Prostate cancer (may cause meta stasis in brain) Meckles diverticulum Hemmoroids Varicocoel Umphalocoel(umbilical hernia) Faecal fistula Cremasteric reflex Short notes on these topics for 5 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have sufficient information from the textbooks to write comprehensive short notes on all 7 topics. Let me compose the answer.
Short Notes for 5 Marks Each
1. Prostate Cancer (with Brain Metastasis)
Definition: Prostate cancer is the most common malignancy of the male genitourinary tract, arising from the glandular epithelium of the prostate, predominantly as adenocarcinoma.
Epidemiology: Most common in men over 50; risk increases with age, family history, and African descent.
Pathology:
- Graded by the Gleason scoring system (grades 1-5; combined score 2-10; higher = more aggressive)
- Most arise in the peripheral zone of the prostate
- Androgen-dependent tumor - testosterone and DHT drive growth
Clinical Features:
- Early: often asymptomatic; detected by elevated PSA (Prostate-Specific Antigen)
- Locally advanced: obstructive LUTS (hesitancy, poor stream, nocturia), hematuria, retention
- Metastatic: bone pain (osteosclerotic/osteoblastic lesions), pathological fractures, spinal cord compression, weight loss
Metastasis Pattern:
- Most common site: bone (osteoblastic) - lumbar spine, pelvis, femur
- Lymph nodes (obturator, iliac)
- Brain metastasis: Less common than breast or lung cancer, but occurs via:
- Hematogenous spread (arterial)
- Epidural extension to dura (dural metastasis is a recognized pattern)
- Batson's plexus (vertebral venous plexus allows direct spread to skull/brain)
- Breast and prostate cancer have a particular predilection for the dura, which may be the only intracranial site of metastasis in an otherwise treated patient. (Plum & Posner's Diagnosis and Treatment of Stupor and Coma)
Diagnosis:
- Digital rectal examination (DRE) - hard, irregular nodule
- Serum PSA (elevated)
- TRUS (transrectal ultrasound)-guided biopsy - confirmatory
- MRI prostate, bone scan, CT for staging
Treatment:
- Localized: radical prostatectomy or radiotherapy
- Metastatic: androgen deprivation therapy (LHRH agonists/antagonists), anti-androgens, chemotherapy (docetaxel), radium-223 for bone mets
- Brain mets: stereotactic radiosurgery, whole brain radiotherapy, dexamethasone for oedema
2. Meckel's Diverticulum
Definition: A true diverticulum of the ileum representing the most common remnant of the vitellointestinal (omphalomesenteric) duct. It contains all layers of the bowel wall.
Rule of 2s (Mnemonic):
- Present in 2% of the population
- 2 inches (5 cm) long
- 2 feet (60 cm) from the ileocaecal valve (on the antimesenteric border)
- 2 types of ectopic mucosa (gastric most common, also pancreatic)
- More common in males 2:1
- Usually presents in first 2 years of life if symptomatic
Pathology: About 20% contain heterotopic (ectopic) epithelium - most commonly gastric mucosa, which can secrete acid and cause peptic ulceration.
Clinical Presentations:
- Haemorrhage - Painless dark rectal bleeding or melaena from peptic ulceration in adjacent ileum due to ectopic gastric mucosa - commonest presentation in children
- Diverticulitis - Presents like appendicitis; perforation resembles perforated duodenal ulcer
- Intestinal obstruction - Via a fibrous band connecting the apex to the umbilicus causing volvulus or kinking
- Intussusception - Meckel's diverticulum acts as the lead point for ileoileal/ileocolic intussusception
- Perforation - Peritonitis
- Littre's hernia - Meckel's diverticulum found in an inguinal or femoral hernia sac
Diagnosis:
- Technetium-99m pertechnetate scan (Meckel's scan) - localizes ectopic gastric mucosa
- CT abdomen, mesenteric angiography for active bleeding
Treatment:
- Symptomatic: diverticulectomy or segmental ileal resection (preferred if base is wide or bleeding is involved, as the ulcer is usually adjacent to the diverticulum)
- Incidental finding at surgery: leave alone if wide-mouthed and not thickened; resect if in doubt
(Bailey and Love's Short Practice of Surgery, 28th Ed)
3. Haemorrhoids (Piles)
Definition: Haemorrhoids are abnormally enlarged and symptomatic vascular cushions (submucosal arteriovenous sinusoids) in the anal canal.
