump with gradual onset + urinary symptoms + age <35 with STI risk strongly points to epididymitis.
Sources: ROSEN's Emergency Medicine - Concepts and Clinical Practice (pp. 1403-1406); Campbell Walsh Wein Urology 3-Volume Set (pp. 1148-1152); Park's Textbook of Preventive and Social Medicine
which specialist is suitable for this case
Based on the previous case (painful paratesticular lump), here is a straightforward answer:
Appropriate Specialist(s)
1. Urologist — Primary Specialist
A urologist is the most appropriate specialist for this case. They manage the full spectrum of scrotal pathology including:
- Epididymitis / epididymo-orchitis
- Testicular torsion (surgical exploration)
- Varicocele
- Hydrocele / spermatocele
- Paratesticular tumors
- Recurrent infections with underlying urinary tract abnormalities
2. Emergency Physician — First Contact (if acute)
If the pain is sudden and severe, the patient should go to the Emergency Department first, not wait for a urology outpatient appointment. Testicular torsion is a time-critical surgical emergency, and the ED team will arrange urgent urology review.
Referral Pathway Summary
Acute sudden pain
→ Emergency Department → Emergency Urologist (surgical exploration)
Gradual onset pain + urinary symptoms
→ General Practitioner (initial antibiotics + urine PCR)
→ Refer to Urologist if no improvement, recurrence, or imaging needed
Suspected malignancy / painless hard lump
→ Urgent Urologist referral (within 2 weeks)
Secondary Specialists (Specific Scenarios)
| Scenario | Additional Specialist |
|---|---|
| STI-related epididymitis | Genitourinary Medicine (GUM) / Sexual Health clinic |
| TB epididymitis confirmed | Infectious Disease specialist |
| Male infertility from varicocele | Andrologist / Reproductive Urologist |
| Malignancy confirmed | Urological Oncologist |
| Child / adolescent | Pediatric Urologist |
Bottom Line
Urologist is the definitive specialist. For acute presentations where torsion is possible, Emergency Medicine is the immediate first step - urology is called in urgently from there.
This is a shared conversation. Sign in to Orris to start your own chat.