Anatomy: Normal anal cushions exist at 3, 7, and 11 o'clock positions (lithotomy position). The dentate line divides the anal canal into two zones:
- Above dentate line: lined by columnar epithelium, autonomic innervation (insensitive to pain), drains into portal system via superior rectal vein
- Below dentate line: lined by squamous epithelium, somatic innervation (very sensitive to pain), drains into systemic circulation via inferior rectal veins
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease)
Classification:
| Type | Location | Feature |
|---|---|---|
| Internal | Above dentate line | Painless; bleed bright red |
| External | Below dentate line | Painful; can thrombose |
| Mixed | Straddle dentate line | Features of both |
Degrees of Internal Haemorrhoids:
- 1st degree: Bleed only, do not prolapse
- 2nd degree: Prolapse on straining, reduce spontaneously
- 3rd degree: Prolapse on straining, require manual reduction
- 4th degree: Permanently prolapsed, irreducible
Predisposing Factors: Chronic constipation, straining, low fibre diet, pregnancy, portal hypertension, prolonged sitting
Symptoms: Painless bright red rectal bleeding (on toilet paper or dripping), prolapse, mucous discharge, pruritus ani, perianal soiling
Treatment:
- Conservative: High-fibre diet, increased fluids, stool softeners, topical agents
- Outpatient/office procedures: Rubber band ligation (most effective for 1st-3rd degree), injection sclerotherapy, infrared coagulation
- Surgical: Haemorrhoidectomy (Milligan-Morgan/Ferguson technique) for 3rd/4th degree; stapled haemorrhoidopexy
(Pfenninger and Fowler's Procedures for Primary Care)
4. Varicocele
Definition: Varicocele is an abnormal dilatation and tortuosity of the veins of the pampiniform plexus of the spermatic cord, due to retrograde venous blood flow through incompetent valves.
Epidemiology:
- Found in 15% of healthy young men
- Incidence in subfertile men: ~40% (most common surgically correctable cause of male infertility)
- 90% are left-sided (bilateral in up to 20% of subfertile men)
Why Left-Sided?
- Left internal spermatic vein is longer and joins the left renal vein at a right angle (rather than obliquely into the IVC like the right)
- Results in higher venous pressure transmitted to left spermatic cord - valvular incompetence - retrograde reflux
Appearance: "Bag of worms" - soft, irregular scrotal swelling above and behind the testis, more prominent on standing or Valsalva; disappears on lying down
Grade (WHO):
- Grade 1: Palpable only on Valsalva
- Grade 2: Palpable at rest
- Grade 3: Visible through scrotal skin
Effects on Fertility:
- Testicular atrophy, elevated intratesticular temperature (disrupts countercurrent heat exchange), decreased sperm count, motility, and morphology
- Pituitary-gonadal hormonal dysfunction
Diagnosis: Clinical examination; scrotal Doppler ultrasound confirms venous reflux
Note: A right-sided varicocele or a varicocele that does not reduce on lying down should raise suspicion of a retroperitoneal mass (e.g. renal cell carcinoma compressing the IVC or renal vein).
Treatment:
- Surgical: Varicocelectomy (retroperitoneal/inguinal ligation or subinguinal microsurgical approach)
- Radiological: Percutaneous embolization via right femoral vein - catheter advanced to left renal vein
(Smith and Tanagho's General Urology, 19th Ed; Gray's Anatomy for Students)
5. Omphalocele (Exomphalos / Umbilical Hernia)
Definition: Omphalocele (also called exomphalos) is a congenital anterior abdominal wall defect at the umbilicus in which abdominal contents herniate through the base of the umbilical cord, covered by a sac of fused amnion and peritoneum.
Incidence: 1.5 to 3 per 10,000 births; male predominance
Embryology: Results from failure of reduction of the physiological gut herniation that normally occurs by the 12th week of gestation. The umbilical cord inserts into the apex of the sac.
Pathology:
- Defect in the skin and linea alba at the umbilicus; surrounding abdominal musculature is intact
- Sac is avascular (composed of amnion + peritoneum); umbilical vessels radiate within the sac wall
- Small omphalocele: contains small bowel loops
- Large omphalocele: liver and spleen may be outside the abdominal cavity
Associated Anomalies (~75% of cases):
- Chromosomal: Trisomy 13 or 18
- Beckwith-Wiedemann syndrome (macroglossia, hepatomegaly, hypoglycaemia, gigantism)
- Pentalogy of Cantrell (omphalocele + sternal cleft + anterior diaphragmatic hernia + pericardial defect + cardiac defect)
- OEIS complex (Omphalocele, Exstrophy of bladder, Imperforate anus, Spinal defect)
- Cardiovascular, CNS, musculoskeletal anomalies
Distinction from Gastroschisis:
| Feature | Omphalocele | Gastroschisis |
|---|---|---|
| Sac present | Yes | No |
| Site | Umbilical | Para-umbilical (right) |
| Associated anomalies | Common (~75%) | Rare (<10%) |
| Bowel | Normal | Matted/thickened |
Diagnosis: Prenatal - elevated maternal serum AFP; antenatal ultrasound; karyotyping/amniocentesis
Treatment: All cases require surgical repair. Small defects - primary closure; large defects - staged closure using silo, skin flaps, or negative pressure wound therapy. Operative timing depends on size and associated anomalies.
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease)
6. Faecal Fistula
Definition: A faecal fistula is an abnormal communication between the intestinal lumen (colon or small bowel) and another epithelial-lined surface (skin, bladder, vagina, or another hollow viscus) through which faecal matter passes.
Classification:
- External (enterocutaneous): Between bowel and skin - most common type clinically managed
- Internal: Between two bowel segments (enterocolic, ileosigmoid) or bowel to other organs (colovesical, rectovaginal, gastrocolic)
Causes (Mnemonic - FRIENDS):
- Foreign body / Crohn's disease
- Radiation
- Inflammation / Infection
- Epithelialized tract
- Neoplasm / malignancy
- Distal obstruction
- Surgical anastomotic leak (most common postoperative cause)
Specific Faecal Fistula - Large Bowel Origin:
- May arise from leakage at a suture line or anastomosis postoperatively
- Early onset after surgery = high risk of peritonitis
- A simple fistula without peritoneal contamination can be managed like a colostomy and will usually close spontaneously provided there is no distal obstruction
Small Intestinal Fistula:
- Causes substantial loss of fluid and electrolytes
- Irritant digestive enzymes cause skin excoriation around the fistula site
- High-output fistula (>500 mL/day) leads to malnutrition and electrolyte imbalance
Conservative Management ("SNAP"):
- Skin care (wound care, stoma bag)
- Nutritional support - TPN (total parenteral nutrition), nil by mouth
- Antimicrobials if infection present; octreotide to reduce output
- Nasogastric drainage to rest bowel
Will close spontaneously if no distal obstruction, no neoplasm, no foreign body, no radiation, no short fistula tract, no epithelialization.
Surgical Management: Required if conservative management fails or if there is distal obstruction - resection of fistulated bowel segment with reanastomosis.
(Pye's Surgical Handicraft, 22nd Ed)
7. Cremasteric Reflex
Definition: The cremasteric reflex is a superficial (cutaneous) reflex in which stroking or light touch of the inner upper thigh causes ipsilateral contraction of the cremaster muscle, resulting in elevation of the ipsilateral testis.
Reflex Arc:
- Afferent limb: Femoral branch of the genitofemoral nerve (L1-L2) - stimulation of inner thigh skin
- Centre: Spinal cord segments L1-L2
- Efferent limb: Genital branch of the genitofemoral nerve - motor to cremaster muscle
Eliciting the Reflex:
- Patient supine; lightly stroke the inner upper thigh with a sharp object from above downwards
- Normal response: testis on the same side rises in the scrotum
Clinical Significance:
| Clinical Context | Significance |
|---|---|
| Testicular torsion | Absent cremasteric reflex on affected side - highly significant finding; most sensitive finding for excluding torsion is the presence of the reflex (sensitivity 73-96%) |
| Upper motor neuron lesion | Exaggerated (UMN lesion above L1) |
| Lower motor neuron lesion / L1-L2 root damage | Absent |
| Orchitis / epididymo-orchitis | May be absent |
| Normal | Present bilaterally in males |
(Tintinalli's Emergency Medicine; Campbell-Walsh-Wein Urology; Localization in Clinical Neurology, 8th Ed)
Important: Absence of the cremasteric reflex in a young male with acute scrotal pain is a red flag for testicular torsion and warrants immediate surgical exploration - do not wait for Doppler ultrasound if clinical suspicion is high.
The reflex is part of the bulbospongiosus reflex group, and return of sacral reflexes (including cremasteric) in the early hours after spinal cord injury suggests recovery of sacral cord function.
Sources: Bailey & Love's Surgery 28e | Smith & Tanagho's Urology 19e | Sleisenger & Fordtran's GI & Liver Disease | Pfenninger & Fowler's Procedures for Primary Care | Campbell-Walsh-Wein Urology | Pye's Surgical Handicraft 22e | Tintinalli's Emergency Medicine | Localization in Clinical Neurology 8e
Prostate cancer (may cause meta stasis in brain) Meckles diverticulum Hemmoroids Varicocoel Umphalocoel(umbilical hernia) Faecal fistula Cremasteric reflex Short notes on these topics for 5 marks wrt anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have excellent anatomical content from the textbooks. Let me compile the full anatomy-focused short notes.
Short Notes with Anatomy Focus (5 Marks Each)
1. Prostate Cancer - Anatomical Basis and Brain Metastasis
Anatomy of the Prostate:
- The prostate is a fibromuscular glandular organ situated in the lesser pelvis, inferior to the urinary bladder, surrounding the prostatic urethra
- Divided into zones (McNeal's zonal anatomy):
- Peripheral zone (~70%) - most common site of carcinoma (~70-80% of cancers)
- Central zone (~25%) - surrounds ejaculatory ducts
- Transitional zone (~5%) - site of benign prostatic hyperplasia
- Fibromuscular stroma - anterior surface
- Relations: Anteriorly - pubic symphysis (separated by retropubic space of Retzius); Posteriorly - rectum (separated by Denonvilliers' fascia); Superiorly - bladder neck; Inferiorly - urogenital diaphragm; Laterally - levator ani
- Blood supply: Inferior vesical artery (branch of internal iliac)
- Venous drainage: Prostatic venous plexus (Santorini's plexus) - drains into internal iliac veins; also communicates with Batson's vertebral venous plexus
- Lymphatic drainage: Internal iliac and obturator lymph nodes (primary); external iliac, presacral nodes
Why Brain Metastasis Occurs - Anatomical Pathway:
- Batson's paravertebral venous plexus: A valveless network of veins surrounding the vertebral column - communicates directly with the prostatic venous plexus. Increased intra-abdominal pressure (coughing, straining) can reverse blood flow through this plexus, carrying tumor cells retrograde up to the vertebrae, skull base, and intracranial dura
- Dural metastasis: Prostate cancer has a particular predilection for the dura mater - may spread from adjacent vertebral/skull metastases by direct extension
- Arterial hematogenous spread via pulmonary circulation - less common route to brain parenchyma
- Prostate cancer brain metastases are predominantly dural/subdural rather than intraparenchymal (unlike lung/breast cancer)
Anatomical Basis of Clinical Signs:
- DRE: prostate palpated through anterior rectal wall (posterior zone is accessible) - hard, irregular, nodular
- Ureteric obstruction from pelvic node enlargement
- Spinal cord compression from vertebral metastases via epidural spread
2. Meckel's Diverticulum - Anatomy
Embryological Origin:
- Meckel's diverticulum is the remnant of the vitellointestinal (omphalomesenteric/vitelline) duct - the connection between the midgut and the yolk sac during fetal development
- Normally, the duct obliterates by the 7th week of gestation
- Failure of obliteration of the ileal end results in Meckel's diverticulum
Anatomical Features - Rule of 2s:
- Present in 2% of the population
- 2 inches (5 cm) long
- Located 2 feet (60 cm) proximal to the ileocaecal valve
- On the antimesenteric border of the ileum (distinguishes it from a mesenteric duplication cyst)
- Contains all 3 layers of the bowel wall (true diverticulum)
- 20% contain ectopic tissue (most commonly gastric mucosa; also pancreatic, colonic)
- Has its own mesodiverticulum with a blood supply from a persistent vitelline artery (branch of the superior mesenteric artery)
Anatomical Relationships:
- The apex may be connected to the umbilicus by a fibrous cord (remnant of the proximal vitellointestinal duct) - this band can cause intestinal obstruction or volvulus
- If the duct persists as a patent channel to the umbilicus, it forms an umbilico-ileal fistula (omphalomesenteric fistula)
- Found in the right iliac fossa region (mimics appendicitis)
- When found in a hernia sac (inguinal/femoral) it is called Littre's hernia
Anatomical Basis of Complications:
- Ectopic gastric mucosa + own blood supply → peptic ulceration at the junction → bleeding
- Fibrous band from apex to umbilicus → internal herniation, volvulus → obstruction
- Diverticulum as lead point for intussusception
- Narrow-necked diverticulum → food trapping → diverticulitis (like appendicitis)
3. Haemorrhoids - Anatomy
Normal Anatomy of Anal Cushions:
- Haemorrhoids are submucosal cushions of arteriovenous sinusoids (not simply dilated veins) - they are a normal anatomical structure
- Located at 3, 7, and 11 o'clock positions in the anal canal (lithotomy position) - left lateral, right anterior, right posterior
- Composed of venules, arterioles, and smooth muscle fibers (the muscularis submucosae ani)
- Function: help seal the anal canal and maintain continence
Key Anatomical Landmark - Dentate (Pectinate) Line:
- Located ~2 cm from anal verge - the saw-toothed junction between endoderm (mucosa above) and ectoderm (squamous epithelium below)
- This line determines the type, symptoms, blood supply, lymph drainage, and nerve supply of haemorrhoids:
| Feature | Above Dentate Line (Internal) | Below Dentate Line (External) |
|---|---|---|
| Epithelium | Columnar/transitional mucosa | Squamous anoderm |
| Nerve supply | Autonomic (insensitive to pain) | Somatic (inferior rectal n.) - very sensitive |
| Arterial supply | Superior rectal a. (inferior mesenteric) | Inferior rectal a. (internal pudendal) |
| Venous drainage | Superior rectal vein → portal system | Inferior rectal vein → systemic |
| Lymphatics | Internal iliac nodes | Inguinal nodes |
Internal Haemorrhoids (above dentate line): Painless bleeding; classified by degree of prolapse
External Haemorrhoids (below dentate line): Painful, thrombosis, covered by anoderm
Mixed Haemorrhoids: Straddle the dentate line
Columns of Morgagni: 6-14 mucosal folds above the dentate line - the haemorrhoidal cushions lie within/under these folds
Portosystemic Communication: Internal haemorrhoids connect portal and systemic venous systems - relevant in portal hypertension (portosystemic anastomosis site)
Why External Haemorrhoids Hurt: Somatic innervation via the inferior rectal branch of the pudendal nerve (S2, S3, S4) - rubber band ligation must be placed >1 cm above the dentate line to avoid pain
(Schwartz's Principles of Surgery 11e; Sleisenger & Fordtran's GI & Liver Disease)
4. Varicocele - Anatomy
Definition: Abnormal dilatation and tortuosity of the veins of the pampiniform plexus of the spermatic cord due to incompetent valves causing retrograde venous flow.
Anatomy of the Pampiniform Plexus:
- A network of ~10 veins surrounding the testicular artery in the spermatic cord
- Functions as a countercurrent heat exchange mechanism - cools arterial blood before it enters the testis (maintains testicular temperature ~2-3°C below core body temperature, essential for spermatogenesis)
- Veins converge to form the testicular (internal spermatic) vein:
- Left testicular vein drains at a right angle into the left renal vein (~8-10 cm longer than the right)
- Right testicular vein drains obliquely into the inferior vena cava
Why Left-Sided Predominance (Anatomical Reasons):
- Left testicular vein is longer and joins the renal vein at 90° (no oblique valve-like effect)
- Higher hydrostatic pressure transmitted from the left renal vein
- The left testicular vein lacks competent valves in ~40% of men
- The left renal vein can be compressed between the aorta and superior mesenteric artery ("Nutcracker phenomenon")
- The left colon content and fecal mass may compress the left renal vein
Layers of Spermatic Cord (Containing the Plexus):
- Internal spermatic fascia (from transversalis fascia)
- Cremasteric muscle and fascia (from internal oblique) - site of the cremasteric reflex
- External spermatic fascia (from external oblique aponeurosis)
Anatomical Classification (Grade):
- Grade 1: Palpable only on Valsalva maneuver
- Grade 2: Palpable at rest without Valsalva
- Grade 3: Visible through scrotal skin - "bag of worms"
Secondary Varicocele: A right-sided varicocele or one not reducing on lying down suggests retroperitoneal pathology (e.g., renal cell carcinoma compressing the right gonadal vein or IVC)
Treatment Anatomy:
- Surgical ligation: At the internal inguinal ring (retroperitoneal) or subinguinal approach - ligate the internal spermatic veins while preserving the testicular artery
- Embolization: Catheter via right femoral vein → IVC → left renal vein → left internal spermatic vein
(Gray's Anatomy for Students; Smith & Tanagho's General Urology 19e; Rosen's Emergency Medicine)
5. Omphalocele (Exomphalos / Umbilical Hernia) - Anatomy
Definition: A congenital anomaly where abdominal viscera herniate through the base of the umbilical cord, covered by a sac of fused amnion and peritoneum (not skin).
Embryological Basis:
- Between weeks 6-10 of gestation, the midgut undergoes physiological herniation into the extraembryonic coelom (base of umbilical cord) as it elongates faster than the abdominal cavity can accommodate
- Normally, the gut returns to the abdominal cavity and the umbilical ring closes by week 12
- In omphalocele: failure of this reduction and closure - viscera remain outside the abdomen at birth
Anatomy of the Defect:
- Central defect in the linea alba and skin at the umbilicus
- Sac present: avascular, composed of fused layers of amnion (outer) and peritoneum (inner)
- Umbilical cord inserts into the apex of the sac - umbilical vessels radiate within the sac wall (critical: cord must be tied at least 5 cm from abdominal wall to avoid clamping an occult omphalocele)
- Surrounding abdominal musculature is intact
- Small omphalocele: contains small bowel loops
- Large omphalocele: may contain liver, spleen, stomach, small and large bowel
Distinction from Gastroschisis (Anatomical Differences):
| Feature | Omphalocele | Gastroschisis |
|---|---|---|
| Sac | Present (amnion + peritoneum) | Absent |
| Location | At umbilicus (central) | Para-umbilical (usually right) |
| Umbilical cord | Inserts into sac | Normal attachment; defect separate |
| Associated anomalies | ~75% | Rare |
| Bowel appearance | Normal (protected by sac) | Matted, inflamed, thickened |
Associated Syndromes (Anatomical Consequences of Failure of Fold Closure):
- Failure of cephalic fold: Sternal defect, anterior diaphragmatic hernia, cardiac defects
- Pentalogy of Cantrell: Omphalocele + sternal cleft + anterior diaphragmatic hernia + pericardial defect + congenital heart disease
- OEIS complex: Omphalocele + Exstrophy of bladder + Imperforate anus + Spinal defect
- Beckwith-Wiedemann syndrome: Macroglossia, organomegaly, hypoglycaemia
- Trisomy 13 or 18
Treatment Anatomy:
- Primary closure if small (abdominal cavity large enough)
- Staged closure with silastic silo for large defects - gradual reduction of contents into a cavity that must be stretched to accommodate them
- Avoid excessive intra-abdominal pressure (compromises diaphragm, renal perfusion)
(Sleisenger & Fordtran's GI & Liver Disease; Yamada's Textbook of Gastroenterology)
6. Faecal Fistula - Anatomy
Definition: An abnormal epithelial-lined communication between the intestinal lumen and an epithelial surface (skin, bladder, vagina, another segment of gut), through which faecal content passes.
Anatomical Classification:
By type of communication:
- External (Enterocutaneous): Bowel → skin surface. Subdivided:
- Colocutaneous (large bowel to skin)
- Enterocutaneous (small bowel to skin) - more serious, higher output
- Internal:
- Enteroenteric (between two bowel loops)
- Enterovesical (bowel to bladder - pneumaturia, faecaluria, recurrent UTI)
- Rectovaginal (between rectum and vagina - faecal passage per vaginum)
- Gastrocolic (between stomach and colon - faecalent vomiting)
Anatomical Basis of High vs Low Output:
- Small intestinal fistula: HIGH output (up to 1-2L/day); rich in digestive enzymes, bile, and electrolytes - causes severe skin excoriation and metabolic derangements (hyponatraemia, hypokalaemia, metabolic acidosis)
- Colonic fistula: LOW output; less fluid and enzyme loss; more likely to close spontaneously if no distal obstruction
Tract Anatomy:
- The fistula tract = a tube of granulation tissue lined by epithelium
- Short, straight, wide tract with no distal obstruction → more likely to heal spontaneously
- Long, epithelialized, narrow tract / irradiated tissue / malignancy / foreign body → will NOT close spontaneously
Conditions that PREVENT Spontaneous Closure (Mnemonic - FRIEND):
- Foreign body in tract
- Radiation damage (endarteritis obliterans)
- Inflammatory bowel disease (Crohn's) or Infection
- Epithelialization of tract
- Neoplasm
- Distal obstruction
Anatomical Considerations in Management:
- Fistulography (contrast injection into external opening) defines the anatomy: origin, length, associated collections
- CT fistulogram identifies associated abscesses, anastomotic leaks, bowel continuity
- A large bowel faecal fistula without peritoneal contamination can be managed conservatively like a colostomy - spontaneous closure expected if no distal obstruction
- TPN (bypasses enteral route entirely) reduces fistula output and allows bowel rest
(Pye's Surgical Handicraft 22e)
7. Cremasteric Reflex - Anatomy
Definition: A superficial somatic reflex in which stroking the inner upper thigh causes ipsilateral elevation of the testis due to contraction of the cremaster muscle.
Anatomy of the Cremaster Muscle:
- Arises from the internal oblique muscle and its aponeurosis, and partly from the transversus abdominis
- Forms the middle (second) layer of coverings of the spermatic cord and testis (between internal and external spermatic fasciae)
- Loops around the spermatic cord and testis in the scrotum
- Innervation: Genital branch of the genitofemoral nerve (L1/L2) - motor supply
- Function: Elevates the testis toward the inguinal canal (thermoregulation, protective response)
Reflex Arc - Complete Anatomy:
Stimulus: light touch / stroke of inner upper thigh skin
↓
Afferent: Femoral branch of genitofemoral nerve / ilioinguinal nerve (L1)
↓
Afferent fibres enter spinal cord at L1 (some sources: L1-L2)
↓
Interneuron at L1-L2 spinal segment
↓
Efferent: Genital branch of genitofemoral nerve (L1/L2)
↓
Motor end plate → Cremaster muscle contracts
↓
Response: Testis elevates ipsilaterally
(Note from Gray's Anatomy for Students: "Gently touching the skin at and around the anterior aspect of the superior part of the thigh stimulates the sensory fibers in the ilioinguinal nerve. These sensory fibers enter the spinal cord at level L1. At this level, the sensory fibers stimulate the motor fibers carried in the genital branch of the genitofemoral nerve, which results in contraction of the cremaster muscle and elevation of the testis.")
The Genitofemoral Nerve Anatomy:
- Arises from the ventral rami of L1 and L2
- Courses on the anterior surface of the psoas major muscle
- Divides near the inguinal ligament into:
- Femoral branch: Passes under inguinal ligament into femoral sheath → sensation to upper anterior thigh
- Genital branch: Passes through the deep inguinal ring into the inguinal canal → motor to cremaster; sensation to scrotum/labia majora
Clinical Significance:
| Situation | Cremasteric Reflex |
|---|---|
| Testicular torsion | Absent - most important sign; absence indicates no vascular supply to cremaster via genitofemoral nerve due to twist of cord |
| Normal child | Brisk (more active in children; diminishes with age) |
| L1-L2 cord lesion (LMN) | Absent |
| UMN lesion above L1 | Exaggerated |
| Genitofemoral neuralgia | Lost on the side of nerve injury |
| Spinal cord injury recovery | Early return of cremasteric reflex = evidence of sacral cord function returning |
Anatomical Note on Testicular Torsion: The spermatic cord twists within the tunica vaginalis (if the tunica is high-attached = "bell-clapper deformity"). Twisting strangulates the cremasteric vessels, removes the afferent stimulus pathway, and eliminates the reflex on the affected side. Absence of cremasteric reflex = torsion until proven otherwise.
(Gray's Anatomy for Students; Campbell-Walsh-Wein Urology; Localization in Clinical Neurology 8e; Tintinalli's Emergency Medicine)
Textbook Sources: Gray's Anatomy for Students | Schwartz's Principles of Surgery 11e | Smith & Tanagho's General Urology 19e | Sleisenger & Fordtran's GI & Liver Disease | Campbell-Walsh-Wein Urology | Pye's Surgical Handicraft 22e | Localization in Clinical Neurology 8e | Rosen's Emergency Medicine
Locking and unlocking of knee joint
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Excellent - I have detailed textbook content and the actual diagram. Now let me compile the comprehensive answer.
Locking and Unlocking of the Knee Joint
(Anatomy Short Note)
Introduction
The knee joint is the largest synovial joint in the body. Unlike most joints, it possesses a unique mechanism called the "screw-home" or locking mechanism that allows the joint to be stabilized in full extension with minimal muscular effort - an energy-efficient adaptation for prolonged standing. This is followed by an equally important unlocking mechanism to initiate flexion.
Anatomical Basis - Why Locking is Possible
To understand locking and unlocking, three anatomical features must be appreciated:
1. Asymmetry of the Femoral Condyles
- The medial femoral condyle is longer (anteroposteriorly) and more curved than the lateral condyle
- The articular surface of the medial condyle extends further anteriorly and has a smaller radius of curvature
- This asymmetry means that during extension, the lateral condyle completes its rolling/gliding earlier than the medial condyle - forcing the femur to rotate medially to "use up" the remaining articular surface of the medial condyle
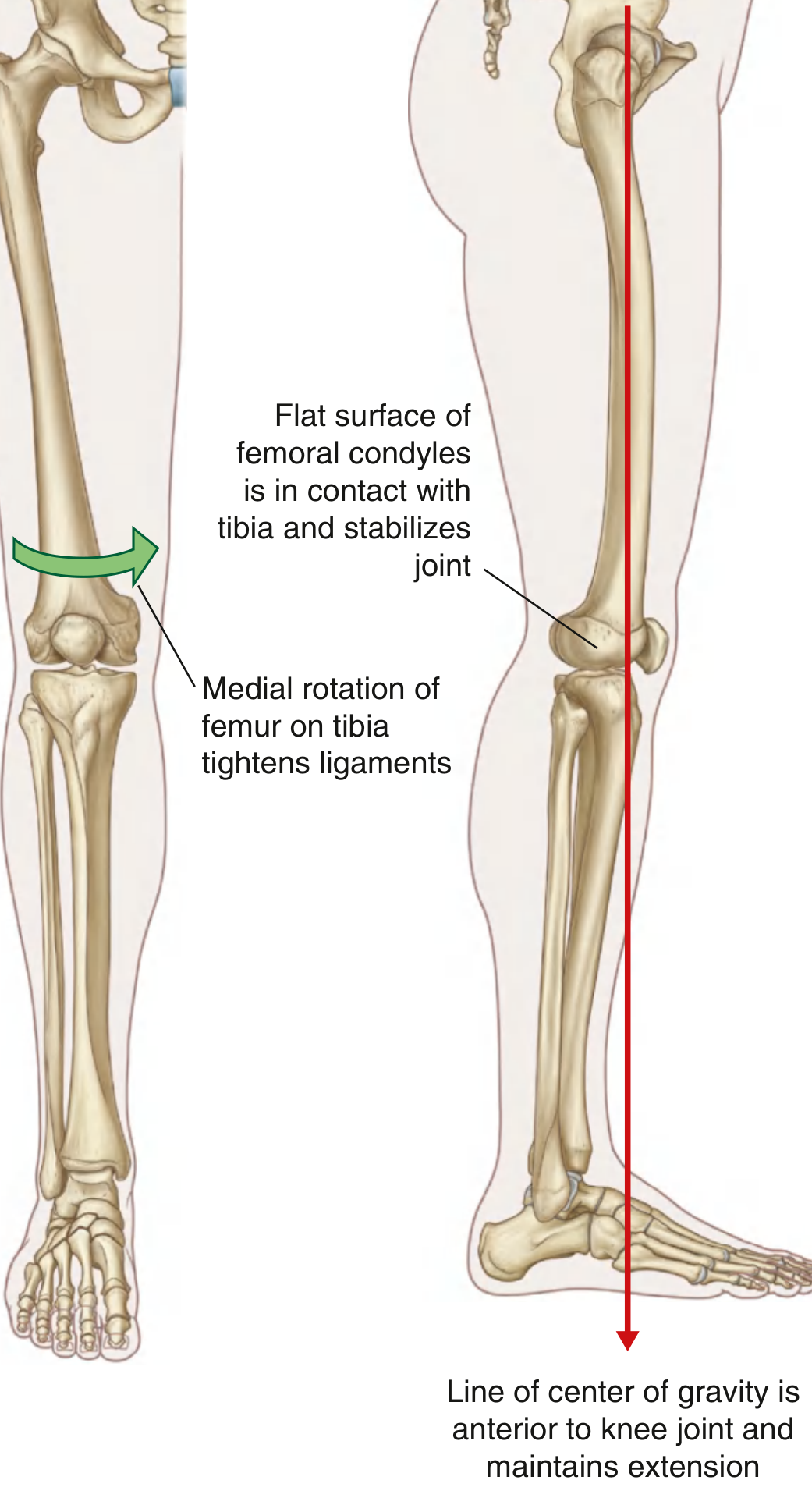
2. Shape of Articular Surfaces Changes During Extension
- In flexion: The femur rests on the curved, rounded posterior aspects of the femoral condyles (smaller contact area = less stable)
- In full extension: The articular surfaces shift to the broad, flat inferior aspects of the femoral condyles (larger contact area = more stable)
- This transformation makes the joint surfaces maximally congruent and stable at full extension
3. Cruciate Ligaments
- The PCL is more vertically oriented and acts as the axis of rotation of the knee
- It guides the screw-home mechanism during terminal extension
- Both cruciate ligaments tighten progressively as the knee reaches full extension
LOCKING OF THE KNEE ("Screw-Home Mechanism")
Definition: The automatic medial rotation of the femur on the fixed tibia (or lateral rotation of tibia on fixed femur in open-chain movement) that occurs during the last 15° of full extension, locking the knee into a stable, close-packed position.
Mechanism - Step by Step:
Weight-bearing (closed kinetic chain) - e.g., rising from sitting:
- As the knee approaches full extension, the lateral femoral condyle finishes its arc of rolling first (shorter condyle)
- The medial femoral condyle still has residual articular surface to cover
- This forces the femur to rotate medially (internally) on the fixed tibia to complete extension
- Equivalently stated: the tibia rotates laterally (externally) ~10° relative to the femur in the last 15° of extension
Open kinetic chain (e.g., swinging leg):
- The tibia rotates externally on the fixed femur as the knee reaches full extension
What Happens at Full Lock:
- The broad, flat inferior femoral condyle surfaces are now fully in contact with the tibial plateau - maximum bony congruence
- All ligaments tighten simultaneously:
- Both collateral ligaments (medial and lateral) become taut
- Both cruciate ligaments become taut (particularly the ACL and PCL)
- The posterior capsule tightens
- The menisci are compressed into stable positions
- The knee is now in its close-packed position - most stable, no rotation possible
- The body's center of gravity falls anterior to the knee joint, so gravity itself helps maintain extension (no quadriceps effort needed in normal standing)
Result: The knee is "locked" - held in full extension passively, with minimal quadriceps activity. This is why prolonged standing is less tiring than prolonged squatting.
UNLOCKING OF THE KNEE
Definition: The reversal of the screw-home mechanism - lateral rotation of the femur on the fixed tibia (or medial rotation of tibia on femur) - that must occur before flexion can begin.
The Muscle Responsible: POPLITEUS
"The popliteus muscle unlocks the knee by initiating lateral rotation of the femur on the tibia." - Gray's Anatomy for Students
Popliteus - Anatomy:
| Feature | Detail |
|---|---|
| Shape | Flat, triangular |
| Origin | Lateral femoral condyle (and lateral meniscus via popliteomeniscal fascicles) |
| Insertion | Posterior surface of proximal tibia (above soleal line) |
| Nerve supply | Tibial nerve (L4, L5, S1) |
| Location | Floor of the popliteal fossa; smallest, most superior deep posterior leg muscle |
Popliteus Actions:
-
In weight-bearing (closed kinetic chain):
- Tibia is fixed (foot on ground)
- Popliteus pulls the lateral femoral condyle posteriorly → laterally rotates the femur on the tibia
- This reverses the screw-home mechanism and unlocks the knee
- Allows flexion to begin
-
In open kinetic chain:
- Femur is fixed
- Popliteus medially rotates the tibia on the femur to unlock
-
Stabilizing role:
- Resists lateral (external) rotation of the tibia on the femur during activity
- Prevents forward displacement of femur on tibia
- Pulls the lateral meniscus posteriorly during flexion (preventing it from being trapped between the condyles)
How Unlocking Proceeds:
- Popliteus contracts → laterally rotates femur ~5° on fixed tibia
- Ligaments (collaterals, cruciates, capsule) slacken/unwind
- Bony congruence reduces (curved posterior condyles re-engage)
- The knee moves out of close-packed position
- Flexion can now proceed - driven by hamstrings (biceps femoris, semimembranosus, semitendinosus)
Summary Table
| Feature | Locking | Unlocking |
|---|---|---|
| Movement | Medial rotation of femur on tibia (or lateral rotation of tibia on femur) | Lateral rotation of femur on tibia (or medial rotation of tibia on femur) |
| When | Last 15° of extension | Start of flexion from full extension |
| Muscle responsible | Passive - driven by condylar geometry + cruciate ligaments | Popliteus (active) |
| Nerve | - | Tibial nerve (L4-S1) |
| Ligament state | All ligaments taut | Ligaments slacken |
| Condyle surface | Flat inferior surface (maximum contact) | Curved posterior surface (less contact) |
| Result | Joint stable; no muscle effort needed | Flexion becomes possible |
Clinical Importance
- True locking of the knee (inability to fully extend) in clinical practice is caused by a torn meniscus (bucket-handle tear) or loose body acting as a mechanical block - distinct from the anatomical "screw-home" locking
- Popliteus injury: Causes posterior knee pain, particularly on downhill walking; may lead to posterolateral instability
- PCL injury: Disrupts the axis of rotation and impairs the screw-home mechanism, leading to rotatory instability
- Bell-clapper deformity / testicular torsion analogy: The screw-home is a rotatory tightening - any disruption of the rotatory sequence (e.g., ligament tear) means the knee cannot lock securely
Sources: Gray's Anatomy for Students (Locking Mechanism, Popliteus sections) | Miller's Review of Orthopaedics 9e (Knee Biomechanics) | Campbell's Operative Orthopaedics 15e (Biomechanics, PCL and screw-home)
This is a shared conversation. Sign in to Orris to start your own chat.